 Ultrasound Adult Echocardiography Assessment, Protocols, and Interpretation
Ultrasound Adult Echocardiography Assessment, Protocols, and Interpretation
Introduction
Echocardiography is a non-invasive diagnostic modality to examine the structure and function of the heart and great vessels. In 1950, the German scientist, Wolfe Dieter Keidel, utilize the transmitted ultrasonic wave technique to study the heart. However, he was not able able to create information regarding cardiac function.[1]
In 1953, Dr. Inge, the father of echocardiography and inventor of M-Mode, and Dr. Helmut Hertz established a commercial ultrasound machine to study the heart.[2] The development of echocardiography modalities such as M-Mode, A-mode, Doppler, transthoracic, transesophageal, contrast, stress echocardiography, and strain imaging took decades and helped achieve prompt diagnoses of various cardiac illnesses.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Transthoracic Echocardiography views and anatomy:[3]
Parasternal Long-axis View (Figure 1)
Structures
- Chambers identified in this view: left atrium, left ventricle, left ventricle outflow tract, aorta.
- Valves identified in this view: mitral valve and aortic valve
- This view helps in identifying regurgitant and stenotic jets of mitral and aortic valves.[4]
Parasternal Short-axis View
Structures
- Chambers identified in this view: left atrium, right atrium, right ventricle outflow tract, main pulmonary artery
- Valves identified in this view: aortic valve, pulmonary valve, tricuspid valve
- This view helps in identifying the tricuspid and pulmonary valve disease as well as patent ductus arteriosus.
Apical 4 Chamber View (Figure 2)
Structures
- Chambers identified in this view: left atrium, right atrium, left ventricle, and right ventricle
- Valves identified in this view: mitral and tricuspid valve
- This view helps identify the wall motion abnormalities of the inferior septal wall and anterolateral wall of the left ventricle, mitral, and tricuspid valve disease.
Apical 5 Chamber View
Structures
- Chambers identified in this view: left atrium, right atrium, left ventricle, left ventricle outflow tract, right ventricle, and aorta
- Valves identified in this view: mitral valve, tricuspid valve, and aortic valve
- This view provides additional information on the Left ventricle outflow tract, aortic valve, and aortic root compared to the four-chamber view.
Apical 2 Chamber View (Figure 3)
Structures
- Chambers identified in this view: left atrium and left ventricle
- Valves identified in this view: mitral valve
- This view helps identify the wall motion abnormalities of the inferior wall and anterior wall of the left ventricle and mitral valve disease.
Apical Parasternal long-axis View (Figure 4)
Structures
- Chambers identified in this view: left atrium, left ventricle, left ventricle outflow tract, aorta.
- Valves identified in this view: mitral valve and aortic valve
- This view helps identify the wall motion abnormalities of the anterior septal wall and the inferolateral wall of the left ventricle. In this view, mitral valve and aortic valve disease are identifiable.
Subcostal Coronal View
Structures
- Chambers identified in this view: left atrium, right atrium, left ventricle, and right ventricle
- Valves identified in this view: mitral and tricuspid valve
- This view helps in diagnosing interatrial septal defect, pericardial effusion, and cardiac tamponade.
Subcostal Saggital view
Structures
- Chambers identified in this view: right atrium, inferior vena cava, hepatic vein, and descending aorta
- This view helps in assessing the fluid status of the patient.
Suprasternal Noch View
Structures
- Chambers identified in this view: left atrium, aortic arch, brachiocephalic artery, left common carotid artery, left subclavian artery, right pulmonary artery.
- This view helps in diagnosing aorta diseases such as aortic dissection and coarctation of the aorta. In this view, congenital heart defect, patent ductus arteriosus can be identified.
