Continuing Education Activity
Pes cavus is an orthopedic condition that manifests in both children and adults. It is defined primarily by the elevation of the longitudinal arch of the foot: a high arched foot. The cavovarus foot is the primary manifestation of cavus and results in pathological malposition of the foot, usually as a result of underlying muscular imbalances as a result of neurologic conditions. This activity reviews the evaluation and management of patients with pes cavus conditions by an interprofessional team.
Objectives:
- Identify the etiology of pes cavus in the different populations it is likely to occur.
- Describe the evaluation of pes cavus conditions.
- Outline the management options available for pes cavus.
- Review interprofessional team strategies for improving care coordination and communication to advance pes cavus and improve outcomes.
Introduction
Pes cavus is an orthopedic condition that manifests in both children and adults. Pes cavus and pes cavovarus are often used interchangeably as the most common manifestation of the cavus foot is the cavovarus presentation. Pes cavus is a deformity that is typically characterized by cavus (elevation of the longitudinal plantar arch of the foot), plantar flexion of the first ray, forefoot pronation, and valgus, hindfoot varus, and forefoot adduction. Pes cavus is frequently a manifestation of an underlying neurological process, but there has been literature that discusses a subset of patients in whom a more subtle form of the cavus foot may present without an underlying disease process.[1][2][3] With the understanding that most cases are related to these underlying neurological processes, it becomes necessary to not only understand the intricacies of the care of the foot deformity itself but to ensure that adequate patient history, family history, clinical exam, radiographic exam, and other necessary testing is performed to ensure that the clinician has adequately diagnosed the underlying cause before initiation of treatment.
Anatomy
The cavovarus foot can be the result of forefoot driven pathology (a flexed first ray), a deformity of the hindfoot, or some combination of both pathologies.[4] The foot normally forms a tripod with the first metatarsal head, calcaneus, and fifth metatarsal head forming the three points of contact with the ground. In the cavus foot, flexion of one element of the tripod, the first ray, leads to tilting and overload of the other two elements.[5]
Forefoot driven pes cavus is most often caused by neurological diseases and is the result of muscular imbalances. A weak tibialis anterior, intrinsic foot muscles, and peroneus brevis are overpowered by a stronger peroneus longus and posterior tibialis. Later these muscles may also weaken but remain in a state of contracture, producing the same effect. The attachment of the peroneus longus at the metatarsals and medial cuneiform results in plantar flexion of the first ray and forefoot pronation. When a foot with fixed forefoot pronation bears weight, the hindfoot is forced to counter-correct into supination, or varus, in order to restore the tripod.[5]
As the deformity develops, the Achilles tendon may eventually act as an invertor of the foot and will shorten over time.[4] The unopposed contracture of the tibialis posterior and peroneus longus will lead to subtalar joint inversion.[6] In gait, the cavovarus foot demonstrates a compensatory heel varus, a locked midfoot, and a reduction of the flexible phase and decreased shock absorption as a result of plantar fascial tightening.[7][4] Typically the arch of the foot will change shape during the gait cycle, and the shock absorption of the midstance phase is negatively affected by the tightening of the plantar fascia leading to decreased shock absorption.[8]
Hindfoot driven cavovarus deformity is commonly the result of trauma.[9] The causes may include malunited pilon fractures and resultant varus angulation of the distal tibial articular surface, malunion of talar neck or calcaneal fractures, or longstanding ankle or subtalar joint instability.[4] The varus deformity will result over time as an attempt to obtain a plantigrade foot by compensation through the subtalar joint.[8] The compensation by the subtalar joint for ankle joint deformity can be explained by the anatomy of the subtalar joint. A healthy subtalar joint can tilt away from the deformity and compensate somewhat for the primary ankle varus that often results from the traumatic etiologies listed above. This will result in an overall balanced hindfoot. A study of 226 subjects with ankle osteoarthritis found the compensation of the subtalar joint in greater than 50% of varus ankle osteoarthritis cases.[10] This prolonged compensation may lead to a progressive and fixed deformity over time.
