 Nuclear Medicine PET/CT Gastrointestinal Assessment, Protocols, and Interpretation
Nuclear Medicine PET/CT Gastrointestinal Assessment, Protocols, and Interpretation
Introduction
Gastrointestinal malignancies are a group of heterogeneous neoplasms encompassing diverse biological and physical behavior. The management options for these tumors vary based on their location, cell type, and growth pattern. Early precise diagnosis and accurate staging are critical to instituting appropriate treatment. Recent advancements in the imaging techniques for evaluating solid and hollow viscous organs have enabled the non-invasive assessment of these tumors, although histopathology remains the gold standard. Despite these refinements, no single imaging modality provides sufficient information, and often multiple investigations are judicially combined to offer strength from one modality where the other is lacking.[1]
Positron emission tomography/Computerized tomography (PET/CT) is a hybrid molecular imaging technique that combines the functional imaging advantages of PET with anatomical imaging from CT. The cancerous cells of the gastrointestinal tract (GIT) demonstrate preferential glucose metabolism to lactate in both aerobic and anaerobic environments; a phenomenon called the Warburg effect.[2]
The energy produced through this pathway is insufficient to meet the demand of increasing growth resulting in a rise in their glucose requirement. The oncogenes on the cell structures and growth factors activated by malignant cells trigger glycolysis through upregulation of GLUT-1 transporters and cellular hexokinase, forming the biochemical basis of FDG-PET imaging.
Fluorine-18 labeled deoxyglucose (FDG) is an analog of glucose that accumulates in the cancerous cells but, unlike glucose, cannot be channeled towards ATP production. This entrapment of FDG in cancerous and some inflammatory cells is responsible for image production in PET scanning. The Gallium PET/CT imaging, in contrast, relies on overexpression of somatostatin receptors in the well-differentiated neuroendocrine tumors and thus offers an exquisite assessment of the selected primary neuroendocrine tumors and their metastases.[3]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Esophagus and Gastroesophageal Junction (GOJ)
Optimum treatment planning of esophageal cancers requires an accurate description of cancer location in upper GI tumors, which is impossible without a clear understanding of the segmental esophageal anatomy. Anatomical levels for these cancers are reported relative to anatomical landmarks set by the American Joint Committee on Cancer staging system (AJCC). The esophagus is divided into four segments. This delineation is vital to ensure that the tumor is covered in its entirety in the radiotherapy field. If surgical resection is planned, the choice of approach is appropriate for the tumor's location. For the localization of gastroesophageal junction (GOJ) tumors, the Siewert-Stein classification divides these cancers into three groups based on their epicenter relative to GOJ. Regional lymph nodes for the esophagus include supraclavicular, peri-esophageal, and celiac nodes.[4]
Large Intestine
The large intestine extends from the cecum to the anal verge, where the stratified squamous epithelium of the anal canal meets the anal skin. For colorectal cancers, the relation of the tumor with peritoneal reflection has high prognostic implications as the involvement of the peritoneum makes it a T4a disease and increases the incidence of peritoneal metastases.[5]
The parietal peritoneum covering the abdominal wall reflects anteriorly on the cecum, ascending and descending colon as visceral peritoneum, leaving their posterior circumference uncovered. The transverse and sigmoid colon are near completely intraperitoneal except for the area along the route of mesenteric vessels. The reflection of the peritoneum on the pelvic structures forms the rectouterine pouch in females and rectovesical pouch in males and partially covers the pelvic sidewall on either side. The rectum is thus covered anteriorly and laterally by the peritoneum in the upper part and only anteriorly in the middle part. The lower part of the rectum is entirely free of the peritoneum.
The anal canal is the terminal part of the GI tract and extends from the anorectal junction above (where the rectum passes through the pelvic diaphragm) to the anal verge below. It approximately measures 4 cm and has two crucial muscle layers. The inner layer, which is the continuation of the GI tract's circular muscle, forms the internal sphincter. The outer layer from the downward continuation of the levator ani and puborectalis forms the external sphincter with a small inter-sphincteric space between the two.
Nodal metastases from the colon follow the mesenteric vessels to either the SMA origin in the right colonic tumors or the IMA origin in the left colonic tumors and can then involve the para-aortic nodes. Rectal tumors drain in the mesorectal nodes to the superior rectal artery nodes, and then along the root of sigmoid mesentery can reach para-aortic nodes. They can also drain into internal iliac nodes.
Anal cancer spread has a greater predilection for the lymphatic system than the bloodstream.[6] The cancers above the dentate line follow the drainage pathway of rectal tumors. The cancers below the dentate line drain into the external iliac system through inguinal and femoral nodes.
Neuroendocrine Tumors
The Gastroenteropancreatic neuroendocrine tumors (GEP-NETs) are a group of heterogeneous neoplasms that arise from embryonal neural crest cells. These can arise from virtually any part of the GI tract, but the small intestine is the most common location. These tumors can exhibit broad clinical behavior ranging from indolent, slow-growing to highly aggressive behavior. This clinical behavior correlates with their cellular proliferation rate measured through immunohistochemical staining of a unique Ki67 protein.
Based on the Ki67 index, these tumors are divided into three grades according to the European Neuroendocrine Tumour Society and World Health Organization 2010 Classification Systems for NETs. Grade 1 tumors are well-differentiated with a ki67 index of <2% and show indolent behavior. Grade 3 tumors are poorly differentiated with a ki67 index of >20% and show aggressive clinical behavior. The Grade 2 moderately differentiated tumors have a behavior and proliferation profile between these two extremes.[7][8]
Radiotracers for PET/CT Imaging
Fluorine-18 combined with deoxyglucose is the most common radiotracer used in PET/CT imaging. The activity detection comes from multiple collisions of a positron in the radioactive material with surrounding electrons in the biological environment until it loses its kinetic energy and combines with an electron to form a short-lived positronium molecule. The positronium eventually annihilates, converting all its mass into two gamma-ray photons, 511 KeV each, that travel 180 degrees in the opposite direction. If both annihilation photons are detected within a short time interval, it is called a coincidence event and assumed to have originated from positronium annihilation somewhere along the line drawn between the two points. This obviates the need for a physical lead collimator and results in much better sensitivity than SPECT imaging, as no extrinsic collimation is required.[9]
For Gallium imaging, the conjugated version of octreotide is bound via 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA) molecule ligand to Gallium 68 radiotracer, which then effectively binds with somatostatin receptors (SSTR) expressed by well-differentiated neuroendocrine tumors. The more aggressive, poorly differentiated tumors may not show uptake on Gallium PET and can sometimes be better evaluated with FDG-PET due to less expression of SSTR and increased glucose metabolism.[10]
Indications
Evidence-based indications for the use of FDG-PET/CT for gastrointestinal tumors in the United Kingdom, as published by the UK Royal College of Radiologists in 2016, include the following:
For esophageal and gastroesophageal cancers, PET/CT is indicated for staging/ restaging if radical treatment is suitable, including for patients who have received neoadjuvant treatment. PET/CT is also indicated for evaluating suspected recurrence when other imaging is negative or equivocal. Further proposed indications include PET/CT in response assessment and radiotherapy planning.
