 Doppler Liver Assessment, Protocols, and Interpretation of Results
Doppler Liver Assessment, Protocols, and Interpretation of Results
Introduction
Doppler liver ultrasonography constitutes an effective and non-invasive means of evaluating the hepatic vasculature. Understanding the normal and abnormal waveforms for the primary hepatic vessels and their characteristic waveforms can help diagnose specific diseases that have a characteristic effect on these waveform patterns. Understanding how an abnormal hepatic artery, hepatic vein, or portal vein manifests on Doppler sonography can help identify or confirm liver diseases.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The liver plays a vital role in the body's metabolic functions and is composed of a relatively complex vascular architecture.[1] One-quarter of the cardiac output goes to the liver.[2] The liver is divided into various hepatic segments, and each hepatic lobule receives a branch from the portal vein, hepatic artery, and biliary tract called the portal triad.[3]
- The portal vein constitutes 75% of the hepatic blood supply. The blood from the portal vein is deoxygenated, carrying mainly nutrients. It is formed by the confluence of superior mesenteric and splenic veins. The portal vein drains all the upper and middle parts of the gastrointestinal tract, pancreas, gallbladder, and spleen.[4] Within the liver, the portal is divided into two branches: the left and the right portal veins. The left supplies segments II, III, and IV, while the right portal vein supplies segments V, VIII, VI, and VII. Variants of the portal venous system are not uncommon.[5]
- Hepatic veins: The hepatic veins are three branches (right, left, and middle hepatic veins) draining blood to the IVC.[6] The most common morphology of the hepatic veins includes a right hepatic vein and a common trunk for the middle and left hepatic veins.[7]
- The hepatic artery supplies 25% of the hepatic blood flow and constitutes the main bulk of oxygenated blood to the liver.[2] Frequent variations of the origin of the hepatic artery exist, with the most common type constituting the common hepatic artery arising from the celiac artery in 70% of patients.[8]
- The inferior vena cava (IVC) represents the confluence of the right and left common iliac veins and is the retroperitoneal draining vessel to the hepatic veins. The inferior vena cava subsequently empties deoxygenated blood to the right heart.[9]
Hepatopetal and Hepatofugal Flow
Hepatopetal flow refers to blood flow towards the liver (from the portal hepatis to the liver periphery). It typically is used in describing the normal blood flow direction in the portal vein. [10] This occurs in a normal liver and allows the liver to detoxify the blood that enters it after absorbing nutrients from the intestine through the portal vein.
Hepatofugal flow refers to blood flow away from the liver in the portal vein and is sometimes referred to as "retrograde" flow. In other words, the portal venous blood flow pattern is from the periphery of the liver towards the porta hepatis.[10] This occurs when the portal venous pressure is high in the case of portal hypertension. Thus portosystemic shunts are reopened with additional findings that include a more narrowed portal vein and prominence of the hepatic artery.[11] Occasionally, a to-and-fro bidirectional blood flow pattern alternating between hepatopetal and hepatofugal flow can be seen in the portal vein before the onset of frank hepatofugal flow.[12]
While HVPG (hepatic venous pressure gradient) is the gold standard for measuring the portal and hepatic venous pressure, it is an invasive procedure with the insertion of a catheter into the hepatic vessels.[13] On the other hand, Doppler ultrasound is a non-invasive procedure and can evaluate for abnormal physiology of the hepatic vasculature.
Indications
Assessment of the Following Clinical Presentations of Diseases
Follow-Up After Liver Transplantation Operation
Hepatic Doppler is used in the early detection of vascular occlusion or graft rejection, and it is the most preferred method of follow-up due to its low cost and non-invasiveness.[14] Sonographic assessment of a post-transplant liver includes a gray-scale evaluation of the hepatic parenchyma and the hepatic biliary tree. Doppler evaluation of the hepatic vasculature involves both gray-scale and Doppler assessment. Evaluation for strictures can manifest as varying degrees of vessel narrowing.[15]
Thrombus formation in the portal vein and IVC can be evaluated on both gray-scale and Doppler assessments. A normal hepatic artery will demonstrate a rapid systolic upstroke lasting up to 80 milliseconds. The resistive index of the hepatic artery, calculated as the ratio of peak systemic velocity minus peak diastolic velocity divided by peak systolic velocity, should be between 0.5 to 0.7.[15] In the setting of post-transplant evaluation, the portal vein should demonstrate a continuous hepatopetal flow pattern with only mild velocity variations on inspiration and expiration. Hepatic veins and IVC should demonstrate a phasic flow pattern corresponding to the blood flow of the cardiac cycle.[15]
Diagnosis of Portal Hypertension and Patency of Collaterals
Cirrhosis and an alteration in portal hemodynamics ultimately result in an increased pressure gradient in the portal vein resulting in abnormal portal vein blood flow away from the liver.[16] Doppler ultrasonography can assess blood flow direction and evaluate the presence of collateral vessels. Doppler indices include portal and splenic venous velocities, flow directions, and resistive/pulsatility indices of the arterial vasculature.[17]
Additional strengths of Doppler assessment include real-time observation, while limitations include a poor detection of slow blood flow and a reduced frame rate.[18] Other useful parameters in the diagnosis of cirrhosis include liver and spleen size, evaluation of liver echotechture, and the evaluation of the bluntness of the liver edge.[19] The normal portal vein pressure is less than 6 mmHg. Portal hypertension is clinically manifested when this pressure exceeds 12 mmHg.