Cock-up deformities are also common at the metatarsophalangeal joints (MTP).[6][4] Overpull of the flexor digitorum longus is a contributing factor, as is the shortening and fibrosis of the plantar fascia. As the pressure under the metatarsal heads increases a result of this cock-up deformity, the MTP joints can eventually dislocate.[4] This increased pressure is independent of the root cause of the cavovarus foot and can be of particular concern in patients with metabolic diseases such as diabetes mellitus due to the increased foot pressure leading to concerns for ulceration.[6]
Natural History
Prognosis highly depends on deformity severity, underlying etiology, & age at presentation. The deformity is typically slow to develop and begins before puberty. In children, the deformity is initially compensated but may become more rigid over time, leading to possible alterations in bone growth, effects on the further development of bones, and alteration of the shape and morphology of the developing foot.[11] The most common cause of pes cavus is the hereditary motor and sensory neuropathies (HMSNs), the most common subtype being Charcot-Marie-Tooth (CMT) disease. CMT is a progressive degeneration of peripheral nerve myelin with decreased motor nerve conduction. Deformities typically worsen, and surgical treatment is often part of the treatment algorithm for these patients to prevent progression to a fixed deformity.[12]
The lateral soft tissue structures may suffer from overload leading to instability in both the typical pes cavovarus.[13] and the subtle cavus foot, or "underpronator." [14] Untreated long-term lateral ankle instability has been documented as a cause of advanced arthritis of the ankle joint.[15] Anterolateral ankle instability may also result.[2]
Patterns of Spread
The pattern of the spread of pes cavus is dependent on the underlying etiology.
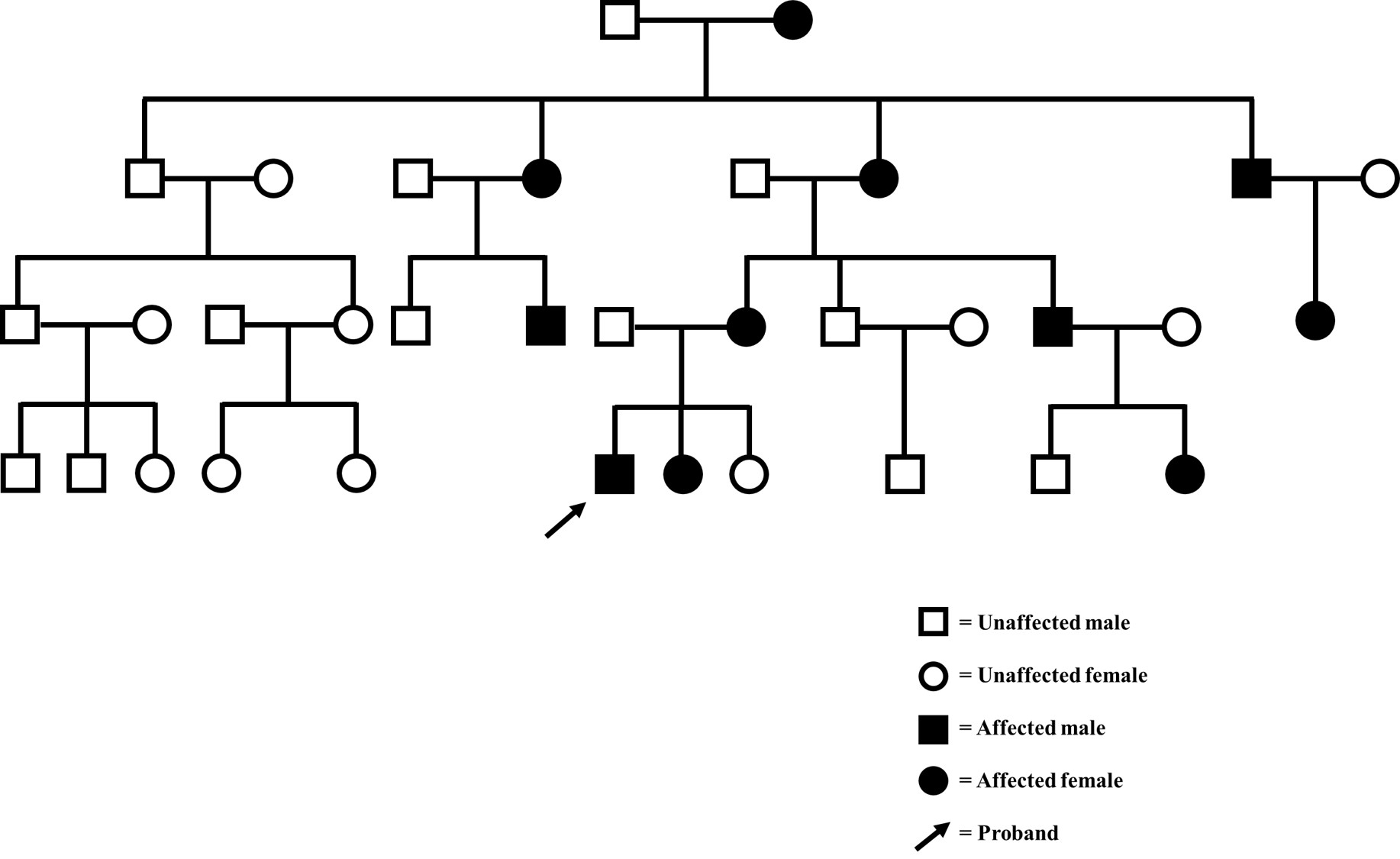
HMSNs subtypes have a heritable transmission in autosomal-dominant, autosomal recessive, and x-linked recessive patterns.[1] The subtle cavus foot that is more commonly found in adults without underlying neurological disorders is also probably inherited, with a currently unclear pattern.[2]
Etiology