For colorectal cancers, imaging with PET/CT is indicated for the staging of patients with synchronous metastases at presentation, for example, pulmonary and liver lesions. Further indications include restaging patients with recurrence, assessing treatment response, detecting recurrence with rising tumor markers, and/or clinical suspicion of recurrence with normal or equivocal findings on other imaging. Post-treatment, the evaluation of indeterminate presacral masses can also be done with PET/CT.
PET/CT is performed in anal cancer to stage selected patients for radical treatment. Further proposed indications include radiotherapy planning and response assessment.
For neuroendocrine tumors, FDG-PET/CT is indicated for the staging/restaging selected poorly differentiated tumors with normal or negative MIBG and octreotide scans. 68Ga-DOTA-NOC PET/CT is indicated in the staging of well-differentiated NETs (grade 1 and 2), detecting unknown primary, and evaluating recurrence.
Contraindications
Imaging with PET/CT requires careful patient preparation. Poor glycaemic control, incomplete fasting, and insulin injection just before the scan can affect the biodistribution of radiotracer as glucose in the blood can compete with FDG on the GLUT-1 transporters, and a high level of insulin can divert a substantial amount of FDG to the skeletal muscles and adipose tissue through insulin-dependent GLUT-4 transporters.
Ideally, PET/CT should not be performed until at least >6 weeks after radiotherapy or surgery and >2 weeks after stent placement to avoid inflammatory uptake at the intervention site, potentially overestimating the disease.[11]
Patients with claustrophobia may require sedation. PET/CT is generally unsuitable for pregnant patients, and alternate means of evaluating disease should be arranged.
Breastfeeding mothers should avoid contact with the infant after the scan, and the general recommendation is to bottle feed the infant by a third person for up to 12 hours after the scan.[12][13]
Equipment
The radiopharmaceutical is prepared in cyclotrons and brought into the department in lead-lined containers early in the morning. The handling process requires exquisite care and diligence to avoid exposure to the staff and public. The radiotracer is injected through a tungsten syringe employed in a specialized carrier and is kept behind a lead screen.[14]
The PET/CT system comprises stand-alone PET and CT scanners housed in a single gantry. The patient bed is shared between the two scanners and moves smoothly from the PET to the CT component during image acquisition.
A scintillator absorbs ionizing radiation and converts the fraction of absorbed energy into photons of visible or ultraviolet light which can then be converted into electric signals through photodetectors. The typical PET scanner consists of thousands of inorganic scintillation crystals organized in blocks to form detector modules arranged in a ring configuration. The bismuth germanate (BGO) detectors have been traditionally used as scintillation crystals but are now replaced by lutetium oxyorthosilicate (LSO) detectors.[15]
These crystals absorb the energy from annihilation events in the body (511 Kev energy) and create tens of thousands of visible wavelength photons proportional to the amount of energy deposited by the annihilation photon. Random coincidence is when two detected photons have come from two separate annihilation events. Scatter coincidence is when both photons are from the same event, but one or both have scattered. True coincidence is the detection of both photons from the same annihilation event.[16]
These light photons are channeled to the coupled photodetectors. The most common photodetectors in PET are photomultiplier tubes (PMTs), which consist of vacuum tubes with photocathodes.[17] The light photons interact with the cathode to produce electrons which are then amplified to produce an electric signal proportional to the energy deposited by the PET photons.
The initially formed image is not perfect in any sense and is significantly affected by the attenuation of PET photons in the body, the variation in detector efficiency, and the recording of scattering and random events with true coincidences. Therefore, attenuation correction is carried by a CT scan performed simultaneously. The CT component also helps provide additional anatomical information lacking in nascent PET images.
The images are then represented quantitatively in terms of the radioactivity concentration, i.e., kBq/ml, which is then converted into a standardized uptake value (SUV) by normalizing to the patient weight and injected radioactivity.[18] This SUV measurement can quantify glucose metabolism from a particular tissue of the body.
- SUV (g/ml) = tracer uptake(kBq/ml) / (activity (MBq) / weight (kg))
Preparation
The patient preparation for FDG-PET is complex as FDG is a glucose analog and will be taken up by all the tissues that physiologically transport glucose. PET imaging provides functional assessment at the cellular level; therefore, it is prone to artifacts caused by the physiological increase in cellular activity. Control of the glycaemic level and avoidance of activity of the non-target areas of the body are vital to maximizing diagnostic yield.
- Glycaemic control: Patients are required to fast for 4 to 6 hours prior to the scan to reduce competition between glucose and deoxyglucose at the level of GLUT-1 transporters. The insulin spike from eating can also divert glucose/ FDG to peripheral muscles through insulin-dependent GLUT-4 receptors. In diabetic patients, imaging is preferred in the early morning to make use of overnight fasting. For the above-described reasons, the insulin injection should not be given before the scan. The blood glucose level is checked before the scan to ensure that it is below 200mg/dl.[19]
- Muscular activity: As part of routine preparation, patients must avoid exercise the day before and on the day of the procedure. Patients should stay relaxed at the time of scanning and avoid swallowing and speaking during the scan to prevent radiotracer uptake in the muscles of phonation.
- Brown fat uptake: The brown fat, due to its ability to produce non-shivering thermogenesis, can take up FDG in the cold environment and thus can give false-positive PET interpretation. Therefore, it is essential to provide the patient with a warm ambiance to keep brown fat activity in control.
- Hydration: Patients should be well hydrated to increase renal excretion of FDG and are further instructed to empty the bladder just before the scan to minimize activity in the pelvic area from the full bladder. The patients are directed to drink water after the scan to facilitate the excretion of radioactive material from the body. Caffeinated drinks are not recommended.[13]
- Cannulation: The procedure is explained to the patients, and any questions are answered to minimize anxiety. Patients are then seated in a lead-lined room and preferentially cannulated with a butterfly infusion set to avoid radiation exposure to the staff members.
- The vaccine status and injection sites are recorded to avoid false-positive pitfalls as local inflammation at the injection site can produce FDG avid reactive change in the draining lymph nodes, most commonly seen in the axilla with arm vaccines.[20]
Technique or Treatment
The recommended intravenous dose of F18 FDG for adults is 370-740 MBq and for children is 4 to 5 MBq/kg.[21] After injection, the patient is seated comfortably in a warm environment for one hour to allow FDG distribution in the body. Any radiotracer extravasation is recorded, and the patient is advised to empty the bladder just before scanning.
