
Introduction
Dental caries is a highly prevalent disease, especially among young children.[1] The care of decayed primary teeth is crucial due to their role in chewing, speaking, and functioning as natural space maintainers in the dental arch. The treatment of dental caries in the pediatric population is a long-standing issue that involves various challenges, like behavior management and the need for a perdurable treatment that lasts until tooth exfoliation.[2]
Stainless steel crowns are the most commonly used restorative option for repairing and preserving the remaining tissue of severely damaged and decayed teeth (see Image. Stainless Steel Crown). They were introduced into pediatric dentistry in 1947, first described by Engel, and then popularised by Humphrey in 1950. Stainless steel crowns have outperformed other materials, such as amalgam and composite, in terms of durability and longevity for more than a half-century. In fact, no restorative material has provided the benefits of low cost, reliability, and durability when interim full-coronal coverage is required.[3][4]
Scientific evidence favors stainless steel crowns as restoration of choice in young children with high caries risk (see Image. Dental Caries).[4] Despite its many advantages, the use of stainless steel crowns is still unpopular among some professionals that see them as difficult to use, even though they are easier to place than intracoronal restorations and have much better long-term outcomes (see Images. Stainless Steel Crown, 1-Year Follow-Up, Stainless Steel Crown, 2-Year Follow-Up).[5]
Indications
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Indications
- Following pulp therapy
- Multisurface caries restorations
- Patients at high risk of caries
- Deciduous teeth with developmental defects, such as amelogenesis imperfecta, dentinogenesis imperfecta, enamel hypoplasia
- Teeth with extensive wear
- Where it is likely that the restoration will fail, e.g., proximal box formed is extended beyond the anatomic line angles.
- Fractured teeth
- Abutment for space maintainer[6]
- Patients who are unlikely to attend follow up appointments[7]
Contraindications
Equipment
Burs and Stones
- No. 169L or No. 69L F.G [10]
- Round bur for removal of caries
- Flame shaped diamond bur or round end tapered bur
- Long thin tapered bur
Others
- Rough or whitening polish wheels
- Greenstone or heatless stone/rubber wheel stone for finishing and polishing [11]
- Wire wheel for finishing crown
- Cement medium - glass slab/cement mixing pad, spatula, cement
- Rubber dam armamentarium
- Local anesthesia
- Dental floss
- Pliers and instruments
- Sharp explorer for marking the gingival extension of the crown margin
Preparation
Before reducing the tooth surface and adapting the crown, the operator must follow the following steps:
Selection of Crown
The operator can select the crown using different methods:
- Measuring the mesiodistal dimension of the tooth before tooth preparation
- Trial and error method
- Crown selection after tooth preparation
Loss of mesiodistal dimension resulting from space loss distal to the mandibular primary first molar complicates selecting an appropriate size crown (see Image. Stainless Steel Crown in Primary First Molar). In such cases, measuring the dimension of the contralateral tooth is advised.[12] A correctly fitting crown should snap into place at try-in.[13] Other factors should be considered when selecting the crown: occlusal anatomy, primate spaces, and crown height.[6]
Occlusal Evaluation
Before placing the rubber dam and preparing the tooth, observe the following:
- Whether the opposing tooth has extruded as a consequence of long-standing carious lesions
- Whether there is mesial drift as a result of carious lesions leading to proximal space loss
- Presence of spacing and crowding
- Examine occlusion directly in the mouth or indirectly with dental analysis casts for incisor, canine, and molar relationship on both sides
- Examine for dental midline and the cusp fossa relationship bilaterally
Local Anesthesia
The tooth and adjacent soft tissues should be sufficiently anesthetized to prevent the pain and discomfort caused by tooth reduction and potential damage to the soft tissues during the stainless steel crown trial fitting. Additional anesthesia of the palatal surfaces of upper teeth is advised for few patients. Local infiltration is considered to be a better choice than topical anesthesia.[14]
When preparing a root-treated tooth, the reduction of the mesial and distal contact areas may cause trauma to the local gingival tissues; therefore, applying topical anesthesia is advisable and may be sufficient.