Pes cavus is seen in both adult and pediatric populations. When it is found to be bilateral, it is often from a hereditary or congenital source. A unilateral presentation is more typical for post-traumatic conditions.[4] In the absence of such a cause, a unilateral presentation of pea cavus mandates MRI of the brain and spinal cord, to exclude treatable progressive lesions such as a brain tumor or, during growth, a tethered spinal cord. There are four primary causes of the cavovarus foot.[4][1][8][16]
- Neurologic conditions: hereditary motor and sensory neuropathies (HMSN), cerebral palsy, post-stroke symptoms, anterior horn disease, spinal cord lesions, poliomyelitis, myelomeningocele, polyneuritic syndromes, Parkinson disease, Huntington chorea, Friedreich ataxia, amyotrophic lateral sclerosis, leprosy, Roussy-Levy syndrome, Stumpell-Lorrain disease, Pierre-Marie heredotaxy
- Traumatic: compartment syndrome, talar neck malunion, peroneal nerve injury, knee dislocation, scar tissue, burns, vascular lesions, hindfoot instability, tibial fractures (distal), or calcaneal malunion
- Post-traumatic bone deformities or ligamentous imbalance or instability often lead to a deformity in this post-traumatic setting.
- Untreated or undertreated clubfoot
- Idiopathic or other causes include tarsal coalition, rheumatoid arthritis, ankle osteoarthritis, plantar fibromatosis, varus subtalar joint axis, diabetic foot syndrome. The subtle cavus foot is often categorized within the idiopathic group.
Epidemiology
The true incidence of the cavus foot is unknown in the population at large, possibly due to the somewhat loose definition, but attempts have been made to define the prevalence in some groups. Studies give different figures according to their geographic location, the pattern of referrals to their practice and healthcare system, and the definition of cavus used. In one study, a patient with bilateral cavovarus feet has a 78% chance of having CMT, and those that have a family history of cavovarus feet have a 91% chance of having CMT.[17] A study of 1846 healthy adult individuals from southern India without any underlying neurological condition found a prevalence of 10% of pes cavus.[18] Another study evaluating diabetic males found a roughly 25% prevalence of cavus deformities.[6] A review of a pedorthotist who fabricated foot orthoses for eight foot and ankle surgeons revealed that over half of all patients were fitted with a cavus foot orthosis.[2] In another study of patients presenting for evaluation of symptomatic pes cavus, roughly two-thirds had an underlying neurological abnormality.[19] There is no known difference between the sexes for the presentation of the cavus foot.