Indications
Appropriate Use And Indication Criteria for Echocardiography According to ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/ SCCT/SCMR 2011[5][6]
- Symptoms related to cardiac diseases such as chest pain, shortness of breath, syncope, palpitations, transient ischemic attack, stroke, and peripheral embolic event
- Previous diagnostic tests such as cardiac enzymes, electrocardiogram, and chest X-ray indicating cardiac disease
- Premature ventricular contraction ( Frequent or exercise-induced)
- Arrhythmias such as Atrial fibrillation, Atrioventricular node re-entry tachycardia, and Ventricular tachycardia (sustained or non-sustained)
- Evaluation of right ventricular function (fractional area change, tricuspid annular plane systolic excursion(TAPSE), Right index of myocardial performance (RIMP), and pulmonary artery pressure in a patient with suspected pulmonary artery hypertension
- Routine follow-up of patients as surveillance (>1 year) for diagnosed pulmonary artery hypertension patients without a change in symptoms or physical examination
- To guide management in patients diagnosed with pulmonary artery hypertension and change in cardiac symptoms or physical examination
- Patient in shock with an uncertain or suspected cardiac cause
- For evaluation pf patient with a suspicion of myocardial infarction either with chest pain or diagnostic tests such as cardiac enzymes and electrocardiogram indicating of myocardial infarction
- For diagnosis of valvular heart disease
- To guide management in patients diagnosed with valvular heart disease and change in cardiac symptoms or physical examination.
- Patients with suspicion of hypertensive heart disease, prosthetic valve dysfunction, infective endocarditis, heart failure, congenital heart disease, cardiac mass, pericardial disease, aortic aneurysm, aortic dissection, or cardiovascular source of embolus
Indication for Transesophageal Echocardiography
- Transthoracic echo nondiagnostic due to patient characteristics
- To guide percutaneous noncoronary cardiac interventions such as closure device placement, radiofrequency ablation, and percutaneous valve procedures.
- To rule out cardiovascular sources such as embolus in patients with no other non-cardiac cause.
- To provide help in the decision-making of cardioversion, anticoagulation, and ablation in atrial flutter or atrial fibrillation.
- To diagnose infective endocarditis in patients with moderate-high pretest probability.
Indication for Stress Echocardiography
- Patients with intermediate and high pre-test probability for coronary artery disease
- Patients with a possible acute coronary syndrome (electrocardiogram: no ischemic changes or with LBBB or electronically paced ventricular rhythm, low-risk TIMI score with either borderline or minimally elevated troponin, High-risk TIMI score with negative troponin)
Contraindications
According to ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/ SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography, Inappropriate Transthoracic Echocardiography Indications
- Patients with asymptomatic sinus bradycardia
- Patients with infrequent Atrial premature contractions or Ventricular premature contractions
- Patients with presyncope and no other evidence of cardiac disease
- Evaluation of left ventricle function for Pre-operative screening in patients without symptoms or signs of cardiac disease
- Routine follow-up of patients as surveillance (<1 year) for diagnosed pulmonary artery hypertension patients without a change in symptoms or physical examination
- Routine follow-up of patients as surveillance in patients with a previous history of pulmonary embolism with normal right ventricular function and pulmonary artery systolic pressure
Absolute Contraindications Of Transesophageal Echocardiography
- History of esophageal stricture, perforation, tumor, laceration, and diverticulum
- History of upper gastrointestinal bleeding
- Severe atlantoaxial joint disorder
- Conditions that prevent neck flexion
Inappropriate Transesophageal Echocardiography Indications
- Routine use of transesophageal echocardiography in patients in whom decision regarding diagnosis and management already resolved by transthoracic echocardiography
- To diagnose infective endocarditis in patients with low pretest probability.
- To rule out cardiovascular source as embolus in patients with an obvious cardiac cause.
- Patients with atrial fibrillation or atrial flutter in whom the decision to anticoagulant already made
Conditions In Which Stress Echocardiography Are Inappropriate
- Patients with low pre-test probability for coronary artery disease
- Patients with definite acute coronary syndrome
Equipment
Equipment Requirement for Transthoracic Echocardiography[7]
- Echocardiography machine
- Transducer
- Contrast agent
Equipment Requirement for Transesophageal Echocardiography[8]
- Echocardiography machine
- Transesophageal Transducer
- Medication for Sedation
- Transesophageal bite block
- Intravenous cannula for medications
- For the bubble study, requirements are agitated saline, Three way stop cock, two 10 ml syringes, Extension tube connector)
- Gel to lubricate Transesophageal probe
- Topic anesthetic such as lidocaine to numb the pharynx
Equipment Requirement for Stress Echocardiography
- Echocardiography machine
- Exercise stress test machine
- Cardiac monitor to look for vitals
- Medications (such as dobutamine and atropine) to give stress in patients who can not perform an exercise stress test and medications ( such as Beta-blockers and calcium channel blockers) to reverse the effect of dobutamine and atropine
Personnel
- Cardiologist
- Echo technician
Technique or Treatment
For transthoracic echocardiography, the patient should lie in the left lateral position.