Rubber Dam Isolation
Using rubber dam isolation is advised for the following reasons:
- To protect adjacent tissue
- To increase visibility and efficiency
- To improve behavior management of child
- To avoid ingestion of the stainless steel crown
Wedging
Many scholars advocated for the use of wooden wedges before beginning tooth preparation. These are used to keep adjacent teeth apart and reduce the chance of iatrogenic damage to the enamel.
Removal of Caries
Caries removal and pulpotomy procedures can be performed before or after crown preparation, although most crown preparation can be done while excavating caries.[6][8][15]
Technique or Treatment
Full et al. suggested that preparing the occlusal surface first allows for better access to the proximal areas of the tooth.[16] Other authors recommended preparing the proximal slices before reducing the occlusal.[17] The best strategy is to reduce the occlusal surface first while removing caries and reducing the proximal surfaces. If proximal reduction were to be performed first, diagnosing possible pulp exposure will become difficult due to the gingival bleeding that can occur when preparing the proximal surfaces (see Image. Endodontic Obturation).
Occlusal Reduction
Operators can use 69L or 169L bur to reduce 1.5 to 2.0 mm of the occlusal surface. The cusps original contour needs to be preserved. Occlusal depth guidance grooves could be given for better reduction. If a sufficient amount of occlusal surface has already been lost due to caries, marginal ridges of neighboring teeth can be used as a reference.[18]
Proximal Reduction
Proximal surfaces are reduced using a 69 L/ tapered fissure bur at high speed to make room for the crown and establish a feather finish line gingivally while avoiding damaging neighboring teeth. The mesial and distal contact points should be cleared such that a probe could pass through them. Following the normal proximal contour, proximal slices should slightly converge toward the occlusal and lingual. A smooth taper from occlusal to gingival, free of ledges or shoulders, should be achieved.[10][6]
Buccal/Lingual Reduction
Reducing the buccal and lingual surfaces is the third step in the preparation. The reduction of the buccal and lingual mucosa is optional. Some authors suggested preparing the buccal and lingual walls to create a gingivally inclined long bevel to make crown placement easier. On the other hand, others advocated for none to minimal (0.5 to 1 mm) preparation on the vestibular and lingual aspect of the crown, unless pronounced enamel convexity should only be reduced by a small amount.[12] Duggal and Curzon recommended trying the selected crown before lingual and buccal reduction.[13]
Lastly, the operator should round all line and point angles. Occlusal-lingual and occlusal-buccal angles are beveled at 45 degrees. Bur is held parallel to the tooth’s long axis, and one should carefully blend the surfaces. Remove any remaining caries and perform appropriate pulp therapy if there is pulp involvement.
The rubber dam should be left in place until cementing the crown. If it interferes with the seating and adaptation of the crown, it can be removed after tooth preparation.[6]
Crown Adaptation
Crown adaptation is critical for retention and gum protection. A poorly adapted crown serves as a source of plaque and bacterial accumulation, resulting in gingivitis and recurrent cervical caries.
Spedding advocated two key principles to adjust a stainless steel crown correctly. The operator must determine the appropriate occlusal-gingival crown length. Crown margins should be contoured circumferentially to follow the natural contours of the marginal gingiva of the tooth.
Steps
Place the crown linguo-buccally on the prepared tooth, applying pressure in the buccal direction so that the crown slips over the buccal surface and into the gingival sulcus. There will be friction as the crown slides over the buccal bulge. Crown positioning will be difficult if the crown is too small or if the buccal bulge is too excessive. In this case, choose a larger crown or reduce the tooth's buccal bulge. After placing the selected crown over the prepared tooth, ask the patient to bite over it. Check for preliminary occlusal and marginal ridge relation. Previously, scratch a mark on the stainless steel crown at the level of the free gingival margin. Scratch or dotted lines indicate the gingival contour, as well as the portion of the crown to be removed. Remove the crown and trim or cut away the additional crown portion gingivally 1 mm below the scratch line with a crown and bridge scissors or, preferably, a large abrasive wheel (“heatless stone”) that allows for more precise reduction. Repeat the procedure until the adequate extension of 1 mm beneath the gingival margin is achieved.