Pathophysiology
The pathophysiology and pathoanatomy result from the site of the deformity, as noted in the anatomy subheading. The critical lesion in forefoot driven pes cavus is thought to be the unopposed contraction (or passive contracture) of the peroneus longus and resultant plantarflexion of the first ray. Hindfoot driven pes cavus is the result of varus malalignment of the hindfoot, often in a compensatory pattern. Pes calcaneocavus, where the hindfoot is dorsiflexed and the forefoot plantarflexed in a compensatory fashion, is caused by calf weakness and is classically found after polio. Finally, the spasticity caused by cerebral palsy can result in a variety of foot shapes, including various types of cavus.
History and Physical
A complete history and physical examination can often establish an underlying diagnosis.
History
Patients may complain of frequent ankle sprains, arch pain, and occasionally knee pain.[8] Foot pain is a frequent presenting symptom and is usually the result of the increased stress on one part of the foot as a result of the deformity. Common sites of pain are in the heel, the cuboid region, other portions of the lateral foot, and the first metatarsal head.[1] Other complaints may include shoes that do not fit anymore or wear out quickly, pain over bony prominences, and painful calluses (frequently under the first and fifth metatarsal heads).[8]
A family history of similar deformities may indicate a hereditary cause, and care should be taken to obtain a thorough family history.[20] Sudden spontaneous development of unilateral pes cavus with other neurologic symptoms may suggest a spinal lesion, and further workup should be initiated.[1]
The patient history for the subtle cavus foot is more consistent with long-standing and milder symptoms or chronic lateral foot pain and/or stress fractures.[3] It may also present as ankle instability or peroneal tendon pathology.
Physical Examination
A thorough orthopedic foot and ankle exam should be performed, and the patient should be examined walking and standing. Overall limb alignment should be evaluated. The shape and symmetry of the feet should be noted from all angles. The heel cord and triceps surae should be evaluated for tightness with both flexion and extension of the knee. The function and strength of all muscles in the lower extremity should be evaluated. The motion of the subtalar joint can provide additional information towards a diagnosis, a more fixed and rigid subtalar joint pointing to etiologies such as a coalition or a primary hindfoot driven cavovarus.[8] The skin and soft tissues should be evaluated for lesions and callosities.[8] A detailed neurological exam should also include reflexes, sensation, proprioception, and vibratory exams.[1]
The Coleman block test is a critical portion of the examination as one of the major goals of the physical exam is to determine the rigidity of the deformity.[12] The test was first described in 1977 and has remained an essential tool for the evaluation of the cavus foot.[21]
The Coleman block test is performed by placing a roughly 1-inch block (or 2.5 cm) or a book under the lateral side of the forefoot and heel. The first metatarsal head should hang off the edge of the block, thus removing its effects on the tripod. The examiner must then evaluate the hindfoot to determine if removing the first metatarsal’s deforming effects has allowed the hindfoot to correct from varus to valgus. If the hindfoot varus does not correct, the deformity is rigid and fixed, and this has different surgical implications than a flexible deformity. If the block test restores hindfoot valgus, then the deformity is flexible and driven by the forefoot.
Evaluation should include palpation along the lesser metatarsals and fifth metatarsal for signs and symptoms of stress fractures. Examination of the ankle for stability, joint tenderness, and peroneal tendinopathy should also be undertaken. Anterior ankle pain is common due to impingement of the relatively dorsiflexed talus.
Further detailed examination of the entire patient should include a physical exam of the patient’s spine to evaluate for deformities such as scoliosis, which is suggestive of CMT, and hairy patches or dimples which might be suggestive of spinal dysraphism. The exam should also include a neurologic evaluation consisting of reflexes, sensation, and vibratory sensation.
