Introduction
Greater trochanteric pain syndrome (GTPS) groups several etiologies of lateral hip, buttock, and thigh pain. These etiologies include greater trochanteric bursitis, gluteal medius tendinopathy or tears, gluteal minimus tendinopathy or tears, and iliotibial band snapping.[1][2] Furthermore, patients may have coexisting bursitis and tendinopathy.
Greater trochanteric bursitis is characterized by localized lateral hip pain that typically presents with focal tenderness over the greater trochanter. The pain typically worsens when walking upstairs, standing up from a chair, or lying with the affected side down.[3][4] The most common physical examination finding of greater trochanteric bursitis is pain with palpation over the greater trochanter; this is the key clinical diagnostic indicator differentiating greater trochanteric bursitis from primary diseases of the hip joint, which typically radiate towards the groin. The pain of greater trochanteric bursitis may be exacerbated by active abduction and passive adduction of the hip.[5][6]
GTPS is more common in females, patients who are overweight or obese, and patients aged 40 to 60 years. It has been suggested that the larger width of the typical female pelvis may cause increased tension on the iliotibial band over the greater trochanter. In addition, patients with GTPS may have coexisting back pain, hip osteoarthritis, and conditions that alter lower extremity mechanics, such as knee pain resulting in abnormal forces around the hip.[1] GTPS is diagnosed clinically and does not have specific diagnostic criteria. Imaging results are variable and may show bursitis, gluteal tendinopathy, or no bursal inflammation.[7][8]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The greater trochanter is located at the neck of the femur and is characterized by its lateral quadrangular projection. The greater trochanter is the primary attachment site for the strong tendons facilitating hip abduction. The muscles of hip abduction are the tensor fascia latae, gluteus medius, and gluteus minimus muscles.[9] There are 4 lateral hip muscles divided into superficial and deep layers. The superficial layer comprises the gluteus maximus and tensor fasciae latae, and the deep layer comprises the gluteus medius and gluteus minimus. The fascia lata is laminar fibrous tissue that starts at the greater trochanter and functions as a site of insertion for the gluteus maximus and tensor fascia latae. The iliotibial band (ITB) is a thickened portion of the fascia lata; the ITB and tensor fascia latae function as a lateral band to reduce strain over the greater trochanter.[1]
The greater trochanter has four facets: anterior, lateral, posterosuperior, and posterior. The anterior facet is the site of insertion for the gluteus minimus tendon; the lateral facet is the site of insertion for the gluteus medius anterior tendon; the posterosuperior facet is the site of insertion for the gluteus medius posterior tendon.[9]
Several bursae around the greater trochanter cofacilitate abduction with the abductor tendons; these include the subgluteus maximus, subgluteus medius, and subgluteus minimus bursae. Colloquially, the "trochanteric bursa" refers to the subgluteus maximus bursa located lateral to the greater trochanter between the gluteus maximus and gluteus medius muscles and deep to the ITB and fascia lata.[9]
The superior gluteal nerve (L5 and S1) innervates the gluteus medius and gluteus minimus muscles.
Trochanteric bursitis may be caused by gluteal muscle overuse or injury, obesity, leg length discrepancy, direct trauma, or inflammation due to tendinopathy or tear of the gluteus medius or gluteus minimus muscles.[10][4][11] The mechanism of injury is microtrauma of the gluteal tendons at their insertion into the greater trochanter. This microtrauma increases friction between the greater trochanter and iliotibial band, resulting in GTPS. The anterior fibers of the gluteal tendons experience the most force and are often the first to tear.[7]
Indications
Injection of the trochanteric bursa is a treatment option for patients diagnosed with greater trochanteric bursitis. It should be considered for patients who fail conservative management.[8] However, interventional treatment should not be delayed, given the disability caused by this painful syndrome.
Contraindications
Absolute contraindications to bursal injections include patient refusal, active systemic infection, cellulitis over the injection site, and significant immunocompromise. The injection-associated risk of hemarthrosis is low, and anticoagulation medications may be continued without changes. Coagulation studies are not required. However, patients with a recently documented supratherapeutic International Normalized Ratio (INR) should reschedule the procedure until after the INR has returned to therapeutic levels.[4]
Equipment
The following equipment is required or recommended to perform a trochanteric bursal injection.
- 18 G needle for aspirating medications
- 25 G hypodermic needle for skin and subcutaneous infiltration with local anesthetic
- 22- to 25-gauge, 3.5-inch spinal needle
- 1% lidocaine for skin and subcutaneous tissue infiltration
- Local anesthetic (0.25% bupivacaine is long-acting, alternative agents may be used)
- Steroid (40 mg/mL triamcinolone is long-acting, alternative agents may be used)
- Imaging suite with access to C-arm fluoroscopy (optional)
- Contrast agent (240 mg/mL iohexol) if using fluoroscopy
- Ultrasound (optional)
Personnel
Trochanteric bursal injections are typically performed by advanced practice providers or physicians trained in primary care, pain medicine, anesthesiology, physical medicine and rehabilitation, interventional radiology, or orthopedic surgery.[8][9] In addition, a skilled staff member is usually present to help facilitate the procedure; a fluoroscopy technician is required if imaging guidance is used.