Imaging is generally performed without oral or IV contrast. The patients are routinely advised to drink water which can act as a negative contrast agent for GIT.
Once the patient is on the scanner bed, the image acquisition starts with a topogram to plan the scanning area. For GI cancers, the imaging is mostly performed from the base of the skull to the mid-thigh. The next step is the non-breath-hold CT scan. The patient bed then moves to the PET component of the scanner to complete the combined imaging. The first set of data comprises non-attenuation correction imaging, which then undergoes attenuation correction using CT scan images.[11] The attenuation-corrected (AC) PET data can produce MIP images or be fused with CT images to provide anatomical and functional assessment in all three dimensions.
The interpretation of PET/CT images is largely carried out through maximum standard uptake value (SUV max) measurements. This is a semiquantitative assessment that is partly affected by the general metabolic status of the individual. Therefore, the background mediastinal blood pool and hepatic SUV max are recorded as a reference.
There is no single SUV value that can reliably differentiate benign from malignant process.[22] As a general rule, the metabolic activity can be categorised into 4 levels:
- Low uptake= SUV max < 2.5
- Intermediate uptake= SUV max 2.5 to 5
- High uptake = SUV max > 5
- Intense uptake = SUV max > 10
Complications
PET/CT is a safe procedure. The radiation dose from a routine diagnostic F-18 FDG at 350 MBq is 6-7 mSv. The CT component of the study is a reasonably low dose ranging from 2 to 4 mSV If used only for attenuation correction to 3-10 mSV if used for both attenuation correction and localization. These values are lower than the contrast-enhanced diagnostic CT scan with a dose of 15 to 25 mSV.[23]
It is imperative to be aware of various false negative and false positive findings that can cause misinterpretation. Some of the examples are as follows:
False-positive PET CT
Respiration or patient movement can mismatch the CT and PET data in the fused images and lead to misinterpretation. This is especially problematic in abdominal imaging, where bowel movement can give the false impression of peritoneal disease due to misregistration of physiological bowel activity outside the bowel lumen. This can be prevented by looking at the non-attenuation correction (NAC) imaging in a tricky situation.
The brown fat uptake in cold ambiance, particularly in the supraclavicular regions, can be misinterpreted as lymph nodes. Correlation of all areas of uptake with CT images is helpful to differentiate solid lesions from low Hounsfield unit fatty tissue.
Radiotracer extravasation and post-vaccination status can produce reactive lymph node uptake in the ipsilateral axilla. Such events should be documented in the patient questionnaire to be reference ready at reporting.
Inflammatory uptake at the site of radiotherapy, surgery, or biopsy can produce false-positive interpretation; therefore, the timing of scan post-intervention is crucial to differentiate malignant disease from inflammation. Chemotherapy can cause reactive marrow hyperplasia with diffuse increased radiotracer uptake in the skeleton.[24]
False-negative PET CT
The tumors with mucinous components might not show an affinity for FGD due to low cellularity, lack of GLUT-1 transporters, and poor glucose metabolism.[25] Well-differentiated NET may not show high FDG uptake; therefore, Gallium PET is instead used for their assessment.
The artifacts from metallic and vascular stents and high activity from the distended urinary bladder can mask the adjacent small tumors. Similarly, metformin causes diffusely increased bowel activity, complicating the assessment of colon pathologies.[26] (Figure 1)
Clinical Significance
Esophageal Cancer
Following histological confirmation of malignancy, esophageal cancer is staged through TNM classification. While early tumors can undergo surgical resection with or without neoadjuvant therapy, chemoradiotherapy followed by surgery is the standard of care for locally advanced esophageal cancers.[27]
Esophageal cancers generally produce focal or segmental areas of increased FDG uptake compared to low diffuse uptake seen in esophagitis (Figure 1). The T staging of early tumors is better performed with endoscopic ultrasound (EUS) due to its ability to differentiate between esophageal wall layers. EUS can also assess the immediate peri-esophageal lymph nodes with confidence. Contrast-enhanced CT scan has a complementary role in this regard. For non-locoregional and distant lymph nodes, PET/CT is the most sensitive modality and thus has a central role in the primary staging of FDG avid esophageal tumors.
Between the two main histological subtypes of esophageal cancers, squamous cell carcinoma primarily involves the upper and mid esophagus and is strongly associated with alcohol consumption and smoking. It generally shows intense FDG uptake as opposed to adenocarcinoma, which predominates in the lower esophagus, has an association with reflux and smoking, and can show highly variable FDG uptake. The incidence of adenocarcinoma is on the rise, and it is now the commonest subtype of esophageal cancer.
The PET/CT report must include the location, length, and SUV max of the tumor; tumor length is an independent prognostic factor for overall survival.[28] The commonest sites of metastases from esophageal cancers include lungs, liver, bones, adrenal glands, and non-regional LNs. Detection of occult metastasis through PET CT, not visible on conventional imaging, can avoid futile surgeries in patients not suitable for curative resection (Figure 2). The assessment of lung metastases is challenging with PET/CT due to the size of the individual lesions, which is often below the threshold (>1 cm) for PET characterization. Secondly, the non-breath-hold CT component of the PET is suboptimal for lung nodule assessment. Due to hepatic background activity, the sensitivity of PET/CT for liver metastases is also low, and if hepatic metastasectomy is planned, then preoperative MRI is essential.
PET/CT is an excellent modality to rule out new metastases or recurrence at distant sites after curative treatment of esophageal cancers. The PET/CT sensitivity to detect disease recurrence is high (pooled sensitivity estimate around 96%), but the specificity is low (pooled specificity estimate 78%) due to post-operative inflammatory change and radiation pneumonitis, giving false-positive results.[29] PET/CT scans have a role in response assessment and radiotherapy planning, but concrete evidence for their routine use is lacking.[30]
Colonic Cancer
The colonic cancers can produce focal intermediate to high intensity eccentric or short segment radiotracer uptake, but the assessment is challenging due to background physiological colonic uptake, bowel movement with misregistration, and FDG uptake in fecal matter. Diffuse high colonic uptake is often seen with metformin intake and can mask the underlying pathology.[31]
Adenocarcinomas show variable uptake but generally have high SUV max except for the mucinous variety, which shows poor FDG avidity due to low cellularity and scarce expression of GLUT-1 transporters.