Diagnosis of Budd Chiari Syndrome
Budd-Chiari syndrome represents an outflow obstruction of the hepatic veins is most typically secondary to a prothrombotic disorder.[20] Doppler in Budd-Chiari syndrome is diagnosed by the occlusion of the hepatic vein drainage of the liver either by stenosis or thrombosis of the hepatic veins or the higher draining inferior vena cava. This is done by measuring the direction and velocity of flow and the vessel diameter.[21] Often there is a non-visualization of the hepatic vein vasculature on Doppler color ultrasound. A fibrous cord, luminal thrombus, and stenosis can be seen.[22] Collaterals can also be seen in a spiderweb morphology, often extending to the inferior vena cava or other hepatic veins.
Diagnosis and Follow-Up of Thrombosis
Chronic thrombus formation can occur in the portal veins, hepatic veins, or the inferior vena cava. Thrombosis appears as an absent signal on color Doppler evaluation. The gold standard for diagnosing vessel thrombosis is angiography of the suspected vessel, but it is an invasive procedure.[23] In chronic thrombosis, collaterals start to appear along with recanalization of the obstructed vessel. Portal vein thrombosis could be due to benign obstruction of the portal vein (caused by the over-coagulable state, slow blood flow, or vascular injury) or malignant obstruction (caused by infiltration of the endovascular lining of the vessel).[24]
Evaluation of a TIPS (transjugular intrahepatic portosystemic shunt) Stent
The transjugular intrahepatic portosystemic shunt (TIPS) procedure is one treatment option for patients with cirrhosis or noncirrhotic total hypertension. TIPS shunts function to treat those who suffer from refractory ascites and variceal bleeding.[25] TIPS dysfunction has a high incidence and can be secondary to malpositioning, thrombosis, and pseudointimal hyperplasia.[26] Ultrasound can assess TIPS velocities(normally considered 90 to 190 cm/s), normal portal vein blood velocity before entering the shunt (normal reading is around 30 cm/s), and assess waveforms and the presence of stenosis.[27]
Assessment of Hemodynamics of Hepatic Focal Lesions
Doppler evaluation can be used in the assessment of benign hemangiomas and telangiectasia.[28] Hypoechoic hepatic focal lesions may appear through the screening process of the high-risk populations for hepatocellular carcinoma. The lesions may be associated with enlarged porta hepatic lymph nodes or para-aortic lymph nodes in metastasis. The vascular flow on color Doppler around the focal lesion can evaluate for neovascularization.[29][30]
Hemodynamics in Heart Failure
This will result in hepatic venous congestion and retrograde flow, inferior vena cava congestion with dilated diameters of the vessels, and increased portal vein pulsatility.[31]
Contraindications
There are no contraindications to this non-invasive procedure.
Equipment
Doppler ultrasound for the abdominal examination has two types: pulsed and color Doppler. Continuous Doppler is used in high-frequency flow in the cardiac valves and vessel examination but is not suitable for the portal and hepatic veins and IVC.
Personnel
Usually, Doppler ultrasound is carried out by an experienced sonographer, either a radiologist or gastroenterologist.
Preparation
Fasting is preferred (4 to 6 hours before examination) to decrease gaseous distension and fluids in the abdomen and increase the visibility of the vessels.[32] Before starting the examination, device adjustments of the gain, frequency, and depth are crucial.[33][34]
Technique or Treatment
Using hepatic Doppler ultrasound as part of the abdominal ultrasound will increase the operator's experience in refining the probe movement and better visualizing the hepatic vessels. The time consumed for both examinations (abdominal ultrasound and hepatic doppler) will not increase much.