Operators can use the number 137 pliers can be used for circumferential contouring. Contouring pliers deliver a belling effect in the middle third of the crown.[19] For cervical crown adaptation, Johnson contouring pliers with a No. 114 are used on the cervical third of the buccal and lingual surfaces. A curved beak plier No. 114 is then used to contour the buccal and lingual surfaces. Curved beak pliers may also be used to contour the crown's proximal areas.[20][13] Lastly, the crimping pliers are used to crimp the cervical margin 1 mm circumferentially for final adaptation and ensure that the crown margin's outline follows the gingival margin of the tooth. The operators can check the final adaptation of the crown by taking a radiograph to verify the gingival contour and extension, ensuring the complete coverage of the tooth.[13][21]
Finishing
A large green stone is used to create a knife-edge finish at the cervical margin of the crown. The bur is rotated counterclockwise at a 45-degree angle. Then a rubber wheel is used to smooth out the margins. The crown type can be smoothed and polished with a piece of cloth or chamois wheel on the dental lathe, using Tripoli polishing agent and jeweler's rouge for final finishing.[11]
Cementation
A luting cement should be used to secure the crown. Once the crown is seated on the prepared tooth, it should be kept under pressure while the cement hardens. Manufacturers recommend glass ionomer, zinc polycarboxylate, and zinc phosphate cement but, fluoride-leaching cement has additional advantages. Due to the clinical advantages, RMGIC is the preferred choice.[22] However, research suggests the type of cement used has little effect on retention, with the essential retentive components derived from proper crown contouring and crimping.
Operators must pay deliberate attention to the removal of excess cement. This is normally accomplished by running a pointed instrument around the cemented crown's margins and sliding knotted dental floss buccolingual through the contact areas after the cement setting. Excess cement has been shown to affect gingival health.[8][6]
Modifications
With Adjacent Stainless Steel Crowns
When more than one crown is required in a quadrant, both teeth should be prepared during the same visit. There should be slightly more than usual reduction on the adjacent proximal surfaces. This will make it easier to place multiple crowns. Before reducing another tooth, the occlusal reduction of one should be completed. Simultaneous reduction of both teeth results in improper reduction. If there are proximal caries on adjacent teeth, there is a risk of mesiodistal space loss. To restore carious adjacent teeth with stainless steel crowns, the preparations should be modified so that the teeth can be fitted with smaller-sized crowns than normal. Rather than more proximal reduction, further reduction of the buccal and lingual walls is carried out.[6][10][23]
Adjacent Stainless Steel Crown With Arch Length Loss/Space Loss
Reduction of the crown's mesiodistal dimension is frequently required, particularly when mesial drift (often caused by caries) has resulted in arch length loss. Flattening the crown's mesial and distal contact areas using Adam's design pliers results in a moderate reduction in the mesiodistal dimension. A contralateral upper tooth crown with a smaller size can be used if there is mesial drift in the lower arch. Another form of modification is vertical slicing and spot-welding, an additional segment of a stainless steel band. This is done to increase the perimeter or extend the length. However, the efficacy of the latter modifications remains largely untested.[8]
Before the Eruption of the Permanent Mandibular First Molar
Even if there are no adjacent teeth, operators should cautiously measure the available mesiodistal dimension, and precise proximal tooth reduction should be performed to prevent unnecessary crown margin overhang. This is particularly pertinent before the first permanent molar erupts distally to the second primary molar (see Image. Stainless Steel Crown in Primary Second Molar). If there is any encroachment in the space required for the eruption of the first permanent molar, it will lead to a distorted eruption pathway of the permanent molar.