PET/CT is not routinely performed to assess primary colorectal cancers and local lymph nodes due to poor spatial resolution of the PET photon detectors and limited inherent bowel contrast.[32] The peri colonic nodes can hide by the metabolic bloom of the primary tumor.[33]
MRI is generally performed for the local staging of rectal cancer and CECT for the remaining colonic cancers. Metastatic disease is seen in 20% of colonic cancers at presentation.[34] PET/CT is indicated for assessing metastatic disease in advanced tumors, especially if their resection is contemplated. The commonest sites of metastases are the liver, lung, ovaries, and peritoneum. Traditionally, metastatic disease is managed with systemic chemotherapy, but there is increasing recognition of metastasectomy with curative intent due to evidence of improved survival (37 to 58%) in patients who undergo surgical resection, even for multiple metastases.[35][36][37]
However, if surgery is considered for liver metastases, planning an MRI of the liver is mandatory. The lung metastases require assessment with a breath-hold CT scan for accurate quantification and characterization. The peritoneal metastases on PET/CT can show focal uptake or diffuse perihepatic curvilinear uptake, often correlated with CT findings of peritoneal nodules or fat stranding. Ascites is commonly associated with peritoneal disease, which may or may not show high FDG uptake.
PET/CT has an established role in detecting disease recurrence in patients with new clinical symptoms, abnormal exam findings, rising tumor markers, or indeterminate presacral lesion on conventional imaging. The differentiation between recurrent disease and post-therapy change can be challenging on PET/CT. Generally, high-intensity focal uptake that persists several months after surgery is concerning for residual or recurrent disease. Low-intensity, ill-defined uptake after surgery is expected and related to inflammatory change.[38] PET/CT is also helpful in detecting recurrence in lymph nodes and distant organs.
There is not enough data to support the definite role of PET/CT in assessing complete responders. In assessing response to liver-directed therapies like selective internal radiation therapy (SIRT), FDG-PET can be helpful as the metabolic response can be greater than the morphological response.[39]
Anal Cancer
Anal cancers are rare and account for less than 2% of large bowel malignancies, although their incidence is increasing over the past few years in developed countries.[40] The commonest cell type is squamous cell carcinoma (>70%) which is strongly linked with infection with high-risk human papillomavirus (HPV-16).[41] Combined chemoradiotherapy is curative in the majority of the patients, but patients with recurrence or local failure after chemoradiotherapy may undergo abdominoperineal resection.
Due to the very high FDG affinity of primary anal squamous cell cancer (SCC), PET/CT is routinely indicated in the primary staging of anal cancer to rule out lymph nodal and hematogenous metastases (Figure 3). The local staging of anal cancers is generally performed with MRI. Further proposed roles of PET/CT in anal cancer management include radiotherapy planning (especially with increasing consideration of intensity-modulated radiation therapy (IMRT)), response assessment, and detection of recurrence.[42]
Gastrointestinal Neuroendocrine Tumors
Advancements in imaging techniques for detecting neuroendocrine tumors could partly be responsible for their rising incidence.
The well-differentiated neuroendocrine tumors (G1, G2) and their metastases are primarily assessed with 68Ga DOTA NOC PET/CT due to their expression of somatostatin receptors (SSTR). Contrary to popular belief, even the most well-differentiated and indolent neuroendocrine tumors can metastasize (Figure 4). FDG-PET/CT is indicated in selected patients with poorly differentiated high-grade tumors (G3) as these tumors generally lack SSTR and demonstrate up-regulation of glucose metabolism, which can be mapped through FDG-PET/CT.[43]
In some patients with metastatic neuroendocrine tumors, there can be mixed proliferation profiles at different disease sites, which often becomes apparent after receptor-targeted therapy; the gallium scan shows stable or regressive disease, but the CT component of the study shows an enlargement of some non-gallium avid areas of disease.[44] FDG-PET/CT in these patients can show increased uptake in these areas due to their aggressive metabolic profile, which differs from the gallium avid disease sites. PET/CT in this scenario can be helpful to select the site for tissue sampling for histological correlate.
The knowledge of Ga68-DOTA peptide biodistribution is crucial for the accurate interpretation of pathological uptake sites. Normal radiotracer uptake is seen in the spleen, adrenal glands, pancreas, pituitary gland, liver, kidneys, thyroid, and salivary glands. Unlike FDG-PET/CT, the uptake in background soft tissue and muscles is minimal, improving the contrast of the pathologies against the background.
Enhancing Healthcare Team Outcomes
The diagnosis and management of gastrointestinal malignancies require a multidisciplinary approach. Upper and lower GI endoscopies are generally the first lines of investigation for suspected gastrointestinal malignancy. Due to significant advancements in surgery, chemotherapy, and radiotherapy, the overall survival from these cancers is on the rise. The judicial use of FDG-PET/CT in FDG avid gastrointestinal malignancies can reduce the risk of disease recurrence by accurately mapping the disease distribution and thus influencing the treatment strategy.
It has become more important to accurately stratify the patients who can benefit from curative resection because the failure of long-term survival with complete resection is often related to the failure to detect distant metastases at the time of surgery. This capability of PET/CT in detecting distant diseases justifies its use in the primary staging of FDG avid GI cancers. However, if the primary tumor is non-avid, the imaging is not reliable for assessing distant disease as the metastases are expected to match the metabolic profile of the primary tumor.
For patients undergoing neoadjuvant therapy, PET/CT can help assess poor responders and may alter management in this group of patients, although the exact time point of imaging and response criterion for PET/CT needs to be established with robust evidence through randomized control trials.
The same phenomenon by which 68Ga-DOTA-NOC PET/CT targets somatostatin receptors expressed by well-differentiated neuroendocrine tumors is exploited for transporting personalized molecular radiotherapy (MRT) to these tumors; the procedure is called peptide receptor radionuclide therapy (PRRT). In this procedure, gallium-68 is replaced by a therapeutic radiotracer (mostly Lutetium-177). Before instituting therapy, the disease is mapped through Gallium PET or octreotide imaging to select the patient suitable for treatment; for the procedure to be effective, the majority of the tumor sites have to take up radiotracer above that of the liver. After therapy, planar imaging is performed to confirm the adequate distribution of radiotherapy in the disease sites.[45] This palliative therapy regimen is being comprehensively researched to evaluate the survival benefits in a selected group of patients.
