 Sonography Gynecology Infertility Assessment, Protocols, and Interpretation
Sonography Gynecology Infertility Assessment, Protocols, and Interpretation
Introduction
Infertility is defined as the inability to conceive after one year of unprotected sexual intercourse in women under 35 and 6 months of unprotected intercourse in women older than 35. Infertility affects about 15.5% of women.[1] The etiologies of infertility include tubal factor (14%), defects in ovulation (21%), and male factor (26%), and are often unexplained by traditional testing (28%). The basic workup for infertility involves evaluating ovarian reserve, tubal and uterine assessment, thyroid problems, prolactin disorders, confirmation of polycystic ovarian syndrome (PCOS), semen parameters, and additional assessment to confirm that the patient is medically fit and ready for pregnancy. This document will discuss the role of sonography in the evaluation and management of female infertility.
Different types of ultrasound scanning for infertility include:
- Baseline or screening ultrasound to assess the pelvic anatomy of the uterus, including uterine lining and bilateral ovaries. All abnormal findings are measured and characterized, such as fibroids, uterine malformations, hydrosalpinges, and ovarian cysts.
- Follicular monitoring ultrasounds are used to track follicles that are maturing and measure the endometrial thickness and also note the endometrial consistency.
- Saline Infusion Sonograms (SIS) with or without 3D assessment are used to assess the uterine cavity for any abnormalities and can also be used for tubal patency assessment.
- Abdominal ultrasound may be needed with any of the above scanning modalities to better assess the pelvic structures that cannot be fully seen with transvaginal scanning or can be used for virginal/ young girls undergoing fertility preservation or female to male transgender patients undergoing fertility treatments to limit feelings of gender dysphoria. In addition, abdominal scanning is used to guide Intrauterine Inseminations, embryo transfers, endometrial biopsies, and hysteroscopic uterine procedures to allow the surgeon a better appreciation of the uterine anatomy.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Understanding the different phases of the endometrium during the menstrual cycle and normal developmental phases in the ovarian follicles is essential for both initial baseline screening assessment and monitoring during natural, IUI, or IVF cycles.
Endometrium
The endometrium goes through consistent changes each month in response to the hormonal milieu. After sloughing of the endometrium and in response to rising estrogen, the endometrium thickens significantly during the follicular phase and shows a trilaminar pattern on ultrasound. After ovulation, in the luteal phase, the lining becomes decidualized, brighter, and is unilaminar until menstruation. The menstrual endometrium can have a heterogeneous appearance with hyper- and hypo- echoic features. Endometrial thickness (ET), endometrial morphological changes, and vascularity are assessed while performing ultrasound during natural or stimulated cycles.
- Endometrial thickness - The thickness of the endometrium is thin initially 4.4 +/- 0.2 mm after menses and increases to 10.3 +/- 0.3 mm before ovulation.[2] Raine-Fenning and Bakos also noted that in natural cycles, the mean endometrial thickness ranges from 10 to 12.5 mm before ovulation.[3][4]
- Endometrial morphology can be categorized into three patterns; Trilaminar, homogenous, and heterogeneous (Figure 1). A trilaminar endometrium is triple-layered and characterized by a hypoechoic endometrium with a central line. This pattern is noted during the follicular phase from 5 to 6 days before ovulation and continues to the day of ovulation.[4] The presence of a trilaminar endometrium on the day of the trigger injection has been associated with higher pregnancy rates in IVF cohorts.[5] Once ovulation has occurred, the organized appearance of the trilaminar lining disappears, and the endometrium becomes more homogenous with poorly defined outer walls and the absence of the central echogenic line. During assisted reproductive technology (ART) cycles, this is often a sonographic clue before laboratory confirmation that the patient may have ovulated (Figure 2). A heterogenous endometrium may be seen while a patient is menstruating due to the presence of blood or clot or when intracavitary pathology (i.e., polyp, myoma, or hyperplastic tissue) is present.[6]
- Endometrial Vascularity is classified into three grades based on the visual assessment of endometrium on power color flow doppler imaging before ovulation. Grade 1 shows no sub-endometrial blood flow, grade 2 shows sub-endometrial blood flow, and grade 3 shows both endometrial and sub-endometrial blood flow.[7]
Ovary
Based on the stages of development, the ovaries have primordial, primary, secondary, tertiary, or antral follicles. The number of primordial follicles determines true ovarian reserve. Primordial follicles are small and difficult to be seen by ultrasound. The ovary has 6-7 million primordial follicles at around five months of gestational age, slowly declining to approximately 1000 at menopause.[8][9]
With the initiation of menarche, a cohort of dormant primordial follicles are recruited during each day of the menstrual cycle, and these follicles grow in size steadily. These primordial follicles develop into primary, secondary, and antral follicles. Development of the fluid-filled cavity, also called the antrum adjacent to the maturing oocyte, results in forming of the antral or tertiary follicle. In normal cycles, one follicle matures and is destined to ovulate while other follicles degenerate and ultimately disappear through a process called apoptosis or programmed cell death.
Antral follicular count (AFC), one of the standard measurements for ovarian reserve, is calculated as the sum of all follicles ranging from 2 to 10 mm contained within both ovaries. The preferred time to measure the AFC is during cycle days 2 through 4 due to the absence of corpus luteum and ovarian cysts. Even though there is a slight variation in the AFC during the menstrual cycle, the AFC can be performed at any point during the menstrual cycle as long as cysts are not obscuring the view of the ovary in its entirety.[10]
Follicle-stimulating hormone (FSH) receptors are developed in the antral follicle once it reaches a minimum diameter of 6 mm, and further growth of this follicle is under control of FSH produced by the anterior pituitary. Dominant follicles are follicles >10 mm. By day 8 to 12, dominant follicles are usually formed, and they grow at an average of 1 to 1.4 mm in diameter per day until they reach a mean diameter of 20 to 24 mm at the time of ovulation in a natural-unstimulated cycle.[11] Other authors have noted a wider range of mean follicular diameter before ovulation.[12]
For ovulation trigger, most IVF centers usually use a cut-off of 18 to 20 mm before egg retrievals. This differs from patients undergoing clomiphene citrate cycles in which the recent literature suggests follicles closer to 21 to 22 mm have a higher odds of leading to clinical pregnancy.[13] (Figure 3) After ovulation, the follicle collapses to form the corpus luteum, producing progesterone and estradiol to support implantation and nidation. The corpus luteum has a “ring of fire” on color flow doppler due to a large increase in angiogenesis.
Indications
Transvaginal Sonogram
- Baseline assessment of the uterus, ovaries, and adnexa to rule out any pathology like fibroids, polyps, uterine anomalies, hydrosalpinx, or PCOS
- Ovarian reserve assessment- antral follicular count
- Monitoring ovulation induction during clomiphene citrate, letrozole, or gonadotropin cycles with or without intrauterine insemination (IUI) and with in-vitro fertilization (IVF) cycles.
- For timing the ovulation trigger during IUI and IVF
- Assessment of endometrial thickness during IUI and IVF
- For performing oocyte retrievals and sometimes for embryo transfer or other uterine procedures, transabdominal scanning is ineffective.
Transabdominal Sonogram
- Women with a large uterus caused by fibroids or adenomyosis, or both.
- When the uterus or ovaries closely adhered to the anterior abdominal wall secondary to scarring from prior surgery, infection or endometriosis.
Saline Infusion Sonogram
- To assess the uterine cavity for pathologies such as polyps, submucosal fibroids, intrauterine synechiae or scarring, and uterine malformations.
- To assess tubal patency (instead of a traditional hysterosalpingogram (HSG)).
Contraindications
Contraindications for an SIS include pregnancy, heavy menstruation or active bleeding, suspicion of infection as noted by patient symptomatology, or a suspicious vaginal discharge upon examination.
Equipment
An ultrasound machine with transabdominal and transvaginal transducers is required. Transducers of 3.5 Mhz or more are used for transabdominal scans, whereas transducers of 5MHz or more are used for transvaginal scans. In recent years, 3D ultrasound has shown value in performing SIS and assessing AFC and ovarian volumes.
Personnel
The required personnel includes a sonographer, a radiologist, an OBGYN trained in ultrasounds, and reproductive endocrinology and infertility specialists.
Preparation
For a transabdominal scan, a distended bladder is recommended to displace the bowel and provide an acoustic window to visualize the pelvic structures. For a transvaginal scan, SIS, or sonohysterosalpingogram, an empty bladder is recommended.
It is ideal for performing SIS or sonohysterosalpingogram during the mid follicular phase when the patient is no longer bleeding to reduce the false-positive rate for detecting polyps or adhesions and better visualization of any pathological conditions. A urine pregnancy test is performed to confirm that the patient is not pregnant before performing SIS or sonohysterosalpingogram.