Preparation
This procedure is typically performed in an outpatient setting. Before the procedure, written informed consent should be obtained after the risks, benefits, and alternatives have been discussed with the patient.
The site of treatment should be marked. The skin should be prepped using an aseptic technique and draped in a sterile manner. Before the start of the procedure, a “time out” should be performed to verify patient identity, procedure, allergies, relevant laboratory results, and correct treatment site.[4]
Technique or Treatment
Injections of the trochanteric bursa can be performed without image guidance based on anatomic landmarks or under ultrasound or fluoroscopic guidance. Ultrasound guidance provides a reliable and safe modality to identify tendons and bursae, which may improve injection accuracy compared to a landmark-based method. In addition, it allows visualization of the needle tip and spread of the injectate.[9] Fluoroscopic guidance should be considered in patients where palpation of the greater trochanter is challenging to minimize the risk of intra-tendinous injection and in patients where the landmark-based injection was unsuccessful in providing pain relief.[1]
Position the patient supine with the hip in a neutral position. Identify the greater trochanter by palpating the lateral aspect of the hip for a bony prominence. Place a needle on the skin at the entry site and confirm placement fluoroscopically. Administer local anesthesia to the dermis and subcutaneous tissue by injecting 1 % lidocaine with a 25-gauge hypodermic needle. Afterward, advance a 25-gauge 3.5-inch spinal needle toward the lateral margin of the greater trochanter until osseous tissue is encountered. Intermittently capture fluoroscopic images while advancing the spinal needle towards the greater trochanter to confirm the needle trajectory and locate the needle tip. Remove the stylet once the spinal needle is at the greater trochanter. After negative aspiration, administer 1 to 2 mL of iodinated contrast to confirm the location. After fluoroscopic confirmation with contrast dye, inject a combination of steroids and 1 to 3 mL of local anesthetic. Remove the spinal needle, cleanse the skin with alcohol, and apply a clean dressing.[4][1]
The intrabursal local anesthetic typically provides immediate but temporary pain relief; bupivacaine can provide up to 4 to 6 hours of pain relief. The onset of pain relief from corticosteroids usually begins between 2 and 5 days postinjection, with the peak effect occurring between 10 and 14 days. Most patients experience the greatest pain relief after approximately six weeks.[7] Steroid injections can relieve pain for 3 to 6 months, but individual responses may vary. Steroid injections may be repeated but are limited to 3 or 4 injections per year due to the increased risk of side effects from cumulative steroid administration.[4] Patients may experience exquisite pain during the procedure when the bursa is contacted and should be counseled appropriately.
Complications
In general, injecting the trochanteric bursa is considered safe, and the risk of serious adverse effects is low.[12][7] The most common risks to discuss with patients are pain, bleeding, infection, allergic reactions, and injury to adjacent structures.
Infection should be considered in the setting of persistent, localized pain associated with erythema or purulent discharge at the injection site, fevers, chills, and other systemic infectious indicators.[4] The overall risk of septic arthritis is less than 0.3 %.[4] Necrotizing fasciitis following injection of the trochanteric bursa is exceedingly rare but has been reported.[12]
Common side effects of steroid injection include headache, flushing, insomnia, and elevated blood glucose.[4] Long-term injectable corticosteroid treatment can weaken tendon structures and increase the risk of steroid-induced tendon rupture.[7][4] Steroid flares can mimic septic arthritis and may present as severe localized pain with an increased systemic inflammatory response and a joint effusion. Flares usually present 1 to 3 days following the procedure and last up to 5 days. The steroid flare does not impact the efficacy of the injection and should be treated conservatively with nonsteroidal anti-inflammatory agents (NSAIDs).[4] A corticosteroid injection can cause fat cells at the injection site to atrophy. A depression in the skin may appear because the underlying fat cells have deteriorated.
Clinical Significance
Greater trochanteric bursitis is a self-limiting condition that may cause significant pain and functional impairment. Although conservative management with NSAIDs, activity modification, physical therapy, and weight reduction is often successful, corticosteroid injections are commonly performed to reduce pain and improve functionality.[13]
Utilizing fluoroscopy or ultrasound may help direct needle placement and confirm intrabursal injection. However, there is little evidence that imaging modalities improve clinical outcomes.[1][14] A multicenter randomized trial comparing landmark-based and fluoroscopy-guided corticosteroid injections demonstrated no significant difference in pain scores at rest and with activity one month after injection.[8]
A study comparing the accuracy of landmark-based injections against ultrasound-guided injections in cadavers demonstrated that ultrasound-guided injections had higher accuracy concerning injection into the greater trochanter bursa.[9] Image-guided injections should be considered for patients who failed to get pain relief with a landmark-based injection or those with imaging demonstrating bursal inflammation.[15][10][8]
Enhancing Healthcare Team Outcomes
Injections of the trochanteric bursa are commonly performed to treat pain secondary to greater trochanteric bursitis. The interprofessional approach is critical to maintaining patient safety and optimizing procedure performance.