A major clinical sign of the subtle cavus foot is the “peek-a-boo” heel first described by Manoli et al. in 1993.[22] It has been described as the ability to see the heel pad easily from the front with the patient standing and both feet pointing ahead. In the normal foot, the heel pad should not be visible when viewed from the front due to the natural valgus alignment of the hindfoot.[2]
Evaluation
Plain film radiographs are the first investigation for the cavus foot. Recommended views include[8]:
Weight-bearing views of the foot and ankle
Calcaneal axial view (others have suggested that the Colby view may be more helpful in the evaluation of hindfoot alignment).[23]
A standard evaluation for fractures, dislocations, and degenerative changes should begin any radiographic assessment, other specific lines, geographic measurements, and angles can help the clinician determine the relative position of the foot to its other components. Some of the more commonly used examples are listed below:
One can determine the presence of cavus by evaluating the relative position of the inferior aspect of the medial cuneiform and the fifth metatarsal base on a lateral x-ray of the foot. When the 5th metatarsal base is closer to the floor, the foot is in cavus.
Meary’s line (a line measured along the long axis of the talus and first metatarsal) is normally zero, but in the cavus foot, the first metatarsal is plantarflexed, increasing the angle. A mild cavus foot may have a Meary’s angle of five to ten degrees, with severe cavus feet having angles greater than twenty degrees.[24]
A Hibb angle may also be used. This is a measurement between the longitudinal axis of the calcaneus and first metatarsal. Values in normal feet are generally less than 45 degrees. In patients in pes cavus deformities, the angle is often greater than 90 degrees.[25]
A talocalcaneal angle on the AP radiograph will show a divergent talus and calcaneus in a normal foot with an angle of twenty to forty degrees. When the angle is decreased, this indicates that the talus and calcaneus are more parallel, and the foot is in cavus.[8]
The Djian-Annonier angle (the angle of the medial arch) is widely used in France and is found to be less than one-hundred and twenty degrees in the cavus foot.[12] This angle is measured from where the calcaneus rests against the ground, to the talonavicular joint at the apex and to the medial sesamoid where it contacts the ground again.
Other Imaging:
Computed tomography (CT) scans may also be performed to allow for evaluation of the joints for arthrosis for surgical planning and a complete evaluation of the hindfoot position.[1]
Magnetic resonance imaging has been described for the evaluation of the lateral ligamentous complex, peroneal tendon pathology, osteochondral lesions, and evaluation of fifth metatarsal base fractures.[26]
In cases of suspected HMSNs, patients may benefit from evaluation by a neurologist for possible electromyogram and/or genetic testing.[26]
Unilateral pes cavus without obvious explanation should prompt MRI of the brain and spinal cord.
Treatment / Management
Non-Operative
Standard non-operative interventions include activity modification, anti-inflammatory medications, simple accommodative shoes, and custom orthoses. Patients with milder deformities and milder symptoms may be successfully treated using custom orthoses, with the goal being realignment of the hindfoot and to offload the lateral foot.[12] For the flexible cavus foot lateral hindfoot posting, a recess for the first metatarsal head and heel pad are the main points in custom orthoses.[27] Attempts may be made to manage more rigid and severe deformities with more restrictive orthoses, such as an Arizona brace.[26] In a randomized controlled trial of 154 patients with painful pes cavus, patients were randomized to custom orthoses or sham orthoses, the patients in the custom orthosis group reported statistically significant improvements in foot pain scores, foot function scores, and quality of life metrics when compared to the sham group.[28] Other small patient cohorts have also had success with delay or prevention of surgical treatment with pes cavus as the result of childhood neurological disorders. d'Astorg et al. had a cohort of 35 feet treated with nocturnal splinting or casting. They were able to delay surgery by an average of 4.5 years in the 11 feet that progressed despite non-operative management. All other feet in the cohort had avoided surgery at last follow-up at 4.5 years.[29]
Medications for the underlying spasticity have been used as well and include baclofen, dantrolene, and diazepam. Botulinum toxin blocks have also been used.[8] A recent randomized, single-blinded trial of botulinum toxin A in children with CMT determined that, although safe and well-tolerated, there was no significant decrease in the progression of the cavus deformity.[30]
Gastrocnemius stretching programs are also used to help prevent contractures. A single patient 12 weeks lower extremity strengthening program resulted in an increase in dorsiflexion strength by 56% to 72% and plantarflexion strength by 15% to 20%. Functional outcomes also improved for the patient.[31] Thus strengthening and stretching remain reasonable short term options, with the understanding that no strong literature exists with regards to change in long-term outcomes or avoidance of further procedures with non-operative modalities.