Technique or Treatment
Transvaginal Ultrasound
The patient is kept in a dorsal lithotomy position, and the transvaginal probe is introduced into the vagina either by the patient or the sonographer. The transducer is covered with ultrasound gel, and a condom or condom-like cover is placed over the gelled probe. KY jelly or a similar gel is then placed on the covered transducer for patient comfort.
- Baseline assessment includes evaluation of uterus, endometrium, ovaries, and cul de sac.
- Uterus: The uterus is evaluated in both sagittal and transverse planes (Figure 4). Attention is given to evaluate the size, shape, orientation of the uterus, cervix, myometrium, and endometrium. The length and height of the uterus are measured in the sagittal plane, and width is measured in transverse or coronal planes at the level of the tubal ostia or cornual regions. The myometrium is evaluated for any pathology like fibroids or adenomyosis. The location and character of all pathological lesions are noted and documented in the images and the final report.
- Endometrium - The endometrium is measured perpendicularly from one echogenic to the other echogenic border at its thickest part in the midsagittal plane (Figure 5). If the fluid is visualized in the cavity, the endometrium is measured by combining the anterior and posterior endometrial thicknesses separately without including the fluid.
- Adnexa: The adnexa is evaluated for any masses such as hydrosalpinges, para-ovarian cysts, or para-tubal cysts.
- Ovaries: The ovaries are identified bilaterally and measured in three dimensions (length, height, and width) (Figure 6). The antral follicles are seen as round or oval anechoic structures. A baseline AFC is performed by counting the number of follicles between 2 to 10 mm and measuring the dimensions of follicles greater than or equal to 10 mm in the early follicular phase in both ovaries.[14] AFC can be measured using three different techniques during the transvaginal scan; a traditional real-time two-dimensional (2D) scan, stored 2D cine loops, or three-dimensional (3D) data sets. Real-time 2D scanning is used to measure the ovary in both the longitudinal and coronal planes. The next step is to optimize the ultrasound settings for better image quality while centering the ovary in its largest axis. The ovary should occupy at least 50% of the screen while counting the follicles ranging from 2 to 10 mm from one ovarian margin to the other. The total follicle number for both ovaries is added to obtain AFC.[10] The 2D cine loop uses the same technique as real-time 2D ultrasound except that the loop involves the continuous sweep of the ovary. The data is saved and assessed at a later time. Even though 3D ultrasound has better reproducibility than 2D methods, it needs additional special training and ultrasound equipment. The technique to perform 3D ultrasound is beyond the scope of this basic topic hence will not be discussed in detail.
- Cul de sac: The cul de sac is evaluated for any fluid, and a sliding sign is performed to assess for any adhesions. The examiner's hand is placed on the patient's abdomen to apply pressure on the uterus. The transvaginal probe is placed near the posterior vaginal fornix to assess whether the cervix and the uterus glide over the anterior rectum and sigmoid colon. The lack of sliding of these organs implies adhesive disease of these structures.[15]
- Monitoring during ovulation induction cycles: A transvaginal ultrasound is performed to assess the follicular growth, endometrium, and uterine arterial blood flow during ovulation induction cycles.
- Follicular assessment: The measurement of the follicles is usually performed using a transvaginal ultrasound. The follicle size can be done using two different techniques during the transvaginal scan using a traditional real-time 2D scan or sonography-based automated volume calculation (Sono AVC). In traditional real-time 2D scanning, the follicles are measured by calculating the average of two orthogonal diameters. To accommodate the asymmetrical growth in the follicles greater than 15 mm, one can calculate the average of diameters in three orthogonal planes for greater accuracy if clinically warranted.[16]
- Endometrial assessment includes measurement of endometrial thickness, identifying the endometrial morphological pattern, and grading the endometrial vascularity. To assess endometrial vascularity, the color flow power doppler box is reduced to as small as possible and focused for a few seconds on the endometrial layer, occupying 50% of the screen.
Transabdominal Ultrasound
A transabdominal ultrasound is performed as needed with infertility. The transducer is placed on the patient's abdomen to assess the uterine size, shape, and orientation. In addition, the myometrium, endometrium, and ovaries are also assessed. This route of scanning is performed to assess ovarian reserve only in virgin patients, patients with vaginal or pelvic pain, or if the pelvic organs are located cranially and anteriorly due to their enlargement or adhesive disease.
Saline Infusion Sonogram
The patient is kept in a dorsal lithotomy position. Transvaginal ultrasound is performed as described above to assess the uterine size, orientation, adnexa, and ovaries. Any cul de sac or peritoneal fluid is noted and quantified. This detail is important in later considering tubal patency assessment after saline infusion. The transvaginal probe is removed from the vagina. A bivalve speculum is placed in the vagina. Cervix is cleansed with betadine or an alternative anti-septic solution. SIS catheter is introduced in the cervix. There are multiple types of SIS catheters (Figure 7).
When tubal patency needs to be assessed, it is preferable to use a catheter with a balloon that can be wedged in the lower uterine segment to block the backflow of fluid so that the fluid with bubbles can be better directed into the tubal ostia. After the catheter placement, the speculum is removed, and the transvaginal probe is reintroduced into the vagina. Normal saline is introduced through the catheter into the uterine cavity by the assistant while the sonographer or the physician is performing the ultrasound. Instillation of the normal saline into the uterine cavity distends the uterine cavity with the anechoic fluid. Any lesions in the endometrial cavity are visualized and measured in three dimensions and characterized accordingly (Figure 8).[17]
If tubal patency assessment is planned or required following the intrauterine assessment, a sonohysterosalpingogram (hysterosalpingo contrast sonography -HyCoSy) is performed. During HyCoSy, an agitated mixture of air and normal saline is injected into the uterine cavity through the SIS catheter while performing a real-time ultrasound. Attention is paid to the cornual ends bilaterally to visualize the passage of fluid with air bubbles through the ostia of the fallopian tubes and noting the spilling of the mixed fluid into the adnexa region or elsewhere in the abdominal cavity (Figure 9).
The final step is to evaluate the area where the balloon is located. The balloon is deflated, and the catheter is removed under ultrasound guidance. This part of the procedure is imperative to fully evaluate the previously occupied area by the balloon. Labeling of all pathological structures should also be noted on the ultrasound pictures while scanning.
Complications
The complications for SIS and sonohysterosalpingogram include pain, bleeding, and infection. Patients should be advised to take pain medication generally one hour before the procedure. Most advocate the use of ibuprofen 400 to 600 mg orally one hour before the procedure. Patients should be advised to look for signs of infections, including fever, abnormal vaginal discharge, pelvic pain, or tenderness up to one month after the procedure. A mild amount of bleeding is common after the procedure, which usually resolves within 24 hours. Additional bleeding may warrant evaluation.
Clinical Significance
Importance of Ovarian Assessment by Ultrasound
- Role of AFC: Evaluation of AFC has similar accuracy as Anti-Mullerian Hormone levels in predicting the ovarian reserve and the response to ovarian stimulation to gonadotropins and pregnancy success rates with IVF.[18] AFC less than 5 is considered low.[1] AFC more than or equal to 20 is associated with a high ovarian response and a higher risk for ovarian hyperstimulation syndrome.[10] Hence AFC can be used to adjust gonadotropin dosage. AFC less than or equal to 4 have an increased risk of menopause within 7 years.[19][20]
- Follicle assessment
- Gonadotropin stimulated cycles - The use of gonadotropins leads to the recruitment of multiple follicles compared with the typical single follicle in a natural, unstimulated cycle. Ultrasonographic assessment of follicular growth is an important step for clinical decision-making and early detection of complications such as ovarian hyperstimulation.[5] Under the influence of exogenous gonadotropins, the follicles grow at an average of 1.7 to 2 mm per day instead of 1 to 1.4 mm per day. Follicular size is directly related to oocyte recovery rates. The highest oocyte recovery rate ( 83.5%) is noted when the follicle diameter is between 18 to 20 mm and significantly lower when it is less than 12 mm or higher than 24 mm.[21] Therefore ultrasounds are performed to assess ovarian response to stimulation and determine the timing of oocyte maturity and timing for hCG or GnRH agonist triggers. Gonadotropin stimulation can also increase the risk of forming multiple follicles instead of a single follicle and result in ovarian hyperstimulation and /or multiple births. Ultrasound is an easy, reliable imaging technique to identify the formation of maturing follicles in which cycles can be modified or canceled as needed.