- The patient could be asked to hold his breath to improve visualization.[35]
- The red color on the screen is usually set up in most devices as the direction of flow towards the probe, while the blue indicates the direction of blood flow away from the probe.
- The portal vein has a thickened fibrous tissue wall that will be reflected as drawing an echogenic line around the vessel, while hepatic vein walls are thin and non-visualized.
- Portal vein diameter can range from 7 to 15 mm.[36] Hepatic veins can have a diameter of 5 to 7 mm. The IVC normal diameter ranges from 13 to 22 mm with a collapsible wall on pressure.[37]
- The patient is best positioned in the left lateral or supine position. Scanning starts in the right subcostal area, which allows for visualization of the portal vein. The confluence of the splenic and superior mesenteric veins is visualized when moving left towards the midline.
- Then scanning in the substernal position, the operator will view the IVC (which should be compressible) and aorta at the midline while the probe faces posteriorly (either longitudinally or transversely).
- Hepatic veins can be best viewed from the right intercostal position where the probe is facing medially, and this position is best to view the drainage of the three hepatic veins into the IVC. The hepatic veins could also be viewed from the subcostal position directing the probe posteriorly. Left and middle hepatic veins are best visualized from the substernal position.
Limitations
- Obesity can cause limitations in the visualization of vessel flow and velocity.
- Eating may cause an increase in the portal pressure and widen the diameter of the vessel. Ingested contents and resultant gaseous distension may hinder the visualization of vessels. Therefore, fasting for at least 4 to 6 hours before the Doppler examination is recommended.
- Changes in the liver hemodynamics may be falsely diagnosed if the gain and frequency are not well adjusted in the device.
- The low frequency may falsely diagnose portal vein thrombosis.
- Patients who cannot hold their breath will create some difficulty for the operator to visualize the vessels, but this could be overcome by the timing of inhalation and moving the probe synchronously.
Clinical Significance
Hepatic Doppler ultrasound is a non-invasive investigative tool that can help clinicians, especially if added to an abdominal ultrasound exam. The procedure is cost-effective and has no complications.
Doppler ultrasound is the first imaging technique used in assessing the vascular condition in the following diseases:
- Portal hypertension associated with cirrhosis
- Portal or hepatic vein thrombosis[38]
- Vascularity of the hepatic focal lesions[39]
- Follow-up after TIPS or liver transplantation[40]
- Measuring the hepatic vein and artery patency, blood velocity, and direction
Referral to other invasive investigative or treatment procedures such as hepatic venous pressure gradient HVPG, angiography, transjugular intrahepatic portosystemic shunt TIPS, and other procedures depends on initial assessment on Doppler ultrasound.
Enhancing Healthcare Team Outcomes
Evaluation of the liver starts with clinical assessment and laboratory workup. Radiological evaluation in the form of abdominal ultrasound accompanied by hepatic Doppler could give the physician a complete picture of the patient's liver condition with a non-invasive procedure. Doppler can detect early hepatic focal lesions and be part of the liver ultrasound screening process in high-risk individuals or post-operative hepatic procedures such as TIPS and liver transplantation.[27]
Hepatic Doppler also can detect portal hypertension and guide further management to include prophylactic band ligation or early medical therapy before the condition deteriorates.[41] It can also be used in the follow-up of patients post-ligation.
Although sonographers and radiologists mainly conduct hepatic Doppler exams, it offers a real-time evaluation of the liver. Doppler can also be an essential part of the hepatic assessment by gastroenterologists and surgeons. As part of their training and practice, such subspecialists are familiar with abdominal ultrasound and hepatic Doppler.
Media
(Click Image to Enlarge)

Portal Hypertension. B-Mode ultrasound showing main portal vein diameter of 15.1 millimeters. This is an indirect finding of portal hypertension.
Contributed by B Covello, MD
(Click Image to Enlarge)
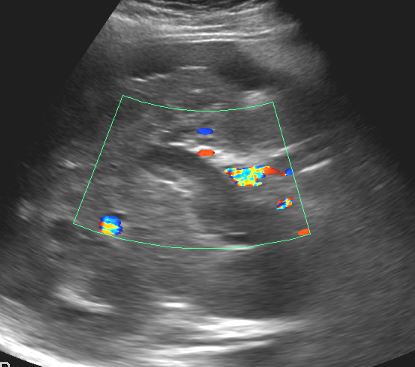
Thrombosis of the portal vein Contributed by Dawood Tafti, MD.