Media
(Click Image to Enlarge)

Figure 1: FDG PET/CT in a patient with dysphagia shows diffuse increased radiotracer uptake in the oesophagus consistent with oesophagitis (Blue arrows). Note heterogeneous uptake in the colon (Green arrow) due to metformin intake. Contributed by Dr Amaila Ramzan, FRCR
(Click Image to Enlarge)
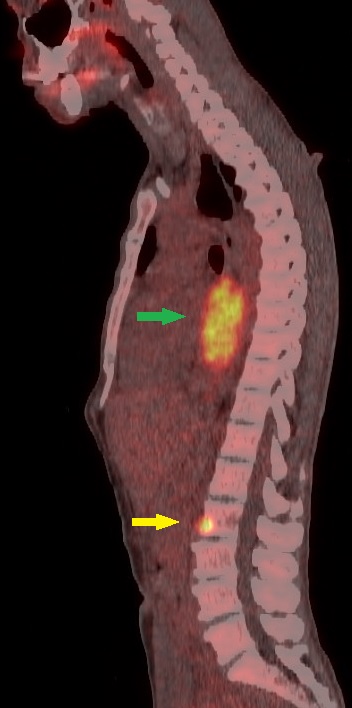
Figure 2: Sagittal fused FDG PET/CT image of a 56-year-old patient shows a highly FDG avid (SUV max 18) mass of mid-thoracic oesophagus (Green arrow) with solitary metastasis in L2 vertebral body (Yellow arrow). FDG PET/CT upstaged the disease in this patient by detecting a metastasis occult on the staging CT scan. Contributed by Dr Amaila Ramzan, FRCR
(Click Image to Enlarge)
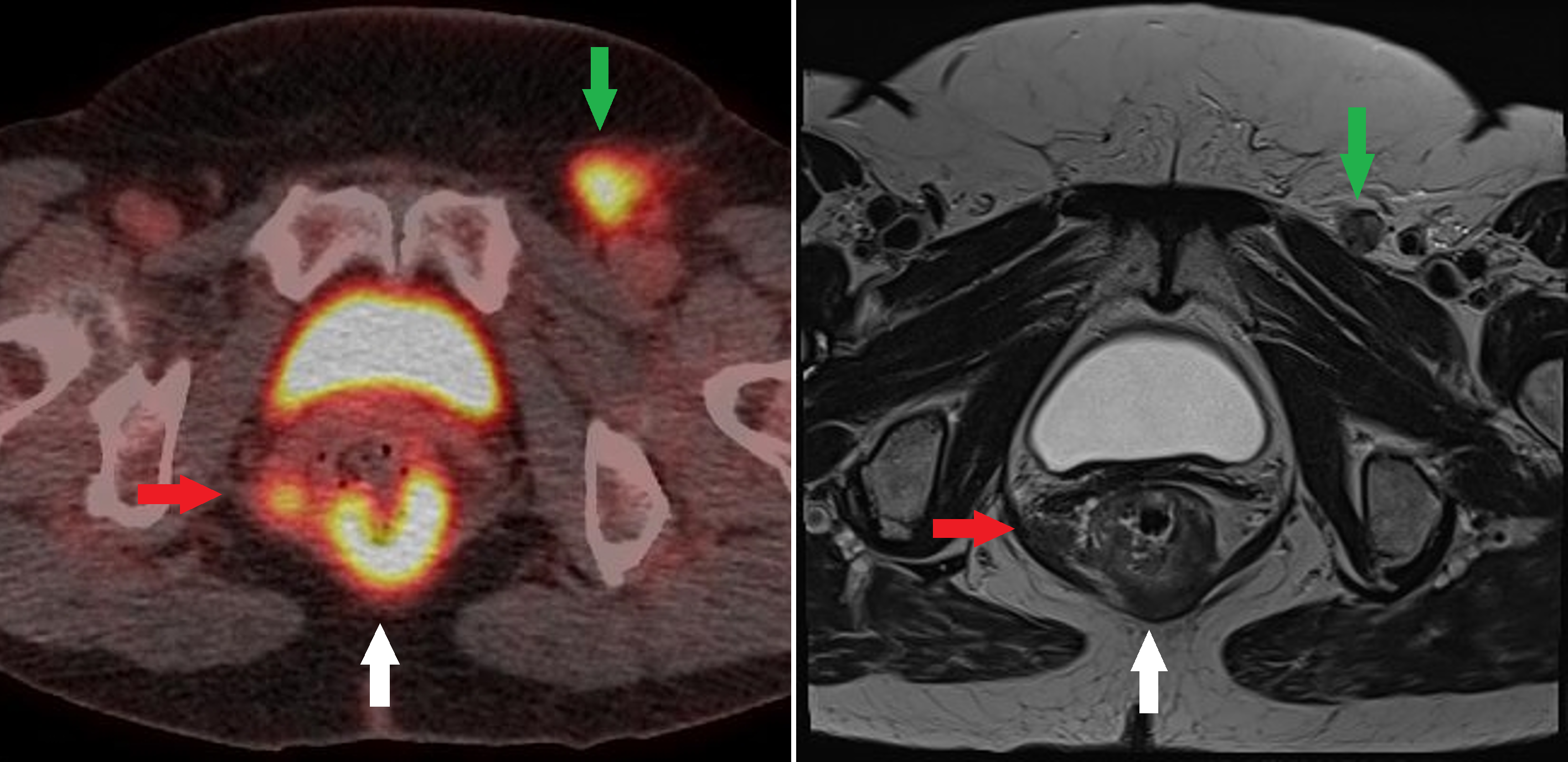
Figure 3: Fused FDG PET/CT and T2 axial MRI images at the same level of an anorectal junction tumor (White arrow) with an FDG avid nodal deposit in the right mesorectum (Red arrow) and in the left groin (Green arrow). Contributed by Dr Amaila Ramzan, FRCR
(Click Image to Enlarge)
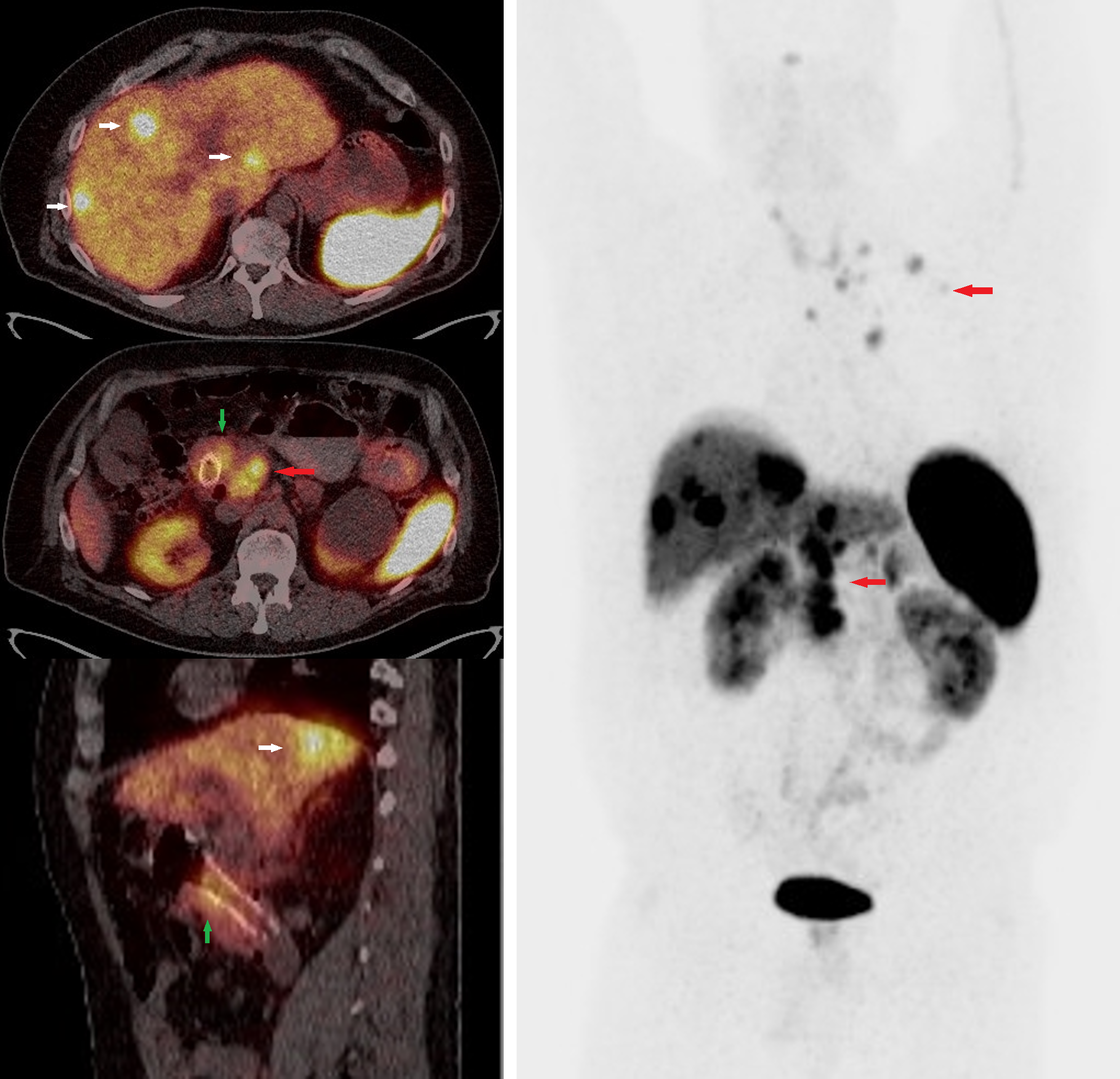
Figure 4: Ga68 DOTATOC PET/CT whole-body scan fused and MIP images of a patient with well-differentiated grade 2 neuroendocrine tumor of the duodenum with metastatic disease to the liver and lymph nodes. Green arrow: Inflammatory uptake around the stent in the duodenal tumor. Red arrows: Radiotracer uptake in conglomerate retroperitoneal and thoracic lymph nodes. White arrow: Radiotracer avid hepatic metastases. Contributed by Dr Amaila Ramzan, FRCR
References
Bentley-Hibbert S, Schwartz L. Use of Imaging for GI Cancers. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2015 Jun 1:33(16):1729-36. doi: 10.1200/JCO.2014.60.2847. Epub 2015 Apr 27 [PubMed PMID: 25918300]
Vaupel P, Schmidberger H, Mayer A. The Warburg effect: essential part of metabolic reprogramming and central contributor to cancer progression. International journal of radiation biology. 2019 Jul:95(7):912-919. doi: 10.1080/09553002.2019.1589653. Epub 2019 Mar 22 [PubMed PMID: 30822194]
Özgüven S, Filizoğlu N, Kesim S, Öksüzoğlu K, Şen F, Öneş T, İnanır S, Turoğlu HT, Erdil TY. Physiological Biodistribution of (68)Ga-DOTA-TATE in Normal Subjects. Molecular imaging and radionuclide therapy. 2021 Feb 9:30(1):39-46. doi: 10.4274/mirt.galenos.2021.37268. Epub [PubMed PMID: 33586406]
Münch S, Marr L, Feuerecker B, Dapper H, Braren R, Combs SE, Duma MN. Impact of (18)F-FDG-PET/CT on the identification of regional lymph node metastases and delineation of the primary tumor in esophageal squamous cell carcinoma patients. Strahlentherapie und Onkologie : Organ der Deutschen Rontgengesellschaft ... [et al]. 2020 Sep:196(9):787-794. doi: 10.1007/s00066-020-01630-y. Epub 2020 May 19 [PubMed PMID: 32430661]
Shepherd NA, Baxter KJ, Love SB. The prognostic importance of peritoneal involvement in colonic cancer: a prospective evaluation. Gastroenterology. 1997 Apr:112(4):1096-102 [PubMed PMID: 9097991]
Salati SA, Al Kadi A. Anal cancer - a review. International journal of health sciences. 2012 Jun:6(2):206-30 [PubMed PMID: 23580899]
Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010 Aug:39(6):707-12. doi: 10.1097/MPA.0b013e3181ec124e. Epub [PubMed PMID: 20664470]
Cives M, Strosberg JR. Gastroenteropancreatic Neuroendocrine Tumors. CA: a cancer journal for clinicians. 2018 Nov:68(6):471-487. doi: 10.3322/caac.21493. Epub 2018 Oct 8 [PubMed PMID: 30295930]
Uenomachi M, Takahashi M, Shimazoe K, Takahashi H, Kamada K, Orita T, Ogane K, Tsuji AB. Simultaneous in vivo imaging with PET and SPECT tracers using a Compton-PET hybrid camera. Scientific reports. 2021 Sep 9:11(1):17933. doi: 10.1038/s41598-021-97302-7. Epub 2021 Sep 9 [PubMed PMID: 34504184]