Crown Extension for Deep Subgingival Caries
Teeth with caries extending apically to the crown margin should have these areas filled with restoration before preparing the tooth to allow an appropriate finishing line for the crown, or a stainless steel extension could be soldered to the crown to form a flange for this area.[6]
Restoration of Bruxism/Hypoplastic Teeth
Greater occlusal wear results from bruxism and hypoplastic disease, causing decreased vertical height. In this case, occlusion can be improved by adding a solder layer from the crown's impression surface to prevent or reduce occlusal reduction (Croll's technique). The rest of the tooth preparation and crown adaptation is standard.[24]
Open-faced Stainless Steel Crown
Stainless steel crowns can be rendered more aesthetically pleasing in anterior teeth by trimming the labial surface of the crown and making it open facing. A composite resin is then placed into the crown's labial face after fitting. Aesthetic crowns with prefabricated tooth-colored buccal and occlusal facings are also available from specialized suppliers.[8]
Modification of Stainless Steel Crown Sizes
Undersized Crown
The crown wall of the best-fitting crown can be cut buccally or lingually, and an additional piece of 0.004-inch orthodontic stainless steel band can be welded over the gap that is then contoured to the desired form.
Oversized Crown
To minimize the crown diameter, the metal edges of the best-sized crown can be given a V cut on the buccal surface. The cut edges are then reapproximated. The overlapping margins are then welded together.[6]
Hall Technique
In 2006, Dr. Norna Hall introduced a quick and non-invasive procedure to arrest caries: the crown is placed without local anesthesia, without tooth preparation, and without caries elimination. The main aim of this procedure was to increase the compliance of an anxious child and the operator's comfort.
The biological principle behind the Hall technique is to arrest caries by leaving and isolating the more superficial layer of biofilm and carious lesion from the oral cavity; therefore, the composition of the biofilm will be substituted to a less cariogenic microflora, arresting the caries progression.[25]
The concerns regarding the Hall technique: use of orthodontic appliances that are time-consuming; premature contacts and increased occlusal vertical dimension as a result of lack of tooth preparation, although they are corrected at the follow-up appointment after one year; aesthetically unappealing.[25]
Indications
- Children with class 1 caries with non-cavitated lesions that are unable to accept fissure sealant, partial removal of caries, or conventional restoration
- Children with class 2 caries with cavitated or non-cavitated lesions that are unable to accept fissure sealant, partial removal of caries, or conventional restoration with no signs of pulpal involvement
- Sufficient sound tissue to retain the crown
Contraindications
- Patients with severe caries with signs and symptoms of irreversible pulpitis or dental sepsis.
- Crown severely destroyed due to caries that is non-restorable
- Children at risk of bacterial endocarditis
Procedure
- Place orthodontic separators between the contact point of the primary molar for 4 or 5 days to create room for the crown.
- Select the smallest-sized crown covering all the cusps, approaching the contact points, and giving a 'spring back' effect.
- Adjustments of the crown are to be made using band-forming pliers if necessary.