- Oral ovulation-inducing medications- Follicular assessment using ultrasound in this population is controversial as there is less chance of ovarian hyperstimulation and multiple births. Additionally, the increase of cycle monitoring with ultrasound may be cost-prohibitive for many patients without providing a significant difference in pregnancy rates. Although ultrasound is not routinely used in all patients, it is utilized in patients using an Hcg trigger for ovulation to time intercourse or IUI and also when there is difficulty predicting ovulation with ovulation predictor kits. In addition, a recent retrospective study including approximately 50,000 IUI cycles showed a higher risk of multifetal pregnancy in patients less than 40 years of age and with >2 mature ovarian follicles. Hence, it may be beneficial to monitor follicular growth in patients using oral ovulation induction medications to reduce multifetal gestations.[22]
- Diagnosis of Polycystic ovarian syndrome: PCOS contributes to female infertility secondary to anovulation. The ultrasound criteria to diagnose PCOS include assessing follicle number per ovary (FNPO) and ovarian volume. (Figure 10). An ovarian volume of greater than 10 ml and an AFC of greater than 12 per ovary on ultrasound is consistent with PCOS based on the Rotterdam Consensus conference. However, greater than 60% of women aged 25 to 30 were found to have ovaries with PCOS based on this criteria. Therefore, this criteria is being changed to FNPO greater than 20 and/ or ovarian volume greater than 10 ml without corpus luteum or other dominant follicles or cysts.[23]
- Diagnosis of other ovarian cysts like cystic teratomas (Figure 11), borderline or malignant ovarian tumors, and endometriomas (Figure 12). Cystic teratomas have hyperechoic areas, sometimes with calcifications. Endometriomas are notable for homogeneous low-level internal echoes or ground glass appearance.
Importance of Endometrial Assessment by Ultrasound
Ultrasound plays a key role in identifying different endometrial and uterine factors that affect embryo implantation.
- Exponential endometrial growth is observed in women undergoing gonadotropin stimulated cycles, whereas reduction in the endometrial lining was noted with increasing age and use of clomiphene citrate (CC).[24][25] Clomiphene citrate, a selective estrogen receptor modulator, affects endometrial development. On ultrasound, a thin endometrial stripe is sometimes developed due to CC's anti-estrogenic effect. (Figure 13). This negative effect on endometrial thickness correlates with the increasing dosage of CC. This effect of clomiphene citrate is noted to last until ovulation. A preovulatory endometrial lining of 6.5 to 7 mm or higher is associated with a better pregnancy rate than an endometrial lining of 6 mm or less.[26][27][28] Oral and/or vaginal Ethinyl estradiol or transdermal estradiol can be given during the CC cycle to increase the endometrial thickness. However, many studies have not shown that supplementation with estrogen for thin linings increases pregnancy rates. In patients with a thin endometrium, while taking CC, alternative ovulation-inducing agents in subsequent cycles may improve endometrial thickness, such as Tamoxifen. Tamoxifen is a selective estrogen receptor modulator, which has a stimulatory effect on estrogen receptors at the level of the uterus compared to the inhibitory effect of CC, thus promoting endometrial growth and increased endometrial thickness. Aromatase inhibitors like letrozole can also be tried in patients who have side effects with CC.
- Higher clinical pregnancy rates are noted when grade 3 endometrial vascularity was observed on color flow power doppler.[29][30]
- Despite other confounding factors affecting successful implantation, a few studies noted a positive correlation between higher clinical pregnancy rates and both triple-layer endometrium and endometrial thickness of 7 mm or higher.[31][24] Endometrial echogenic patterns alone do not alter clinical decision-making during infertility treatments but are important to consider when considering alternative treatments.
- The presence of polyps, endometrial fluid, adenomyosis, and leiomyomas is associated with abnormal endometrial molecular expressions, in turn altering endometrial receptivity and negatively impacting implantation and early embryo development.[32] On many occasions, a careful look at the endometrial lining can reveal endometrial polyps, submucosal fibroids, intrauterine fluid accumulation, or a congenital uterine anomaly. Even though endometrium can be assessed by transvaginal scan, SIS showed 93% specificity and 75 % sensitivity in detecting intrauterine adhesions compared to HSG, TVUS, SIS with hysteroscopy.[33] MRI, SIS, hysteroscopy were equally effective and superior to TVUS in detecting intracavitary lesions.[34]
- Endometrial polyps are either sessile or pedunculated localized tumors with endometrial glands, stroma, and blood vessels. Polyps are seen on ultrasound as hyperechoic masses with a feeding vessel on color flow Doppler (Figure 14). Endometrial polyps have a prevalence of 32% and are common in patients with infertility.[35] AAGL recommends surgical removal of polyps in infertile patients to improve their pregnancy success rates.[36]
- The most common causes for endometrial fluid in reproductive age women include intrauterine adhesions (Asherman’s syndrome), hydrosalpinx, cesarean scar niche, and subclinical intrauterine infection. Ultrasound features of intrauterine adhesions include disruption to the endometrial- myometrial junction, hypoechoic bands traversing the endometrial cavity, presence of skip lesions, and areas of normal functional endometrium (Figure 15).[37]
Importance of Uterine Assessment by Ultrasound
- Submucosal fibroids: On ultrasound, submucosal fibroids appear as hypoechoic structures in the endometrium with a circular pattern on color flow doppler. Submucosal fibroids can reduce implantation, live birth rates, and their surgical resection has improved clinical pregnancy rates, live birth rates in some studies.[38][39][40] (Figure 16). Intramural fibroids distorting the cavity can also decrease live birth rates by 21% and clinical pregnancy rates by 15% per IVF cycle.[41] In contrast, subserosal fibroids do not affect implantation but can obstruct the visualization of ovaries and oocyte collection. After a systematic review, ASRM proposed that myomectomy for cavity distorting myomas improves pregnancy rates and reduces the risk of early pregnancy loss.[42]
- Adenomyosis -ultrasound features of adenomyosis include globular uterine enlargement without any leiomyomas, cystic anechoic spaces in the myometrium, asymmetric uterine wall thickening, subendometrial echogenic linear striations, heterogeneous echotexture of myometrium, obscure endometrial/ myometrial border, thickening of the transition zone.[43] (Figure 17). Ultrasound has a sensitivity of 82.5% and specificity of 84.6% in diagnosing adenomyosis and is comparable to MRI.[44][45] Despite the conflicting evidence, adenomyosis has an overall negative impact on fertility due to its effect on endometrial receptivity and decidualization.[32]
- Congenital anomalies of the uterus or Mullerian duct anomalies significantly affect preterm delivery, pregnancy losses, malpresentation, and possibly infertility. While there are many different variants of Mullerian anomalies, septate, arcuate, and bicornuate uteri are the most common types seen in clinical practice. (Figure 18) Bicornuate uterus increases the risk for preterm birth and malpresentation at delivery, whereas septate uterus increases the risk for early miscarriage.[46] When a Mullerian anomaly is suspected on a 2D ultrasound, the American Society for Reproductive Medicine (ASRM) recommends further investigation by performing a saline infusion sonogram with or without 3D reconstruction or hysteroscopy to characterize the anatomy better. Using 3D ultrasound, one can measure the degree of indentation of the protruding medial portion to distinguish between arcuate and septate uteri, which has a reported cut-off ranging between 1.0-1.5cm.[47] 3D ultrasound has similar efficacy as MRI for the diagnosis of congenital anomalies of the uterus.[48]
Importance of tubal Assessment
- The presence of hydrosalpinges reduced live birth rates by 30% due to the reflux of toxic fluid into the endometrium.[49][50] Ultrasound findings of hydrosalpinx include thick or thin-walled, tubular, or contorted S-shaped anechoic fluid-filled structure with partial septa. (Figure 19) Sometimes the hydrosalpinx looks like “beads on a string.” ASRM recommends laparoscopic salpingectomy or proximal tubal occlusion with cautery or partial salpingectomy to improve subsequent pregnancy and live birth rates through IVF in patients with hydrosalpinges.[51]
- Evaluation of tubal patency plays a key role in counseling infertility patients considering IUI or IVF therapies. Sonohysterosalpingogram (HycoSY) is a quick, simple technique to confirm tubal patency rapidly. A combined SIS with 2D or 3D ultrasound can be performed around day 5 through 9 as a “one-stop-shop” infertility evaluation.[52] HyCoSy is comparable to HSG for assessment of tubal patency when compared with the laparoscopic chromopertubation.[53]
Role of Ultrasound in Embryo Transfer
Transabdominal ultrasound is usually used to guide the embryo transfer catheter during embryo transfer. An increase in pregnancy rate from 30.1% to 36.8% was noted when embryo transfer was performed using ultrasound versus clinical touch method.[54][55]
Enhancing Healthcare Team Outcomes
Ultrasound is a safe, reliable, cost-effective, and easily available imaging modality to assess the anatomy and morphology of the female reproductive organs. Performing 2D ultrasound along with SIS, HyCoSy, and 3D ultrasound in one setting can curtail the significant time delay in performing infertility workup. Performing a 2D ultrasound is part of general ob-gyn training, but performing SIS, HyCoSy, 3D ultrasound generally needs additional training. All general obstetricians and gynecologists are not equipped with this special skill. Therefore collaborating with an REI provider or physicians who provide fertility services is important to provide care in a timely and efficient manner.