Karfis I, Marin G, Levillain H, Drisis S, Muteganya R, Critchi G, Taraji-Schiltz L, Guix CA, Shaza L, Elbachiri M, Mans L, Machiels G, Hendlisz A, Flamen P. Prognostic value of a three-scale grading system based on combining molecular imaging with (68)Ga-DOTATATE and (18)F-FDG PET/CT in patients with metastatic gastroenteropancreatic neuroendocrine neoplasias. Oncotarget. 2020 Feb 11:11(6):589-599. doi: 10.18632/oncotarget.27460. Epub 2020 Feb 11 [PubMed PMID: 32110279]
Long NM, Smith CS. Causes and imaging features of false positives and false negatives on F-PET/CT in oncologic imaging. Insights into imaging. 2011 Dec:2(6):679-698 [PubMed PMID: 22347986]
Hicks RJ, Binns D, Stabin MG. Pattern of uptake and excretion of (18)F-FDG in the lactating breast. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2001 Aug:42(8):1238-42 [PubMed PMID: 11483686]
Boellaard R, Delgado-Bolton R, Oyen WJ, Giammarile F, Tatsch K, Eschner W, Verzijlbergen FJ, Barrington SF, Pike LC, Weber WA, Stroobants S, Delbeke D, Donohoe KJ, Holbrook S, Graham MM, Testanera G, Hoekstra OS, Zijlstra J, Visser E, Hoekstra CJ, Pruim J, Willemsen A, Arends B, Kotzerke J, Bockisch A, Beyer T, Chiti A, Krause BJ, European Association of Nuclear Medicine (EANM). FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. European journal of nuclear medicine and molecular imaging. 2015 Feb:42(2):328-54. doi: 10.1007/s00259-014-2961-x. Epub 2014 Dec 2 [PubMed PMID: 25452219]
Level 1 (high-level) evidenceBenamor M, Ollivier L, Brisse H, Moulin-Romsee G, Servois V, Neuenschwander S. PET/CT imaging: what radiologists need to know. Cancer imaging : the official publication of the International Cancer Imaging Society. 2007 Oct 1:7 Spec No A(Special issue A):S95-9 [PubMed PMID: 17921089]
Nadig V, Herrmann K, Mottaghy FM, Schulz V. Hybrid total-body pet scanners-current status and future perspectives. European journal of nuclear medicine and molecular imaging. 2022 Jan:49(2):445-459. doi: 10.1007/s00259-021-05536-4. Epub 2021 Oct 14 [PubMed PMID: 34647154]
Level 3 (low-level) evidenceVaquero JJ, Kinahan P. Positron Emission Tomography: Current Challenges and Opportunities for Technological Advances in Clinical and Preclinical Imaging Systems. Annual review of biomedical engineering. 2015:17():385-414. doi: 10.1146/annurev-bioeng-071114-040723. Epub [PubMed PMID: 26643024]
Level 3 (low-level) evidenceKapoor V, McCook BM, Torok FS. An introduction to PET-CT imaging. Radiographics : a review publication of the Radiological Society of North America, Inc. 2004 Mar-Apr:24(2):523-43 [PubMed PMID: 15026598]
Boellaard R, O'Doherty MJ, Weber WA, Mottaghy FM, Lonsdale MN, Stroobants SG, Oyen WJ, Kotzerke J, Hoekstra OS, Pruim J, Marsden PK, Tatsch K, Hoekstra CJ, Visser EP, Arends B, Verzijlbergen FJ, Zijlstra JM, Comans EF, Lammertsma AA, Paans AM, Willemsen AT, Beyer T, Bockisch A, Schaefer-Prokop C, Delbeke D, Baum RP, Chiti A, Krause BJ. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: version 1.0. European journal of nuclear medicine and molecular imaging. 2010 Jan:37(1):181-200. doi: 10.1007/s00259-009-1297-4. Epub [PubMed PMID: 19915839]
Ozaslan E, Kiziltepe M, Addulrezzak U, Kula M, Bozkurt O, Kut E, Duran AO, Ucar M, Sakalar T, Dogan E, Topaloglu US, Inanc M, Ozkan M. Is SUVmax of (18)F-FDG PET/CT Predictive Factor for Malignancy in Gastrointestinal Tract? Nigerian journal of clinical practice. 2021 Aug:24(8):1217-1224. doi: 10.4103/njcp.njcp_637_18. Epub [PubMed PMID: 34397034]
Shirone N, Shinkai T, Yamane T, Uto F, Yoshimura H, Tamai H, Imai T, Inoue M, Kitano S, Kichikawa K, Hasegawa M. Axillary lymph node accumulation on FDG-PET/CT after influenza vaccination. Annals of nuclear medicine. 2012 Apr:26(3):248-52. doi: 10.1007/s12149-011-0568-x. Epub 2012 Jan 21 [PubMed PMID: 22271546]