- Cementation of the crown with glass ionomer cement. The tooth must be maintained in occlusion until the cement sets, followed by excess removal using floss.[25][26]
The Hall technique should be chosen as an alternative when the traditional approach with crown preparation is implausible.[25]
Complications
Interproximal Ledge
Wrongly positioning the bur can result in a ledge instead of the desired shoulder-free interproximal cutting. If the operator fails to remove the ledge, the crown seating will be impeded.[6]
Marginal Discrepancy
Several researchers have extensively demonstrated the association between gingivitis and marginal defects, such as impaired marginal adaptation and insufficient removal of excess cement. Careful adaptation of the margins before fitting is required, and post-fitting gingivitis can be minimized by diligently polishing the crown margin. A preventive regimen, including oral hygiene training, should be included in the treatment plan.[8][27]
Inhalation or Ingestion of Crown
A rubber dam is to be placed till cementation to prevent aspiration of the crown. Sometimes to prepare the distal surface, the rubber dam may be removed prior. Even after all the measures taken, accidents do happen. Clinicians and their staff must remain calm to make timely decisions to avoid potentially dangerous complications and ultimately save their patients' lives. The dentist's responsibility is to be alert to both early and delayed signs and symptoms of an aspiration accident and respond quickly if and when it occurs. High vacuum suctioning, patting on the back after placing the patient in the prone position, Heimlich maneuver should be tried to yield the crown. A clinical referral for a rapid chest radiograph should be made if still not successful in retrieving the crown. If the crown remains in the lung or bronchi, it can be removed via bronchoscopy. Immediate medical and surgical intervention would be required.[28]
Clinical Significance
Primary teeth are relatively at a larger risk of caries than permanent teeth. They also have larger pulp with prominent pulp horns placing exacting demands on cavity design. Hence a full-coverage restoration is required. Although stainless steel crowns have an aesthetic disadvantage, they are still the treatment of choice for the following reasons:
- Durability
- Efficiency
- Longevity
- Cost-effectiveness
- Reliability
Even though other tooth-colored restorations are available in the market, they are either costly or require more tooth reduction, thereby increasing the chances of pulp exposure.[15][29]
Enhancing Healthcare Team Outcomes
Dental caries is the most frequent oral disease of children worldwide, with a prevalence of 1% to 12% in developed countries and up to 70% in underdeveloped nations.[25] The management of caries in primary dentition is challenging and complex due to the need for behavior management measures and perdurable treatments that last until tooth exfoliation - both issues being solved by utilizing stainless steel crowns (see Image. Primary Dentition). Despite this, studies show that pediatric dentists are more likely to restore carious deciduous dentition using stainless steel crowns than general dentists (see Image. Stainless Steel Crown of 46).[30] A higher level of training in this treatment at the undergraduate level and access to postgraduate courses are required to increase the use of these effective appliances by general dentists.[30]
Media
(Click Image to Enlarge)

Stainless Steel Crown. This is a postoperative photo of a stainless steel crown in 46.
Contributed by D Amlani, BDS
(Click Image to Enlarge)

Dental Caries. This is a preoperative photo of 46 showing dental caries.
Contributed by D Amlani, BDS
(Click Image to Enlarge)
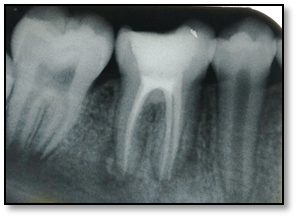
Endodontic Obturation. This is a periapical radiograph showing the endodontic obturation of 46.
Contributed by D Amlani, BDS
(Click Image to Enlarge)

Stainless Steel Crown of 46.
Contributed by D Amlani, BDS
(Click Image to Enlarge)

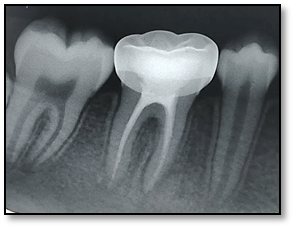
Stainless Steel Crown, 1-Year Follow-Up. This radiograph shows a stainless steel crown of 46 at a 1-year follow-up.
Contributed by D Amlani, BDS
(Click Image to Enlarge)
Stainless Steel Crown, 2-Month Follow-Up. This radiograph shows a stainless steel crown of 46 at a two-month follow-up.
Contributed by D Amlani, BDS
(Click Image to Enlarge)

Primary Dentition. This image shows stainless steel crowns in primary dentition.
Contributed by P Daruich, BDS
(Click Image to Enlarge)

Stainless Steel Crown in Primary First Molar.
Contributed by P Daruich, BDS
(Click Image to Enlarge)

Stainless Steel Crown in Primary Second Molar.
