Continuing Education Activity
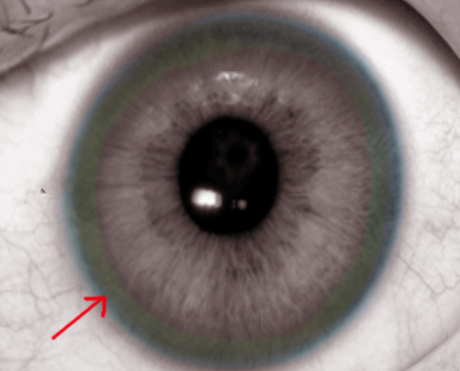
Kayser–Fleischer (KF) rings are a common ophthalmologic finding in patients with Wilson disease. Initially thought to be due to the accumulation of silver, they were first demonstrated to contain copper in 1934. KF rings are seen in most of the patients with neurologic involvement from Wilson disease. These rings are caused by the deposition of excess copper on the inner surface of the cornea in the Descemet membrane. A slit lamp examination is mandatory to make a diagnosis of KF rings particularly in the early stages unless the rings are visible to the naked eye in conditions of severe copper overload. Kayser–Fleischer rings do not cause any impairment of vision but disappear with treatment and reappear with disease progression. KF rings are not specific to Wilson disease alone, they are also seen in other chronic cholestatic disorders such as primary biliary cholangitis and children with neonatal cholestasis. This activity reviews the evaluation and treatment of a patient with a Kayser-Fleischer ring and addresses the role of the interprofessional team in managing this condition.
Objectives:
- Identify diseases commonly associated with a Kayser-Fleischer ring.
- Summarize the expected physical exam findings expected in a patient with a Kayser-Fleischer ring.
- Outline the treatment options available in a patient with a Kayser-Fleischer ring.
- Review the evaluation and treatment of a patient with a Kayser-Fleischer ring and demonstrate the role of the interprofessional team in managing this condition.