(Click Image to Enlarge)
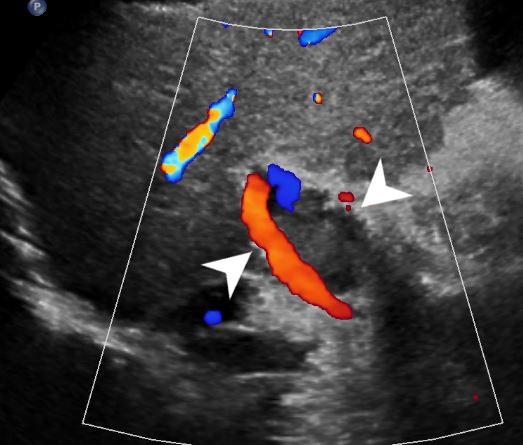
Portal vein thrombosis Contributed by Dawood Tafti, MD.
References
Torres Rojas AM, Lorente S, Hautefeuille M, Sanchez-Cedillo A. Hierarchical Modeling of the Liver Vascular System. Frontiers in physiology. 2021:12():733165. doi: 10.3389/fphys.2021.733165. Epub 2021 Nov 16 [PubMed PMID: 34867439]
Eipel C, Abshagen K, Vollmar B. Regulation of hepatic blood flow: the hepatic arterial buffer response revisited. World journal of gastroenterology. 2010 Dec 28:16(48):6046-57 [PubMed PMID: 21182219]
Couinaud C. Liver anatomy: portal (and suprahepatic) or biliary segmentation. Digestive surgery. 1999:16(6):459-67 [PubMed PMID: 10805544]
Level 3 (low-level) evidenceCarneiro C, Brito J, Bilreiro C, Barros M, Bahia C, Santiago I, Caseiro-Alves F. All about portal vein: a pictorial display to anatomy, variants and physiopathology. Insights into imaging. 2019 Mar 21:10(1):38. doi: 10.1186/s13244-019-0716-8. Epub 2019 Mar 21 [PubMed PMID: 30900187]
Level 3 (low-level) evidenceSchmidt S, Demartines N, Soler L, Schnyder P, Denys A. Portal vein normal anatomy and variants: implication for liver surgery and portal vein embolization. Seminars in interventional radiology. 2008 Jun:25(2):86-91. doi: 10.1055/s-2008-1076688. Epub [PubMed PMID: 21326549]
Hardy KJ. The hepatic veins. The Australian and New Zealand journal of surgery. 1972 Aug:42(1):11-4 [PubMed PMID: 4512537]
Fang CH, You JH, Lau WY, Lai EC, Fan YF, Zhong SZ, Li KX, Chen ZX, Su ZH, Bao SS. Anatomical variations of hepatic veins: three-dimensional computed tomography scans of 200 subjects. World journal of surgery. 2012 Jan:36(1):120-4. doi: 10.1007/s00268-011-1297-y. Epub [PubMed PMID: 21976007]
Marchal G, Kint E, Nijssens M, Baert AL. Variability of the hepatic arterial anatomy: a sonographic demonstration. Journal of clinical ultrasound : JCU. 1981 Sep:9(7):377-81 [PubMed PMID: 6792236]
Tucker WD, Shrestha R, Burns B. Anatomy, Abdomen and Pelvis: Inferior Vena Cava. StatPearls. 2024 Jan:(): [PubMed PMID: 29493975]
McNaughton DA, Abu-Yousef MM. Doppler US of the liver made simple. Radiographics : a review publication of the Radiological Society of North America, Inc. 2011 Jan-Feb:31(1):161-88. doi: 10.1148/rg.311105093. Epub [PubMed PMID: 21257940]
Ralls PW. Color Doppler sonography of the hepatic artery and portal venous system. AJR. American journal of roentgenology. 1990 Sep:155(3):517-25 [PubMed PMID: 2117348]
Level 2 (mid-level) evidenceWachsberg RH, Bahramipour P, Sofocleous CT, Barone A. Hepatofugal flow in the portal venous system: pathophysiology, imaging findings, and diagnostic pitfalls. Radiographics : a review publication of the Radiological Society of North America, Inc. 2002 Jan-Feb:22(1):123-40 [PubMed PMID: 11796903]
Suk KT. Hepatic venous pressure gradient: clinical use in chronic liver disease. Clinical and molecular hepatology. 2014 Mar:20(1):6-14. doi: 10.3350/cmh.2014.20.1.6. Epub 2014 Mar 26 [PubMed PMID: 24757653]
Kimura Y, Tapia Sosa R, Soto-Trujillo D, Kimura Sandoval Y, Casian C. Liver Transplant Complications Radiologist Can't Miss. Cureus. 2020 Jun 5:12(6):e8465. doi: 10.7759/cureus.8465. Epub 2020 Jun 5 [PubMed PMID: 32642371]