Level 2 (mid-level) evidenceDelbeke D, Coleman RE, Guiberteau MJ, Brown ML, Royal HD, Siegel BA, Townsend DW, Berland LL, Parker JA, Hubner K, Stabin MG, Zubal G, Kachelriess M, Cronin V, Holbrook S. Procedure guideline for tumor imaging with 18F-FDG PET/CT 1.0. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2006 May:47(5):885-95 [PubMed PMID: 16644760]
Level 1 (high-level) evidenceKinahan PE, Fletcher JW. Positron emission tomography-computed tomography standardized uptake values in clinical practice and assessing response to therapy. Seminars in ultrasound, CT, and MR. 2010 Dec:31(6):496-505. doi: 10.1053/j.sult.2010.10.001. Epub [PubMed PMID: 21147377]
Leide-Svegborn S. Radiation exposure of patients and personnel from a PET/CT procedure with 18F-FDG. Radiation protection dosimetry. 2010 Apr-May:139(1-3):208-13. doi: 10.1093/rpd/ncq026. Epub 2010 Feb 18 [PubMed PMID: 20167792]
Griffeth LK. Use of PET/CT scanning in cancer patients: technical and practical considerations. Proceedings (Baylor University. Medical Center). 2005 Oct:18(4):321-30 [PubMed PMID: 16252023]
Berger KL, Nicholson SA, Dehdashti F, Siegel BA. FDG PET evaluation of mucinous neoplasms: correlation of FDG uptake with histopathologic features. AJR. American journal of roentgenology. 2000 Apr:174(4):1005-8 [PubMed PMID: 10749239]
Level 2 (mid-level) evidenceSteenkamp DW, McDonnell ME, Meibom S. Metformin may be associated with false-negative cancer detection in the gastrointestinal tract on PET/CT. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2014 Oct:20(10):1079-83. doi: 10.4158/EP14127.RA. Epub [PubMed PMID: 25100379]
Lordick F, Mariette C, Haustermans K, Obermannová R, Arnold D, ESMO Guidelines Committee. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of oncology : official journal of the European Society for Medical Oncology. 2016 Sep:27(suppl 5):v50-v57 [PubMed PMID: 27664261]
Level 1 (high-level) evidenceHollis AC, Quinn LM, Hodson J, Evans E, Plowright J, Begum R, Mitchell H, Hallissey MT, Whiting JL, Griffiths EA. Prognostic significance of tumor length in patients receiving esophagectomy for esophageal cancer. Journal of surgical oncology. 2017 Dec:116(8):1114-1122. doi: 10.1002/jso.24789. Epub 2017 Aug 2 [PubMed PMID: 28767142]
Goense L, van Rossum PS, Reitsma JB, Lam MG, Meijer GJ, van Vulpen M, Ruurda JP, van Hillegersberg R. Diagnostic Performance of ¹⁸F-FDG PET and PET/CT for the Detection of Recurrent Esophageal Cancer After Treatment with Curative Intent: A Systematic Review and Meta-Analysis. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2015 Jul:56(7):995-1002. doi: 10.2967/jnumed.115.155580. Epub 2015 May 7 [PubMed PMID: 25952733]
Level 1 (high-level) evidenceKitajima K, Nakajo M, Kaida H, Minamimoto R, Hirata K, Tsurusaki M, Doi H, Ueno Y, Sofue K, Tamaki Y, Yamakado K. Present and future roles of FDG-PET/CT imaging in the management of gastrointestinal cancer: an update. Nagoya journal of medical science. 2017 Nov:79(4):527-543. doi: 10.18999/nagjms.79.4.527. Epub [PubMed PMID: 29238109]
Jayaprakasam VS, Paroder V, Schöder H. Variants and Pitfalls in PET/CT Imaging of Gastrointestinal Cancers. Seminars in nuclear medicine. 2021 Sep:51(5):485-501. doi: 10.1053/j.semnuclmed.2021.04.001. Epub 2021 May 6 [PubMed PMID: 33965198]
Moses WW. Fundamental Limits of Spatial Resolution in PET. Nuclear instruments & methods in physics research. Section A, Accelerators, spectrometers, detectors and associated equipment. 2011 Aug 21:648 Supplement 1():S236-S240 [PubMed PMID: 21804677]
Dahmarde H, Parooie F, Salarzaei M. Is (18)F-FDG PET/CT an Accurate Way to Detect Lymph Node Metastasis in Colorectal Cancer: A Systematic Review and Meta-Analysis. Contrast media & molecular imaging. 2020:2020():5439378. doi: 10.1155/2020/5439378. Epub 2020 Jul 18 [PubMed PMID: 32733174]