Contributed by P Daruich, BDS
References
Kopczynski K, Meyer BD. Examining Parental Treatment Decisions Within a Contemporary Pediatric Dentistry Private Practice. Patient preference and adherence. 2021:15():645-652. doi: 10.2147/PPA.S300684. Epub 2021 Mar 25 [PubMed PMID: 33790544]
Kaptan A,Korkmaz E, Evaluation of success of stainless steel crowns placed using the hall technique in children with high caries risk: A randomized clinical trial. Nigerian journal of clinical practice. 2021 Mar; [PubMed PMID: 33723119]
Level 1 (high-level) evidenceMathew MG, Roopa KB, Soni AJ, Khan MM, Kauser A. Evaluation of Clinical Success, Parental and Child Satisfaction of Stainless Steel Crowns and Zirconia Crowns in Primary Molars. Journal of family medicine and primary care. 2020 Mar:9(3):1418-1423. doi: 10.4103/jfmpc.jfmpc_1006_19. Epub 2020 Mar 26 [PubMed PMID: 32509626]
Seale NS, The use of stainless steel crowns. Pediatric dentistry. 2002 Sep-Oct; [PubMed PMID: 12412965]
Uhlen MM,Tseveenjav B,Wuollet E,Furuholm J,Ansteinsson V,Mulic A,Valen H, Stainless-steel crowns in children: Norwegian and Finnish dentists' knowledge, practice and challenges. BMC oral health. 2021 Apr 12; [PubMed PMID: 33845821]
Randall RC. Preformed metal crowns for primary and permanent molar teeth: review of the literature. Pediatric dentistry. 2002 Sep-Oct:24(5):489-500 [PubMed PMID: 12412964]
Pinkham JR. Intraprofessional controversies: reflections on the stainless steel crown situation. ASDC journal of dentistry for children. 2001 Sep-Dec:68(5-6):292-3 [PubMed PMID: 11985187]
Level 3 (low-level) evidenceKindelan SA, Day P, Nichol R, Willmott N, Fayle SA, British Society of Paediatric Dentistry. UK National Clinical Guidelines in Paediatric Dentistry: stainless steel preformed crowns for primary molars. International journal of paediatric dentistry. 2008 Nov:18 Suppl 1():20-8. doi: 10.1111/j.1365-263X.2008.00935.x. Epub [PubMed PMID: 18808544]
Duggal MS,Curzon ME, Restoration of the broken down primary molar: 2. Stainless steel crowns. Dental update. 1989 Mar; [PubMed PMID: 2599249]
Nash DA, The nickel-chromium crown for restoring posterior primary teeth. Journal of the American Dental Association (1939). 1981 Jan; [PubMed PMID: 7019286]
Croll TP,Epstein DW,Castaldi CR, Marginal adaptation of stainless steel crowns. Pediatric dentistry. 2003 May-Jun; [PubMed PMID: 12889701]
Ramazani N, Ranjbar M. Effect of tooth preparation on microleakage of stainless steel crowns placed on primary mandibular first molars with reduced mesiodistal dimension. Journal of dentistry (Tehran, Iran). 2015 Jan:12(1):18-24 [PubMed PMID: 26005450]
Afshar H, Ghandehari M, Soleimani B. Comparison of Marginal Circumference of Two Different Pre-Crimped Stainless Steel Crowns for Primary Molars After Re-Crimping. Journal of dentistry (Tehran, Iran). 2015 Dec:12(12):926-31 [PubMed PMID: 27559353]
Padminee K, Hemalatha R, Shankar P, Senthil D, Trophimus GJ. Topical anesthesia for stainless steel crown tooth preparation in primary molars: a pilot study. Journal of dental anesthesia and pain medicine. 2020 Aug:20(4):241-250. doi: 10.17245/jdapm.2020.20.4.241. Epub 2020 Aug 27 [PubMed PMID: 32934990]
Level 3 (low-level) evidenceInnes NP,Ricketts D,Chong LY,Keightley AJ,Lamont T,Santamaria RM, Preformed crowns for decayed primary molar teeth. The Cochrane database of systematic reviews. 2015 Dec 31; [PubMed PMID: 26718872]