Operative
Many authors will advocate for early operative intervention due to the progressive deformity and muscular imbalances that are present prior to unsalvageable fixed deformities with degenerative joints.[1][24][7] In-depth algorithms are available from several sources based upon the complete clinical picture of the patient.[26][12][3][1]
Options for surgical intervention include numerous in-phase tendon transfers, out-of-phase tendon transfers, tendon lengthenings, calcaneal osteotomies, talar neck osteotomies, dorsiflexion osteotomy of the first ray, midfoot osteotomies, and arthodeses for joints in which degenerative changes have occurred. The precise combination of procedures used depends greatly on each patient's deformity and the surgeon's experience and philosophy.
Commonly performed procedures are listed as examples below:
With regards to tendon transfers, in the flexible cavus foot, the posterior tibial tendon may be transferred to the dorsum of the foot to augment the weak tibialis anterior. The peroneus longus may also be transferred to the peroneus brevis to reduce the pull on the first ray and to assist with the eversion of the foot.[8][26]
Soft tissue releases such as gastrocnemius recession or heel cord lengthening are often advocated in the setting of hindfoot equinus.[1] However, many surgeons believe the Achilles should be left intact, and the tension in it reduced by correcting the position of the hindfoot with osteotomies or fusions.
Osseous alignment procedures commonly consist of a first metatarsal dorsiflexion osteotomy for fore-foot driven cavus. For hindfoot drive varus, a lateralizing calcaneal osteotomy is commonly used to recreate native hindfoot valgus and realign the pull of the gastrocnemius.[8] Plantar fascia release may be part of the treatment algorithm as well to allow for further dorsiflexion of the first ray.[1][32]
Joint sparing osteotomies are preferred in patients without advanced degenerative disease. However, even in those patients in which arthrodesis is performed, the balancing of the muscular forces is recommended to avoid fusion failure.[1] Triple arthrodesis remains a surgical option but is generally viewed as a salvage operation as most patients who underwent this procedure as teenagers had significant adjacent joint disease by their thirties.[7][33]
Surgical treatment of the subtle cavus foot often occurs while the surgeon is addressing other pathologies such as lateral overload symptoms, stress fractures, or lateral ankle instability.[2] Forefoot correction through tendon transfer and first metatarsal dorsiflexion osteotomy is typically the first step, followed by a lateralizing calcaneal osteotomy. Plantar fascial release is not a common part of the treatment algorithm for the subtle cavus foot.[3]
Differential Diagnosis
The problem often lies less with determining that the foot is in cavus and rather in adequately diagnosing the underlying etiology of the cavus foot to help determine the optimal treatment for the patient. Pes cavus may be a presentation of a great number of different diseases and conditions that must be differentiated from each other. The clinician should be aware that the majority of patients that present with significant pes cavus have an underlying disorder.
Bearing that in mind, the cavovarus foot must be differentiated from the equinovarus foot, the foot may appear somewhat similar, but the equinovarus foot may result from different causes and will require a different surgical algorithm.[34]
- Charcot–Marie–Tooth disease
- Congenital hypomyelinating neuropathy
- Dejerine–Sottas neuropathy
- Distal hereditary motor neuropathies
Prognosis
Prognosis is, once again, dependent on the underlying disease condition that led to the cavovarus foot. Some disease conditions lead to progressive deformity such as CMT, other sources of cavovarus foot are relatively nonprogressive, such as poliomyelitis.[7] Treatment and prognosis for these conditions vary. CMT type 1 has a younger onset (in the teens) and earlier progression than CMT type 2 (onset in the third and fourth decades). The hands are affected later than the feet, and this can obviously add to disability. Rare types of CMT can result in more additional neurological problems affecting the cranial nerves.