Patient care coordinators and nurses also play a crucial role in managing infertility patients. The timing of ultrasound is typically precise to the patient’s menstrual cycle. Therefore, scheduling patients for ultrasounds expeditiously is essential to an infertility evaluation. Involving an interprofessional team of providers who can prioritize the patient's needs, provide education and support while navigating their journey to a successful pregnancy can increase patient satisfaction and alleviate burnout for care providers. This interprofessional care coordination involving nurses, physician assistants, nurse practitioners, and physicians can improve patient outcomes.
Media
(Click Image to Enlarge)
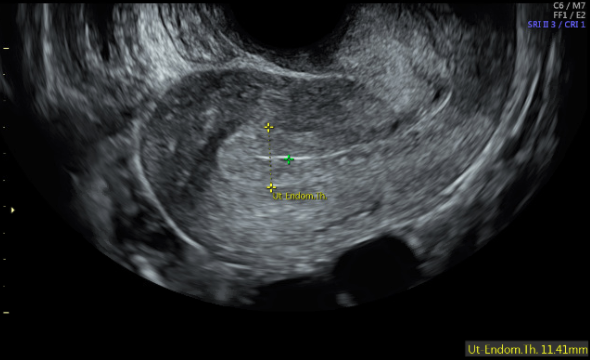
Figure 1: Sagittal view of uterus showing trilaminar endometrium, Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
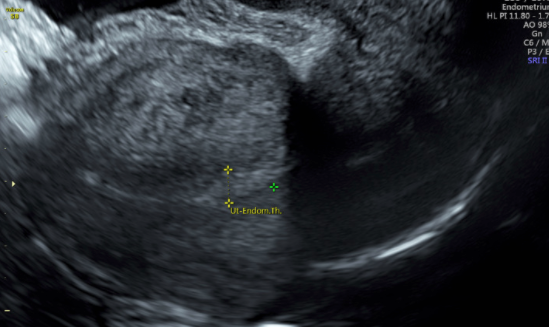
Figure 2: Sagittal view of uterus showing the luteal phase endometrium Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
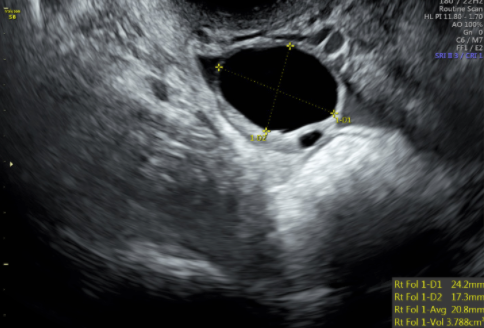
Figure 3: Transvaginal ultrasound image showing the ovary with a dominant follicle before ovulation trigger injection is administered Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
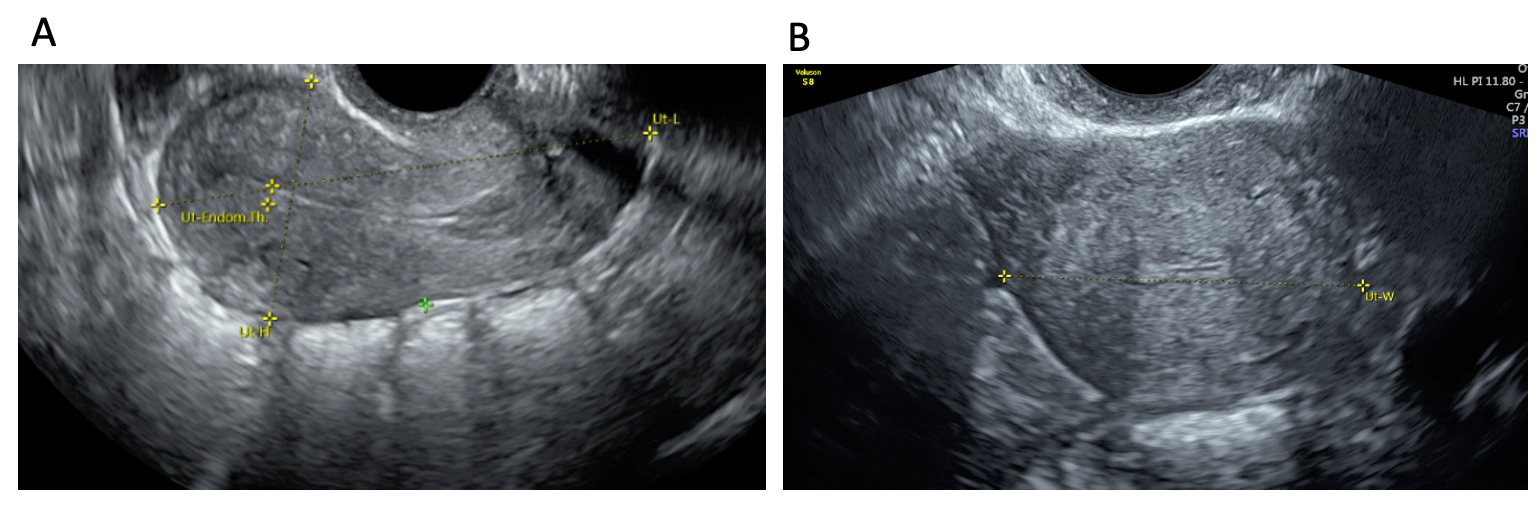
Figure 4: Transvaginal scan showing the uterine measurements in both (A) sagittal and (B) transverse planes Contributed by Jenna Kahn, MD
(Click Image to Enlarge)

Figure 5: Midsagittal view of the uterus with its endometrium being measured perpendicularly from one echogenic to the other echogenic border at its thickest part Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