Level 1 (high-level) evidenceFull CA, Walker JD, Pinkham JR. Stainless steel crowns for deciduous molars. Journal of the American Dental Association (1939). 1974 Aug:89(2):360-4 [PubMed PMID: 4527221]
Mink JR, Bennett IC. The stainless steel crown. The Journal of the Ontario Dental Association. 1968 Oct:45(10):420-30 [PubMed PMID: 5247599]
Society of Pediatric Dentistry. [Guideline on operation of stainless steel crown for decidous teeth restoration]. Zhonghua kou qiang yi xue za zhi = Zhonghua kouqiang yixue zazhi = Chinese journal of stomatology. 2020 Aug 9:55(8):551-554. doi: 10.3760/cma.j.cn112144-20200514-00270. Epub [PubMed PMID: 32842346]
Level 2 (mid-level) evidenceAyedun OS,Oredugba FA,Sote EO, Comparison of the treatment outcomes of the conventional stainless steel crown restorations and the hall technique in the treatment of carious primary molars. Nigerian journal of clinical practice. 2021 Apr; [PubMed PMID: 33851682]
Mulder R, Medhat R, Mohamed N. In vitro analysis of the marginal adaptation and discrepancy of stainless steel crowns. Acta biomaterialia odontologica Scandinavica. 2018:4(1):20-29. doi: 10.1080/23337931.2018.1444995. Epub 2018 Feb 28 [PubMed PMID: 29536024]
Guelmann M, Gehring DF, Turner C. Retention of veneered stainless steel crowns on replicated typodont primary incisors: an in vitro study. Pediatric dentistry. 2003 May-Jun:25(3):275-8 [PubMed PMID: 12889706]
Virupaxi S, Pai R, Mandroli P. Retentive strength of luting cements for stainless steel crowns: A systematic review. Journal of the Indian Society of Pedodontics and Preventive Dentistry. 2020 Jan-Mar:38(1):2-7. doi: 10.4103/JISPPD.JISPPD_313_19. Epub [PubMed PMID: 32174622]
Level 1 (high-level) evidenceMink JR,Hill CJ, Modification of the stainless steel crown for primary teeth. ASDC journal of dentistry for children. 1971 May-Jun; [PubMed PMID: 4934143]
Croll TP. Increasing occlusal surface thickness of stainless steel crowns: a clinical technique. Pediatric dentistry. 1980 Dec:2(4):297-9 [PubMed PMID: 7017102]
Altoukhi DH, El-Housseiny AA. Hall Technique for Carious Primary Molars: A Review of the Literature. Dentistry journal. 2020 Jan 17:8(1):. doi: 10.3390/dj8010011. Epub 2020 Jan 17 [PubMed PMID: 31963463]
Ludwig KH, Fontana M, Vinson LA, Platt JA, Dean JA. The success of stainless steel crowns placed with the Hall technique: a retrospective study. Journal of the American Dental Association (1939). 2014 Dec:145(12):1248-53. doi: 10.14219/jada.2014.89. Epub [PubMed PMID: 25429038]
Level 2 (mid-level) evidenceSharaf AA,Farsi NM, A clinical and radiographic evaluation of stainless steel crowns for primary molars. Journal of dentistry. 2004 Jan; [PubMed PMID: 14659715]
Level 2 (mid-level) evidenceAdewumi A, Kays DW. Stainless steel crown aspiration during sedation in pediatric dentistry. Pediatric dentistry. 2008 Jan-Feb:30(1):59-62 [PubMed PMID: 18402101]
Level 3 (low-level) evidenceClark L, Wells MH, Harris EF, Lou J. Comparison of Amount of Primary Tooth Reduction Required for Anterior and Posterior Zirconia and Stainless Steel Crowns. Pediatric dentistry. 2016 Jan-Feb:38(1):42-6 [PubMed PMID: 26892214]
Shelton A, Yepes JF, Vinson LA, Jones JE, Tang Q, Eckert GJ, Downey T, Maupome G. Utilization of Stainless Steel Crowns by Pediatric and General Dentists. Pediatric dentistry. 2019 Mar 15:41(2):127-131 [PubMed PMID: 30992110]