Complications
A delay in diagnosis or prolonged usage of orthotics despite worsening deformity can eventually lead to a fixed and rigid deformity that may only be salvaged by arthrodesis.[7][24][1]
There is a risk of tendon transfer or stabilization failure without correction of the underlying osseous deformity or with incomplete correction.[35] When the neurology is progressive (as in CMT), then no surgical procedure can completely guard against recurrence.
An arthrodesis is a surgical option as well, but the results have been less promising in the long term, and adjacent joint disease is a known complication in foot and ankle surgery. A study by Ward et al. evaluated long term results of surgical intervention in patients with CMT and a flexible cavovarus foot. Their intervention included plantar fasciotomy, transfer of the peroneus longus to brevis, and a first metatarsal osteotomy. The average age of the study group at the time of surgery was 15.5 years, with an average follow-up time of 41.5 years. The reconstruction cohort developed less degenerative changes in the foot and ankle and had a lower incidence of re-operation compared to historic CMT cohorts treated primarily with a triple arthrodesis.[36] Saltzman et al.’s 25 and 44-year follow-up study of triple arthrodesis performed for a variety of foot deformities demonstrated that while most patients were overall satisfied with their procedure that at first follow-up, 31 percent had adjacent joint degeneration and by 44-year follow-up, all patients had degenerative joint disease.[37]
Complications may also result from the subtle cavus foot and may include ankle instability, varus ankle arthrosis, peroneal tendon disorders, lateral foot overload including 5th metatarsal stress fractures, anteromedial ankle impingement syndromes, plantar fasciitis, claw toe deformities, and pathology may extend proximally with knee derangement as a result.[8]
Cavovarus alignment and chronic ankle instability are also risk factors for the development of ankle joint arthritis.[35] The cavovarus alignment has been shown to increase medial joint pressure in cadaver studies, with the same study revealing an improvement in the abnormal contact pressures with lateralizing calcaneal osteotomy.[38]
Deterrence and Patient Education
Patient and caregiver education should be focused on the role of physical therapy and orthosis wear for more mild conditions with the understanding that these nonoperative modalities may not be able to prevent progression of the cavovarus deformity definitively and that subsequent procedures may be necessary to allow for a plantigrade foot.
As with many orthopedic conditions, the first line of treatment can be nonoperative management, but shared decision making with the patient and caregiver must occur when and if the deformity worsens regarding that operative intervention.
Pearls and Other Issues
Pes cavus typically presents in adolescence or early adulthood and is often a sign of an underlying neurological disease.
Through a combination of a history, physical exam, and imaging, the clinician should be able to diagnose if the deformity is forefoot or hindfoot driven. The clinician must also determine, primarily through specialized tests such as the Coleman block test, if the deformity is rigid or flexible.
Non-operative management may be considered, but in the majority of cases, where the underlying etiology is an HMSN, the cavus foot will continue to progress, and the deformity will become fixed and rigid without surgical correction.
Surgical interventions, including tendon transfers, osteotomies, and joint fusions, must be tailored to each specific patient’s clinical picture.
Enhancing Healthcare Team Outcomes
It is critical that the clinician correctly identifies the cavus foot as a sign of an underlying disease. In many cases, the patient may not be presenting to a foot and ankle specialist but rather may be seen by other members of the health-care team, such as their primary care provider or pediatrician.[20][8] Furthermore, identification of the correct diagnosis may involve subspecialist referral, electrodiagnostic testing, genetic testing, or even advanced imaging of the spine. [Level V]
Early identification and intervention to prevent progression of the and flexible and correctable cavus foot to the rigid cavus foot requiring arthrodesis and/or more extensive osteotomies is paramount.[1][7][32] [Level 4 and 5]
Identification of the subtle cavus foot may require greater vigilance as there may be no other signs or symptoms of systemic disease and yet the subtle cavus foot may lead to significant pathology and disability if left untreated.[2][14] [Level 5] Equally, it is important that subtle or borderline "deformity" is not overdiagnosed or overtreated, based only on rigid biomechanical guidelines - all treatment should be guided primarily by patient symptoms.