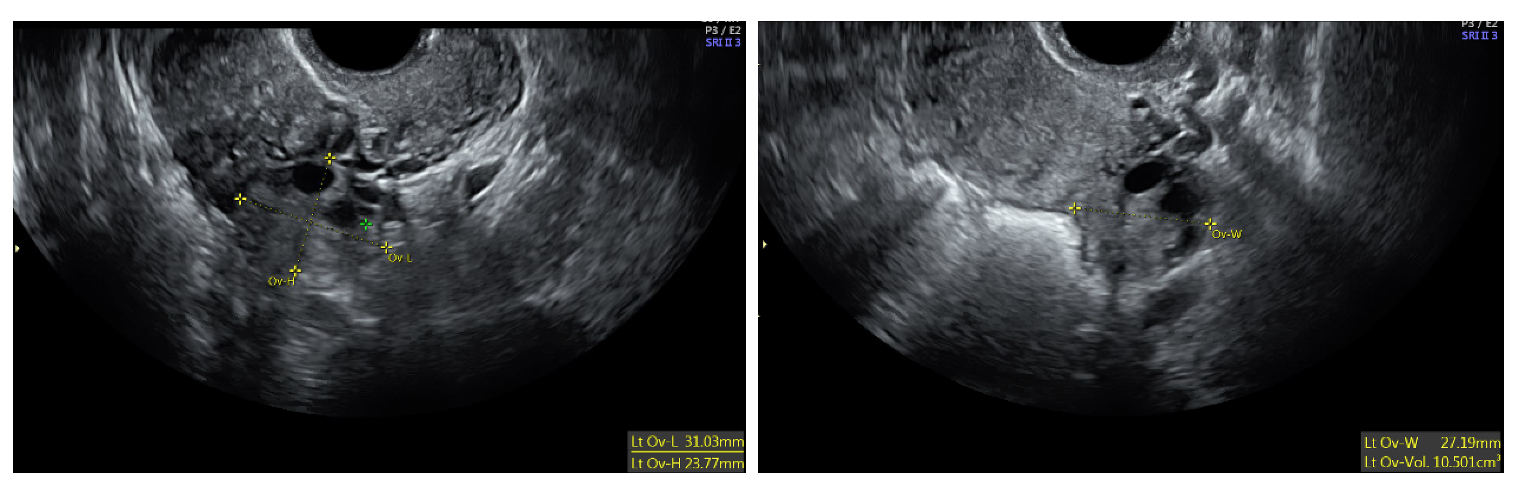
Figure 6: Transvaginal ultrasound image showing ovary and its measurements in three dimensions Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
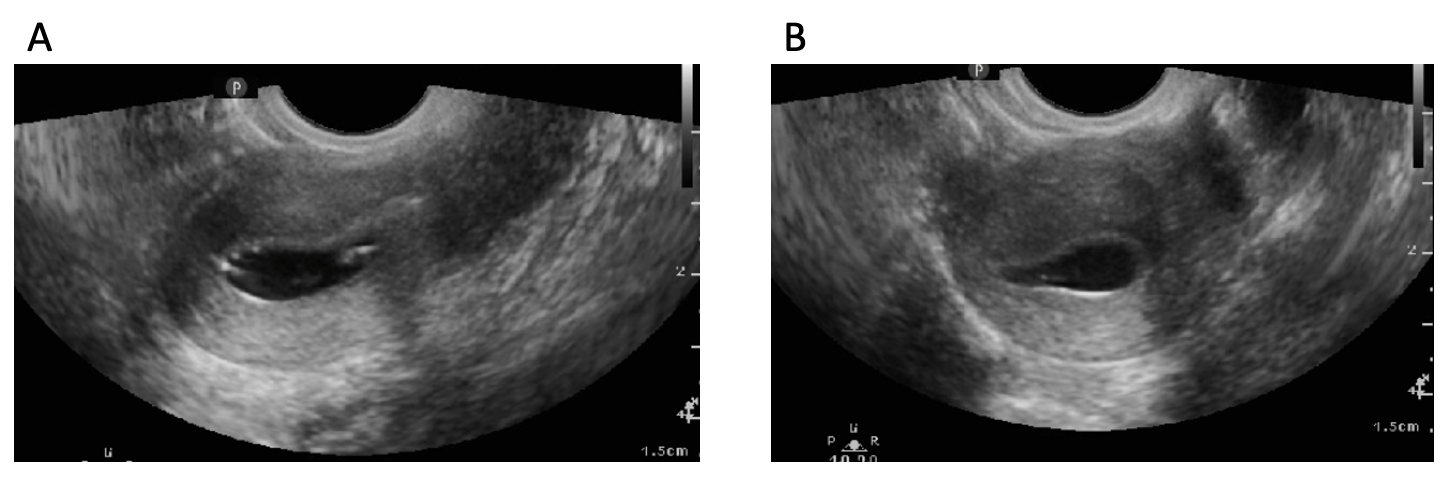
Figure 8: A) sagittal and (B) transverse views of a normal uterine cavity in Saline Infusion Sonogram (SIS) Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
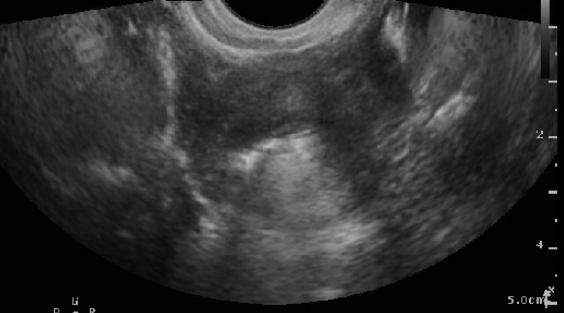
Figure 9: SIS showing patent fallopian tube (hyper-echoic bubbles seen flowing through the cornua and outside of the uterine cavity) Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
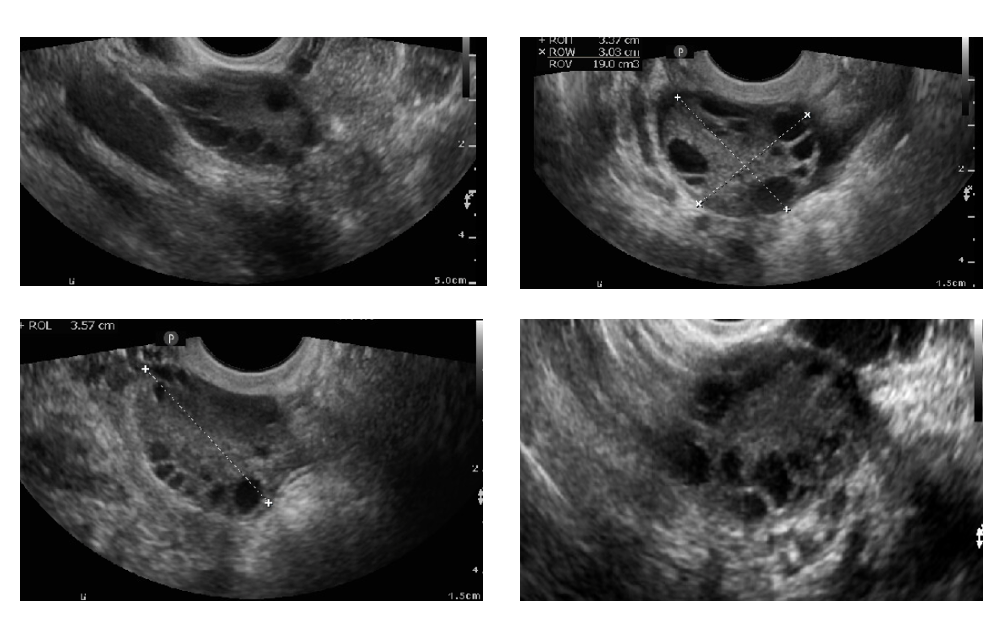
Figure 10: Transvaginal 2D scan showing polycystic ovaries Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
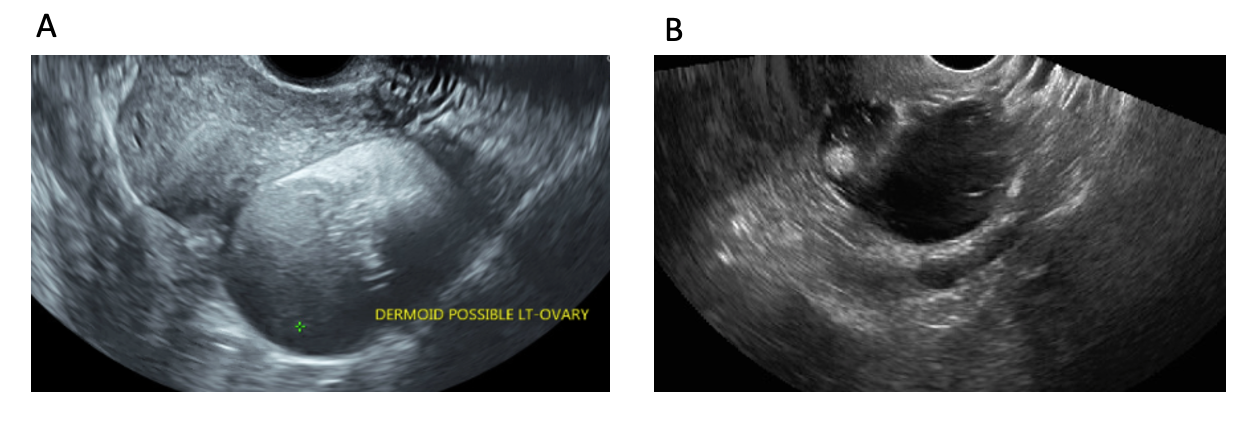
Figure 11: 2D transvaginal scan showing A) cystic teratoma with B) hyper-echoic Rokitansky nodule and hair Figure 11A contributed by Jenna Kahn MD and Figure 11B contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
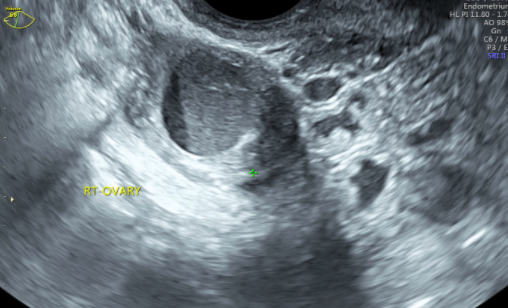
Figure 12: 2D transvaginal scan showing a hemorrhagic cyst or endometrioma Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
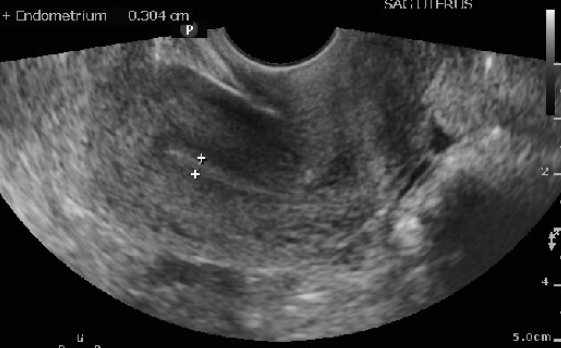
Figure 13: Transvaginal scan of uterus with thin endometrial stripe in a patient using Clomiphene Citrate (CC) Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
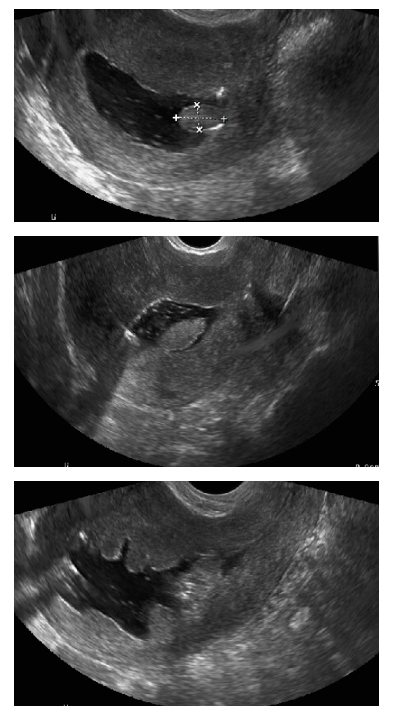