Crossin JD, Muradali D, Wilson SR. US of liver transplants: normal and abnormal. Radiographics : a review publication of the Radiological Society of North America, Inc. 2003 Sep-Oct:23(5):1093-114 [PubMed PMID: 12975502]
Kim MY, Jeong WK, Baik SK. Invasive and non-invasive diagnosis of cirrhosis and portal hypertension. World journal of gastroenterology. 2014 Apr 21:20(15):4300-15. doi: 10.3748/wjg.v20.i15.4300. Epub [PubMed PMID: 24764667]
Baik SK. Haemodynamic evaluation by Doppler ultrasonography in patients with portal hypertension: a review. Liver international : official journal of the International Association for the Study of the Liver. 2010 Nov:30(10):1403-13. doi: 10.1111/j.1478-3231.2010.02326.x. Epub 2010 Aug 19 [PubMed PMID: 20731772]
Maruyama H, Yokosuka O. Ultrasonography for Noninvasive Assessment of Portal Hypertension. Gut and liver. 2017 Jul 15:11(4):464-473. doi: 10.5009/gnl16078. Epub [PubMed PMID: 28267700]
Colli A, Fraquelli M, Andreoletti M, Marino B, Zuccoli E, Conte D. Severe liver fibrosis or cirrhosis: accuracy of US for detection--analysis of 300 cases. Radiology. 2003 Apr:227(1):89-94 [PubMed PMID: 12601199]
Level 3 (low-level) evidenceBargalló X, Gilabert R, Nicolau C, García-Pagán JC, Ayuso JR, Brú C. Sonography of Budd-Chiari syndrome. AJR. American journal of roentgenology. 2006 Jul:187(1):W33-41 [PubMed PMID: 16794137]
Valla DC. Budd-Chiari syndrome/hepatic venous outflow tract obstruction. Hepatology international. 2018 Feb:12(Suppl 1):168-180. doi: 10.1007/s12072-017-9810-5. Epub 2017 Jul 6 [PubMed PMID: 28685257]
Chaubal N, Dighe M, Hanchate V, Thakkar H, Deshmukh H, Rathod K. Sonography in Budd-Chiari syndrome. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2006 Mar:25(3):373-9 [PubMed PMID: 16495498]
Manzano-Robleda Mdel C, Barranco-Fragoso B, Uribe M, Méndez-Sánchez N. Portal vein thrombosis: what is new? Annals of hepatology. 2015 Jan-Feb:14(1):20-7 [PubMed PMID: 25536638]
Chawla YK, Bodh V. Portal vein thrombosis. Journal of clinical and experimental hepatology. 2015 Mar:5(1):22-40. doi: 10.1016/j.jceh.2014.12.008. Epub 2015 Jan 6 [PubMed PMID: 25941431]
Foshager MC, Ferral H, Nazarian GK, Castañeda-Zúñiga WR, Letourneau JG. Duplex sonography after transjugular intrahepatic portosystemic shunts (TIPS): normal hemodynamic findings and efficacy in predicting shunt patency and stenosis. AJR. American journal of roentgenology. 1995 Jul:165(1):1-7 [PubMed PMID: 7785564]
Cura M, Cura A, Suri R, El-Merhi F, Lopera J, Kroma G. Causes of TIPS dysfunction. AJR. American journal of roentgenology. 2008 Dec:191(6):1751-7. doi: 10.2214/AJR.07.3534. Epub [PubMed PMID: 19020247]
Benito A, Bilbao J, Hernández T, Martinez-Cuesta A, Larrache J, González I, Vivas I. Doppler ultrasound for TIPS: does it work? Abdominal imaging. 2004 Jan-Feb:29(1):45-52 [PubMed PMID: 15160753]
Naganuma H, Ishida H, Kuroda H, Suzuki Y, Ogawa M. Hereditary hemorrhagic telangiectasia: how to efficiently detect hepatic abnormalities using ultrasonography. Journal of medical ultrasonics (2001). 2020 Jul:47(3):421-433. doi: 10.1007/s10396-020-01022-w. Epub 2020 May 10 [PubMed PMID: 32390074]
Kang HJ, Lee JM, Jeon SK, Ryu H, Yoo J, Lee JK, Han JK. Microvascular Flow Imaging of Residual or Recurrent Hepatocellular Carcinoma after Transarterial Chemoembolization: Comparison with Color/Power Doppler Imaging. Korean journal of radiology. 2019 Jul:20(7):1114-1123. doi: 10.3348/kjr.2018.0932. Epub [PubMed PMID: 31270975]