Level 1 (high-level) evidenceRiihimäki M, Hemminki A, Sundquist J, Hemminki K. Patterns of metastasis in colon and rectal cancer. Scientific reports. 2016 Jul 15:6():29765. doi: 10.1038/srep29765. Epub 2016 Jul 15 [PubMed PMID: 27416752]
Choti MA, Sitzmann JV, Tiburi MF, Sumetchotimetha W, Rangsin R, Schulick RD, Lillemoe KD, Yeo CJ, Cameron JL. Trends in long-term survival following liver resection for hepatic colorectal metastases. Annals of surgery. 2002 Jun:235(6):759-66 [PubMed PMID: 12035031]
Level 2 (mid-level) evidenceFernandez FG, Drebin JA, Linehan DC, Dehdashti F, Siegel BA, Strasberg SM. Five-year survival after resection of hepatic metastases from colorectal cancer in patients screened by positron emission tomography with F-18 fluorodeoxyglucose (FDG-PET). Annals of surgery. 2004 Sep:240(3):438-47; discussion 447-50 [PubMed PMID: 15319715]
Saito Y, Omiya H, Kohno K, Kobayashi T, Itoi K, Teramachi M, Sasaki M, Suzuki H, Takao H, Nakade M. Pulmonary metastasectomy for 165 patients with colorectal carcinoma: A prognostic assessment. The Journal of thoracic and cardiovascular surgery. 2002 Nov:124(5):1007-13 [PubMed PMID: 12407386]
Even-Sapir E, Parag Y, Lerman H, Gutman M, Levine C, Rabau M, Figer A, Metser U. Detection of recurrence in patients with rectal cancer: PET/CT after abdominoperineal or anterior resection. Radiology. 2004 Sep:232(3):815-22 [PubMed PMID: 15273334]
Level 2 (mid-level) evidenceSzyszko T, Al-Nahhas A, Canelo R, Habib N, Jiao L, Wasan H, Pagou M, Tait P. Assessment of response to treatment of unresectable liver tumours with 90Y microspheres: value of FDG PET versus computed tomography. Nuclear medicine communications. 2007 Jan:28(1):15-20 [PubMed PMID: 17159544]
Grulich AE, Poynten IM, Machalek DA, Jin F, Templeton DJ, Hillman RJ. The epidemiology of anal cancer. Sexual health. 2012 Dec:9(6):504-8. doi: 10.1071/SH12070. Epub [PubMed PMID: 22958581]
Shiels MS, Kreimer AR, Coghill AE, Darragh TM, Devesa SS. Anal Cancer Incidence in the United States, 1977-2011: Distinct Patterns by Histology and Behavior. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2015 Oct:24(10):1548-56. doi: 10.1158/1055-9965.EPI-15-0044. Epub 2015 Jul 29 [PubMed PMID: 26224796]
Di Carlo C, di Benedetto M, Vicenzi L, Costantini S, Cucciarelli F, Fenu F, Arena E, Mariucci C, Montisci M, Panni V, Patani F, Valenti M, Palucci A, Burroni L, Mantello G. FDG-PET/CT in the Radiotherapy Treatment Planning of Locally Advanced Anal Cancer: A Monoinstitutional Experience. Frontiers in oncology. 2021:11():655322. doi: 10.3389/fonc.2021.655322. Epub 2021 Jul 1 [PubMed PMID: 34277406]
Sharma P, Singh H, Bal C, Kumar R. PET/CT imaging of neuroendocrine tumors with (68)Gallium-labeled somatostatin analogues: An overview and single institutional experience from India. Indian journal of nuclear medicine : IJNM : the official journal of the Society of Nuclear Medicine, India. 2014 Jan:29(1):2-12. doi: 10.4103/0972-3919.125760. Epub [PubMed PMID: 24591775]
Level 3 (low-level) evidenceTang LH, Untch BR, Reidy DL, O'Reilly E, Dhall D, Jih L, Basturk O, Allen PJ, Klimstra DS. Well-Differentiated Neuroendocrine Tumors with a Morphologically Apparent High-Grade Component: A Pathway Distinct from Poorly Differentiated Neuroendocrine Carcinomas. Clinical cancer research : an official journal of the American Association for Cancer Research. 2016 Feb 15:22(4):1011-7. doi: 10.1158/1078-0432.CCR-15-0548. Epub 2015 Oct 19 [PubMed PMID: 26482044]
Pobłocki J, Jasińska A, Syrenicz A, Andrysiak-Mamos E, Szczuko M. The Neuroendocrine Neoplasms of the Digestive Tract: Diagnosis, Treatment and Nutrition. Nutrients. 2020 May 15:12(5):. doi: 10.3390/nu12051437. Epub 2020 May 15 [PubMed PMID: 32429294]