Figure 14: Saline Infusion Sonogram (SIS) showing endometrial polyp Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
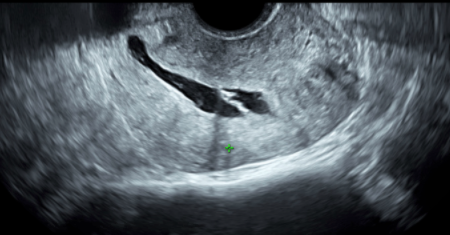
Figure 15: Saline Infusion Sonogram (SIS) showing intrauterine adhesions Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
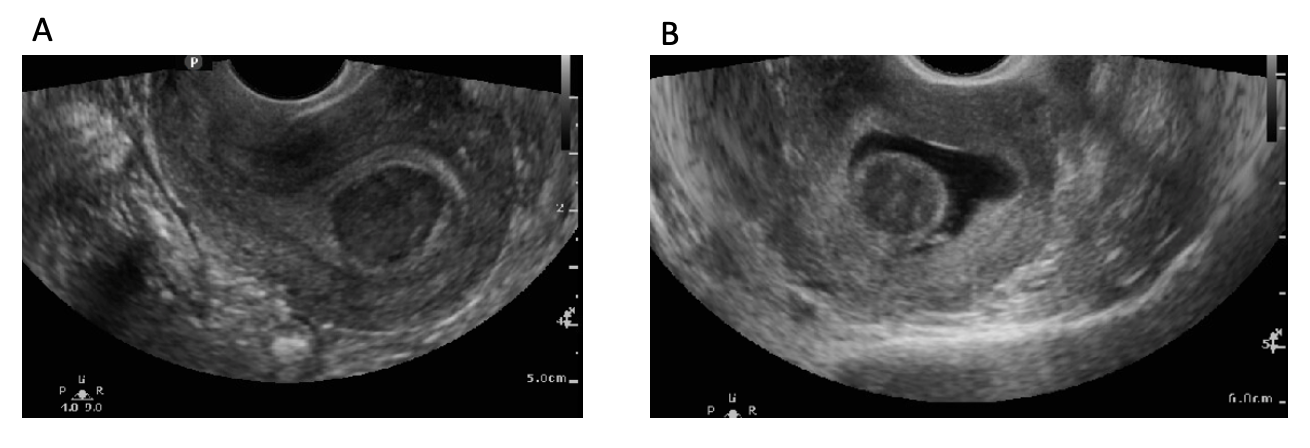
Figure 16: Type 0 submucosal fibroid shown on (A) 2D transvaginal scan and (B) Saline Infusion Sonogram (SIS) Contributed by Laveena Kondagari, MD
(Click Image to Enlarge)
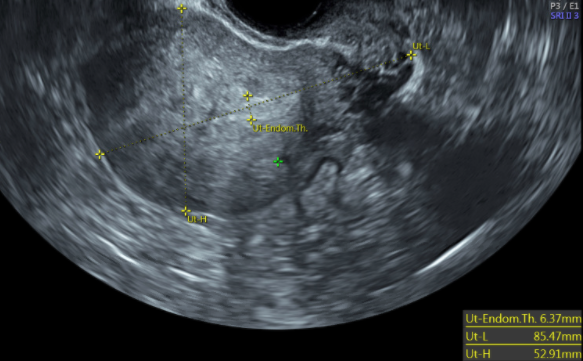
Figure 17: 2D transvaginal scan showing sagittal view of the uterus with adenomyosis Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
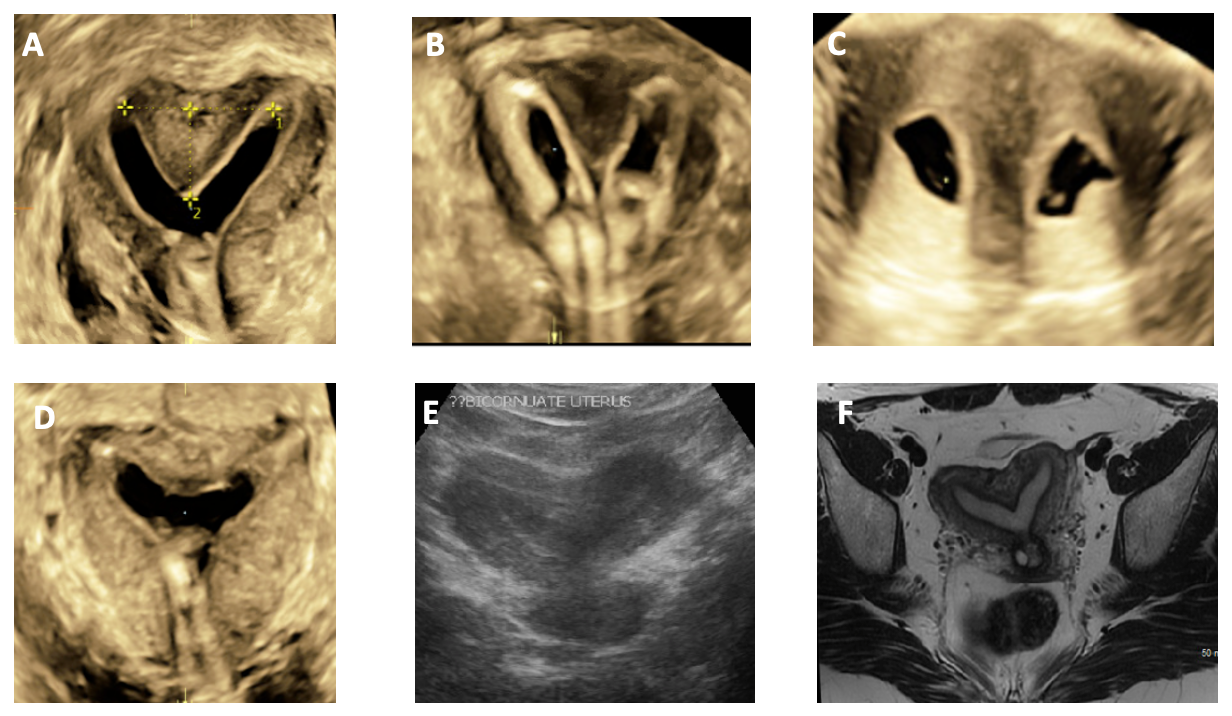
Figure 18: (A) 3D ultrasound coronal view of partial septate uterus, (B) 3D ultrasound coronal view of a complete septate uterus, (C) Ultrasound transverse view of a complete septate uterus, (D) 3D ultrasound coronal view of an arcuate uterus, (E) Ultrasound coronal view of bicornuate uterus, (F) MRI image of bicornuate uterus Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
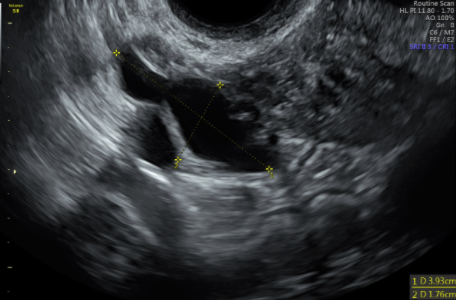
Figure 19: 2D transvaginal ultrasound showing hydrosalpinx Contributed by Jenna Kahn, MD
(Click Image to Enlarge)
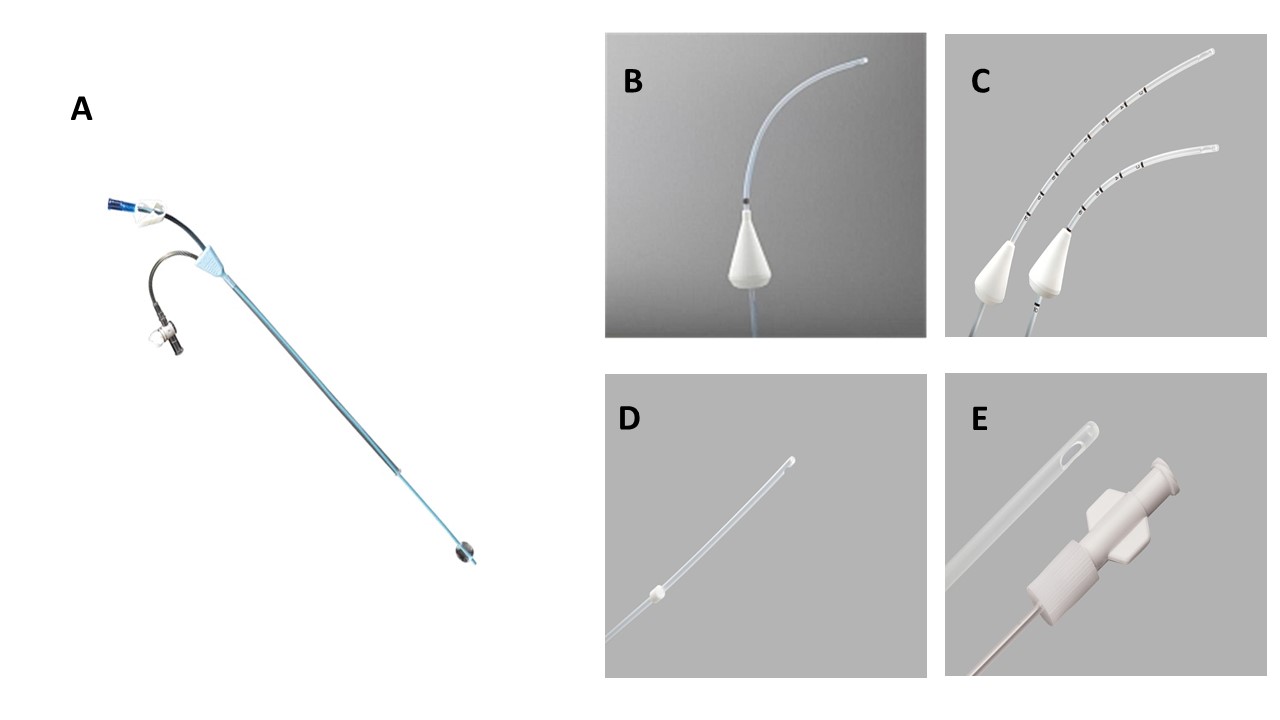
Figure 7: Different types of Catheters used for Saline infusion sonogram (SIS). [A] Ackrad H/S elliptosphere catheter (5 Fr); [B] Goldstein catheter (5.2-5.4 Fr); [C] Goldstein Sonobiopsy catheter (7.2 Fr); [D] Soules catheter (5.3 Fr); [E] Shepard catheter (5.4 Fr). Image A courtesy of Cooper Surgical, Inc. Images B, C, D, E courtesy of Cook Medical.