Complications
The complications from transthoracic echocardiography and stress echocardiography are infrequent.
Transesophageal Echocardiography[9][10]
- Gastrointestinal bleeding
- Esophageal perforation
- Pharyngeal hematoma
- Aspiration
- Laryngospasm
- Arrhythmia
- Toxic methemoglobinemia
Stress Echocardiography[11][12]
- Myocardial infarction
- Arrhythmia
- Coronary spasm
- Hypertension or hypotension secondary to medication
Clinical Significance
Transthoracic echocardiography is a non-invasive test, low-cost, widely available, a first-line diagnostic test to evaluate cardiac disease and function. It not only helps to diagnose cardiac disease but also provides useful information to guide therapy.
Transesophageal Echocardiography: It is an invasive test done in the condition in which transthoracic echo is inconclusive or need further information on disease such as infective endocarditis. The esophagus's proximity to the heart and absence of intervening structures such as the lung make the Transesophageal echo ideal for examining various important structures.
Stress Echocardiography: The inclusion of imaging in routine stress testing increase both sensitivity and specificity of the test to diagnose coronary artery disease. Stress echocardiography post-myocardial infarction help in risk stratification, location, and extent of coronary artery disease. Stress echocardiography can also be used to risk-stratify patients before non-cardiac surgery as resting echo does not provide essential prognostic information.
Enhancing Healthcare Team Outcomes
To perform echocardiography requires an interprofessional team that includes a cardiologist and an echo technician. It is vital to take a proper history and to perform a physical examination pre-procedure to determine the indication of the procedure. Communication between echo technicians and the cardiologist is essential, especially when there is a discrepancy in results.
Media
(Click Image to Enlarge)
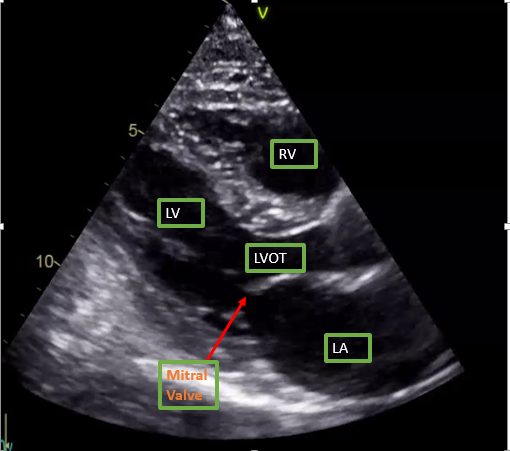
Parasternal long axis view on Transthoracic echocardiogram Contributed by Ghufran Adnan
(Click Image to Enlarge)
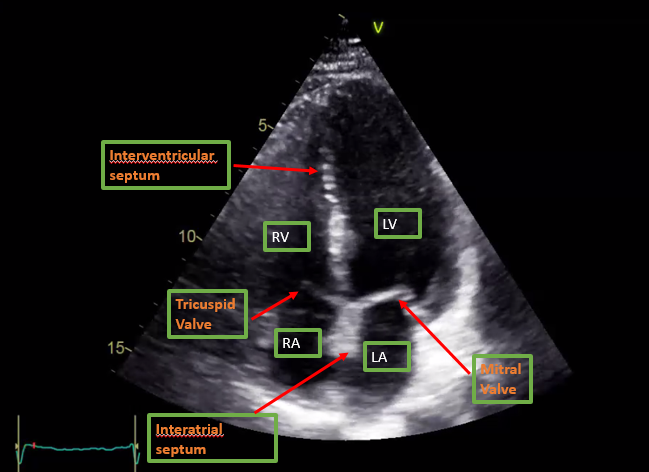
Apical Four chamber view on Transthoracic echocardiography Contributed by Ghufran Adnan
(Click Image to Enlarge)
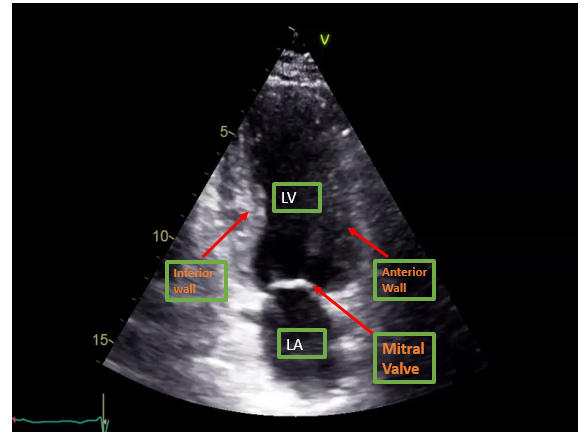
Apical Two chamber view on Transthoracic Echocardiography Contributed by Ghufran Adnan
(Click Image to Enlarge)
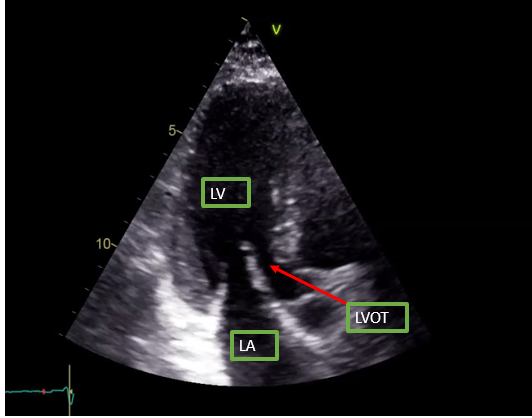
Apical parasternal long axis on Transthoracic echocardiography Contributed by Ghufran Adnan
References