Maruyama H, Yoshikawa M, Yokosuka O. Current role of ultrasound for the management of hepatocellular carcinoma. World journal of gastroenterology. 2008 Mar 21:14(11):1710-9 [PubMed PMID: 18350602]
Jefkins M, Chan B. Hepatic and portal vein Dopplers in the clinical management of patients with right-sided heart failure: two case reports. The ultrasound journal. 2019 Nov 12:11(1):30. doi: 10.1186/s13089-019-0146-3. Epub 2019 Nov 12 [PubMed PMID: 31748951]
Level 3 (low-level) evidenceAfif AM, Chang JP, Wang YY, Lau SD, Deng F, Goh SY, Pwint MK, Ooi CC, Venkatanarasimha N, Lo RH. A sonographic Doppler study of the hepatic vein, portal vein and hepatic artery in liver cirrhosis: Correlation of hepatic hemodynamics with clinical Child Pugh score in Singapore. Ultrasound (Leeds, England). 2017 Nov:25(4):213-221. doi: 10.1177/1742271X17721265. Epub 2017 Aug 3 [PubMed PMID: 29163657]
Carovac A, Smajlovic F, Junuzovic D. Application of ultrasound in medicine. Acta informatica medica : AIM : journal of the Society for Medical Informatics of Bosnia & Herzegovina : casopis Drustva za medicinsku informatiku BiH. 2011 Sep:19(3):168-71. doi: 10.5455/aim.2011.19.168-171. Epub [PubMed PMID: 23408755]
Kurzweil A, Martin J. Transabdominal Ultrasound. StatPearls. 2024 Jan:(): [PubMed PMID: 30521234]
Macnaught F, Campbell-Rogers N. The liver: how we do it. Australasian journal of ultrasound in medicine. 2009 Aug:12(3):44-47. doi: 10.1002/j.2205-0140.2009.tb00061.x. Epub 2015 Dec 31 [PubMed PMID: 28191063]
Geleto G, Getnet W, Tewelde T. Mean Normal Portal Vein Diameter Using Sonography among Clients Coming to Radiology Department of Jimma University Hospital, Southwest Ethiopia. Ethiopian journal of health sciences. 2016 May:26(3):237-42 [PubMed PMID: 27358544]
Patil S, Jadhav S, Shetty N, Kharge J, Puttegowda B, Ramalingam R, Cholenahally MN. Assessment of inferior vena cava diameter by echocardiography in normal Indian population: A prospective observational study. Indian heart journal. 2016 Dec:68 Suppl 3(Suppl 3):S26-S30. doi: 10.1016/j.ihj.2016.06.009. Epub 2016 Jul 1 [PubMed PMID: 28038721]
Level 2 (mid-level) evidenceFrancoz C, Valla D, Durand F. Portal vein thrombosis, cirrhosis, and liver transplantation. Journal of hepatology. 2012 Jul:57(1):203-12. doi: 10.1016/j.jhep.2011.12.034. Epub 2012 Mar 21 [PubMed PMID: 22446690]
Tanaka H. Current role of ultrasound in the diagnosis of hepatocellular carcinoma. Journal of medical ultrasonics (2001). 2020 Apr:47(2):239-255. doi: 10.1007/s10396-020-01012-y. Epub 2020 Mar 13 [PubMed PMID: 32170489]
Ricci P, Cantisani V, Lombardi V, Alfano G, D'Ambrosio U, Menichini G, Marotta E, Drudi FM. Is color-Doppler US a reliable method in the follow-up of transjugular intrahepatic portosystemic shunt (TIPS)? Journal of ultrasound. 2007 Mar:10(1):22-7. doi: 10.1016/j.jus.2007.02.005. Epub 2007 Apr 16 [PubMed PMID: 23396711]
Aggeletopoulou I, Konstantakis C, Manolakopoulos S, Triantos C. Role of band ligation for secondary prophylaxis of variceal bleeding. World journal of gastroenterology. 2018 Jul 14:24(26):2902-2914. doi: 10.3748/wjg.v24.i26.2902. Epub [PubMed PMID: 30018485]