References
Expert Panel on Women’s Imaging.,Wall DJ,Reinhold C,Akin EA,Ascher SM,Brook OR,Dassel M,Henrichsen TL,Learman LA,Maturen KE,Patlas MN,Robbins JB,Sadowski EA,Saphier C,Uyeda JW,Glanc P, ACR Appropriateness Criteria® Female Infertility. Journal of the American College of Radiology : JACR. 2020 May; [PubMed PMID: 32370955]
Baerwald AR,Pierson RA, Endometrial development in association with ovarian follicular waves during the menstrual cycle. Ultrasound in obstetrics [PubMed PMID: 15343603]
Raine-Fenning NJ,Campbell BK,Clewes JS,Kendall NR,Johnson IR, Defining endometrial growth during the menstrual cycle with three-dimensional ultrasound. BJOG : an international journal of obstetrics and gynaecology. 2004 Sep; [PubMed PMID: 15327609]
Bakos O,Lundkvist O,Wide L,Bergh T, Ultrasonographical and hormonal description of the normal ovulatory menstrual cycle. Acta obstetricia et gynecologica Scandinavica. 1994 Nov; [PubMed PMID: 7817731]
Hershko-Klement A,Tepper R, Ultrasound in assisted reproduction: a call to fill the endometrial gap. Fertility and sterility. 2016 Jun; [PubMed PMID: 27140291]
Leone FP,Timmerman D,Bourne T,Valentin L,Epstein E,Goldstein SR,Marret H,Parsons AK,Gull B,Istre O,Sepulveda W,Ferrazzi E,Van den Bosch T, Terms, definitions and measurements to describe the sonographic features of the endometrium and intrauterine lesions: a consensus opinion from the International Endometrial Tumor Analysis (IETA) group. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2010 Jan [PubMed PMID: 20014360]
Level 3 (low-level) evidenceChien LW,Au HK,Chen PL,Xiao J,Tzeng CR, Assessment of uterine receptivity by the endometrial-subendometrial blood flow distribution pattern in women undergoing in vitro fertilization-embryo transfer. Fertility and sterility. 2002 Aug; [PubMed PMID: 12137858]
Faddy MJ,Gosden RG,Gougeon A,Richardson SJ,Nelson JF, Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Human reproduction (Oxford, England). 1992 Nov; [PubMed PMID: 1291557]
Faddy MJ,Gosden RG, A model conforming the decline in follicle numbers to the age of menopause in women. Human reproduction (Oxford, England). 1996 Jul; [PubMed PMID: 8671489]
Coelho Neto MA,Ludwin A,Borrell A,Benacerraf B,Dewailly D,da Silva Costa F,Condous G,Alcazar JL,Jokubkiene L,Guerriero S,Van den Bosch T,Martins WP, Counting ovarian antral follicles by ultrasound: a practical guide. Ultrasound in obstetrics [PubMed PMID: 29080259]
Klenov VE,VAN Voorhis BJ, Ultrasound in Infertility Treatments. Clinical obstetrics and gynecology. 2017 Mar; [PubMed PMID: 28059846]
Mikolajczyk RT,Stanford JB,Ecochard R, Multilevel model to assess sources of variation in follicular growth close to the time of ovulation in women with normal fertility: a multicenter observational study. Reproductive biology and endocrinology : RB [PubMed PMID: 19077200]
Level 2 (mid-level) evidenceHancock KL,Pereira N,Christos PJ,Petrini AC,Hughes J,Chung PH,Rosenwaks Z, Optimal lead follicle size for human chorionic gonadotropin trigger in clomiphene citrate and intrauterine insemination cycles: an analysis of 1,676 treatment cycles. Fertility and sterility. 2021 Apr; [PubMed PMID: 33272641]
AIUM Practice Parameter for the Performance of a Focused Ultrasound Examination in Reproductive Endocrinology and Female Infertility. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2019 Mar; [PubMed PMID: 30758891]
Hudelist G,Fritzer N,Staettner S,Tammaa A,Tinelli A,Sparic R,Keckstein J, Uterine sliding sign: a simple sonographic predictor for presence of deep infiltrating endometriosis of the rectum. Ultrasound in obstetrics [PubMed PMID: 23400893]
Campbell S, Ultrasound Evaluation in Female Infertility: Part 1, the Ovary and the Follicle. Obstetrics and gynecology clinics of North America. 2019 Dec; [PubMed PMID: 31677749]
O'Neill MJ, Sonohysterography. Radiologic clinics of North America. 2003 Jul; [PubMed PMID: 12899492]
Jayaprakasan K,Chan Y,Islam R,Haoula Z,Hopkisson J,Coomarasamy A,Raine-Fenning N, Prediction of in�vitro fertilization outcome at different antral follicle count thresholds in a prospective cohort of 1,012 women. Fertility and sterility. 2012 Sep; [PubMed PMID: 22749225]
Level 2 (mid-level) evidenceDepmann M,Broer SL,van der Schouw YT,Tehrani FR,Eijkemans MJ,Mol BW,Broekmans FJ, Can we predict age at natural menopause using ovarian reserve tests or mother's age at menopause? A systematic literature review. Menopause (New York, N.Y.). 2016 Feb; [PubMed PMID: 26372034]
Level 1 (high-level) evidenceWellons MF,Bates GW,Schreiner PJ,Siscovick DS,Sternfeld B,Lewis CE, Antral follicle count predicts natural menopause in a population-based sample: the Coronary Artery Risk Development in Young Adults Women's Study. Menopause (New York, N.Y.). 2013 Aug; [PubMed PMID: 23422869]
Wittmaack FM,Kreger DO,Blasco L,Tureck RW,Mastroianni L Jr,Lessey BA, Effect of follicular size on oocyte retrieval, fertilization, cleavage, and embryo quality in in vitro fertilization cycles: a 6-year data collection. Fertility and sterility. 1994 Dec; [PubMed PMID: 7957985]
Level 2 (mid-level) evidenceEvans MB,Stentz NC,Richter KS,Schexnayder B,Connell M,Healy MW,Devine K,Widra E,Stillman R,DeCherney AH,Hill MJ, Mature Follicle Count and Multiple Gestation Risk Based on Patient Age in Intrauterine Insemination Cycles With Ovarian Stimulation. Obstetrics and gynecology. 2020 May; [PubMed PMID: 32282611]
Teede HJ,Misso ML,Costello MF,Dokras A,Laven J,Moran L,Piltonen T,Norman RJ,International PCOS Network., Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertility and sterility. 2018 Aug; [PubMed PMID: 30033227]
Level 1 (high-level) evidenceZhao J,Zhang Q,Li Y, The effect of endometrial thickness and pattern measured by ultrasonography on pregnancy outcomes during IVF-ET cycles. Reproductive biology and endocrinology : RB [PubMed PMID: 23190428]
Level 2 (mid-level) evidenceFleischer AC,Pittaway DE,Beard LA,Thieme GA,Bundy AL,James AE Jr,Wentz AC, Sonographic depiction of endometrial changes occurring with ovulation induction. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 1984 Aug; [PubMed PMID: 6434749]
Wu Y,Gao X,Lu X,Xi J,Jiang S,Sun Y,Xi X, Endometrial thickness affects the outcome of in vitro fertilization and embryo transfer in normal responders after GnRH antagonist administration. Reproductive biology and endocrinology : RB [PubMed PMID: 25296555]
Level 2 (mid-level) evidenceTraub ML,Van Arsdale A,Pal L,Jindal S,Santoro N, Endometrial thickness, Caucasian ethnicity, and age predict clinical pregnancy following fresh blastocyst embryo transfer: a retrospective cohort. Reproductive biology and endocrinology : RB [PubMed PMID: 19386129]