Nixdorff U. The inaugurator of transmitted echocardiography: Prof. Dr Wolf-Dieter Keidel. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2009 Jan:10(1):48-9. doi: 10.1093/ejechocard/jen233. Epub 2008 Oct 15 [PubMed PMID: 18922817]
Acierno LJ, Worrell LT. Inge Edler: father of echocardiography. Clinical cardiology. 2002 Apr:25(4):197-9 [PubMed PMID: 12000080]
Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster MC, Horton K, Ogunyankin KO, Palma RA, Velazquez EJ. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2019 Jan:32(1):1-64. doi: 10.1016/j.echo.2018.06.004. Epub 2018 Oct 1 [PubMed PMID: 30282592]
Thomas JD. Doppler echocardiographic assessment of valvar regurgitation. Heart (British Cardiac Society). 2002 Dec:88(6):651-7 [PubMed PMID: 12433911]
Rao G, Sajnani N, Kusnetzky LL, Main ML. Appropriate use of transthoracic echocardiography. The American journal of cardiology. 2010 Jun 1:105(11):1640-2. doi: 10.1016/j.amjcard.2010.01.026. Epub [PubMed PMID: 20494676]
American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American College of Chest Physicians, Douglas PS, Garcia MJ, Haines DE, Lai WW, Manning WJ, Patel AR, Picard MH, Polk DM, Ragosta M, Parker Ward R, Weiner RB. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance American College of Chest Physicians. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2011 Mar:24(3):229-67. doi: 10.1016/j.echo.2010.12.008. Epub [PubMed PMID: 21338862]
Hillis GS, Bloomfield P. Basic transthoracic echocardiography. BMJ (Clinical research ed.). 2005 Jun 18:330(7505):1432-6 [PubMed PMID: 15961816]
Prabhu M, Raju D, Pauli H. Transesophageal echocardiography: instrumentation and system controls. Annals of cardiac anaesthesia. 2012 Apr-Jun:15(2):144-55. doi: 10.4103/0971-9784.95080. Epub [PubMed PMID: 22508208]
Côté G, Denault A. Transesophageal echocardiography-related complications. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2008 Sep:55(9):622-47. doi: 10.1007/BF03021437. Epub [PubMed PMID: 18840593]
Min JK, Spencer KT, Furlong KT, DeCara JM, Sugeng L, Ward RP, Lang RM. Clinical features of complications from transesophageal echocardiography: a single-center case series of 10,000 consecutive examinations. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2005 Sep:18(9):925-9 [PubMed PMID: 16153515]
Level 1 (high-level) evidenceHirano Y, Yamamoto T, Uehara H, Nakamura H, Wufuer M, Yamada S, Ikawa H, Ishikawa K. [Complications of stress echocardiography]. Journal of cardiology. 2001 Aug:38(2):73-80 [PubMed PMID: 11525112]
Mertes H, Sawada SG, Ryan T, Segar DS, Kovacs R, Foltz J, Feigenbaum H. Symptoms, adverse effects, and complications associated with dobutamine stress echocardiography. Experience in 1118 patients. Circulation. 1993 Jul:88(1):15-9 [PubMed PMID: 8319327]