Level 2 (mid-level) evidenceZhang T,Li Z,Ren X,Huang B,Zhu G,Yang W,Jin L, Endometrial thickness as a predictor of the reproductive outcomes in fresh and frozen embryo transfer cycles: A retrospective cohort study of 1512 IVF cycles with morphologically good-quality blastocyst. Medicine. 2018 Jan; [PubMed PMID: 29369190]
Level 2 (mid-level) evidenceWang L,Qiao J,Li R,Zhen X,Liu Z, Role of endometrial blood flow assessment with color Doppler energy in predicting pregnancy outcome of IVF-ET cycles. Reproductive biology and endocrinology : RB&E. 2010 Oct 18 [PubMed PMID: 20955593]
Level 2 (mid-level) evidenceZaidi J,Campbell S,Pittrof R,Tan SL, Endometrial thickness, morphology, vascular penetration and velocimetry in predicting implantation in an in vitro fertilization program. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 1995 Sep [PubMed PMID: 8521069]
Richter KS,Bugge KR,Bromer JG,Levy MJ, Relationship between endometrial thickness and embryo implantation, based on 1,294 cycles of in vitro fertilization with transfer of two blastocyst-stage embryos. Fertility and sterility. 2007 Jan [PubMed PMID: 17081537]
Level 2 (mid-level) evidenceMunro MG, Uterine polyps, adenomyosis, leiomyomas, and endometrial receptivity. Fertility and sterility. 2019 Apr [PubMed PMID: 30929720]
Soares SR,Barbosa dos Reis MM,Camargos AF, Diagnostic accuracy of sonohysterography, transvaginal sonography, and hysterosalpingography in patients with uterine cavity diseases. Fertility and sterility. 2000 Feb [PubMed PMID: 10685551]
Farquhar C,Ekeroma A,Furness S,Arroll B, A systematic review of transvaginal ultrasonography, sonohysterography and hysteroscopy for the investigation of abnormal uterine bleeding in premenopausal women. Acta obstetricia et gynecologica Scandinavica. 2003 Jun [PubMed PMID: 12780419]
Level 1 (high-level) evidenceHinckley MD,Milki AA, 1000 office-based hysteroscopies prior to in vitro fertilization: feasibility and findings. JSLS : Journal of the Society of Laparoendoscopic Surgeons. 2004 Apr-Jun [PubMed PMID: 15119651]
Level 2 (mid-level) evidenceAmerican Association of Gynecologic Laparoscopists., AAGL practice report: practice guidelines for the diagnosis and management of endometrial polyps. Journal of minimally invasive gynecology. 2012 Jan-Feb [PubMed PMID: 22196255]
Level 1 (high-level) evidenceAmin TN,Saridogan E,Jurkovic D, Ultrasound and intrauterine adhesions: a novel structured approach to diagnosis and management. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2015 Aug [PubMed PMID: 26094824]
Bajekal N,Li TC, Fibroids, infertility and pregnancy wastage. Human reproduction update. 2000 Nov-Dec; [PubMed PMID: 11129696]
Casini ML,Rossi F,Agostini R,Unfer V, Effects of the position of fibroids on fertility. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology. 2006 Feb [PubMed PMID: 16603437]
Level 2 (mid-level) evidenceSomigliana E,Vercellini P,Daguati R,Pasin R,De Giorgi O,Crosignani PG, Fibroids and female reproduction: a critical analysis of the evidence. Human reproduction update. 2007 Sep-Oct [PubMed PMID: 17584819]
Sunkara SK,Khairy M,El-Toukhy T,Khalaf Y,Coomarasamy A, The effect of intramural fibroids without uterine cavity involvement on the outcome of IVF treatment: a systematic review and meta-analysis. Human reproduction (Oxford, England). 2010 Feb [PubMed PMID: 19910322]
Level 1 (high-level) evidencePractice Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org.,Practice Committee of the American Society for Reproductive Medicine., Removal of myomas in asymptomatic patients to improve fertility and/or reduce miscarriage rate: a guideline. Fertility and sterility. 2017 Sep [PubMed PMID: 28865538]
Sakhel K,Abuhamad A, Sonography of adenomyosis. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2012 May [PubMed PMID: 22535729]
Meredith SM, Sanchez-Ramos L, Kaunitz AM. Diagnostic accuracy of transvaginal sonography for the diagnosis of adenomyosis: systematic review and metaanalysis. American journal of obstetrics and gynecology. 2009 Jul:201(1):107.e1-6. doi: 10.1016/j.ajog.2009.03.021. Epub 2009 Apr 26 [PubMed PMID: 19398089]
Level 1 (high-level) evidenceBazot M,Cortez A,Darai E,Rouger J,Chopier J,Antoine JM,Uzan S, Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Human reproduction (Oxford, England). 2001 Nov; [PubMed PMID: 11679533]
Chan YY,Jayaprakasan K,Tan A,Thornton JG,Coomarasamy A,Raine-Fenning NJ, Reproductive outcomes in women with congenital uterine anomalies: a systematic review. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2011 Oct [PubMed PMID: 21830244]
Level 1 (high-level) evidenceCarbonnel M,Pirtea P,de Ziegler D,Ayoubi JM, Uterine factors in recurrent pregnancy losses. Fertility and sterility. 2021 Mar [PubMed PMID: 33712099]
Deutch TD, Abuhamad AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of müllerian duct anomalies: a review of the literature. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2008 Mar:27(3):413-23 [PubMed PMID: 18314520]
de Wit W,Gowrising CJ,Kuik DJ,Lens JW,Schats R, Only hydrosalpinges visible on ultrasound are associated with reduced implantation and pregnancy rates after in-vitro fertilization. Human reproduction (Oxford, England). 1998 Jun [PubMed PMID: 9688415]
Cohen MA,Lindheim SR,Sauer MV, Hydrosalpinges adversely affect implantation in donor oocyte cycles. Human reproduction (Oxford, England). 1999 Apr; [PubMed PMID: 10221245]
Level 2 (mid-level) evidencePractice Committee of American Society for Reproductive Medicine in collaboration with Society of Reproductive Surgeons., Salpingectomy for hydrosalpinx prior to in vitro fertilization. Fertility and sterility. 2008 Nov [PubMed PMID: 19007649]
Groszmann YS,Benacerraf BR, Complete evaluation of anatomy and morphology of the infertile patient in a single visit; the modern infertility pelvic ultrasound examination. Fertility and sterility. 2016 Jun [PubMed PMID: 27054310]
Luciano DE,Exacoustos C,Luciano AA, Contrast ultrasonography for tubal patency. Journal of minimally invasive gynecology. 2014 Nov-Dec [PubMed PMID: 24910933]
Level 3 (low-level) evidenceSallam HN,Sadek SS, Ultrasound-guided embryo transfer: a meta-analysis of randomized controlled trials. Fertility and sterility. 2003 Oct; [PubMed PMID: 14556831]
Level 1 (high-level) evidenceCozzolino M,Vitagliano A,Di Giovanni MV,Lagan� AS,Vitale SG,Blaganje M,Drusany Stari? K,Borut K,Patrelli TS,Noventa M, Ultrasound-guided embryo transfer: summary of the evidence and new perspectives. A systematic review and meta-analysis. Reproductive biomedicine online. 2018 May; [PubMed PMID: 29576332]
Level 3 (low-level) evidence