Communication is essential as each healthcare team member plays a role in facilitating patient care. The nurse should bring in the equipment and medications and place appropriate monitors for vital signs. The imaging technician should know the treatment site to position the fluoroscopy machine appropriately. Any questions or concerns about the medications administered during the procedure should be directed toward a pharmacist. After the procedure, the patient should be monitored for any immediate adverse effects or complications.
The patient should be instructed that pain relief after the procedure will likely be temporary due to the transient effect of the local anesthetic and that it will take several days for the corticosteroids to take effect. In addition, the patient should be educated on common issues after the procedure, such as local site tenderness and any signs or symptoms that warrant medical attention. The patient should also be advised to avoid prolonged submersion in water for 24 hours.[4]
The clinician who performed the procedure should be available to answer any questions or concerns before patient discharge. An interprofessional approach provides the best patient outcomes.
Media
(Click Image to Enlarge)
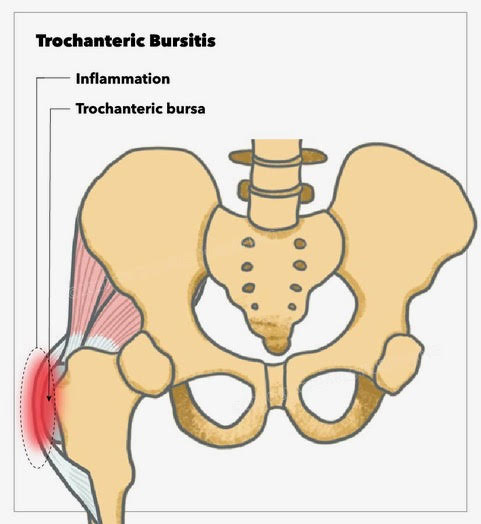
Trochanteric Bursitis Contributed by Emma Gregory, Illustrator StatPearls Publishing
(Click Image to Enlarge)
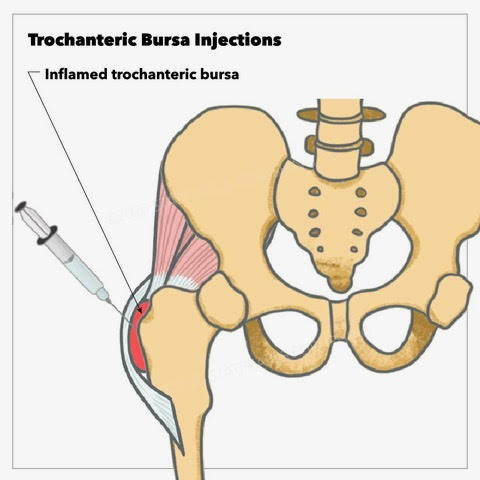
Trochanteric Bursitis Injection Contributed by Emma Gregory, Illustrator StatPearls Publishing
References
Mao LJ, Crudup JB, Quirk CR, Patrie JT, Nacey NC. Impact of fluoroscopic injection location on immediate and delayed pain relief in patients with greater trochanteric pain syndrome. Skeletal radiology. 2020 Oct:49(10):1547-1554. doi: 10.1007/s00256-020-03451-7. Epub 2020 May 2 [PubMed PMID: 32361853]
Redmond JM, Chen AW, Domb BG. Greater Trochanteric Pain Syndrome. The Journal of the American Academy of Orthopaedic Surgeons. 2016 Apr:24(4):231-40. doi: 10.5435/JAAOS-D-14-00406. Epub [PubMed PMID: 26990713]
Wilson SA, Shanahan EM, Smith MD. Greater trochanteric pain syndrome: does imaging-identified pathology influence the outcome of interventions? International journal of rheumatic diseases. 2014 Jul:17(6):621-7. doi: 10.1111/1756-185X.12250. Epub 2013 Dec 6 [PubMed PMID: 24314334]
Level 2 (mid-level) evidenceRaythatha M, Spitz D, Tang JY. Fluoroscopically-guided Joint and Bursa Injection Techniques: A Comprehensive Primer. Seminars in roentgenology. 2019 Apr:54(2):124-148. doi: 10.1053/j.ro.2018.09.002. Epub 2018 Sep 21 [PubMed PMID: 31128737]
Lustenberger DP, Ng VY, Best TM, Ellis TJ. Efficacy of treatment of trochanteric bursitis: a systematic review. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine. 2011 Sep:21(5):447-53. doi: 10.1097/JSM.0b013e318221299c. Epub [PubMed PMID: 21814140]
Level 1 (high-level) evidenceKaiser K, Fitzgerald M, Fleshman B, Roberts K. Large and Intermediate Joint Injections: Olecranon Bursa, Greater Trochanteric Bursa, Medial and Lateral Epicondyle Peritendinous Injections. Primary care. 2022 Mar:49(1):119-130. doi: 10.1016/j.pop.2021.10.005. Epub 2022 Jan 5 [PubMed PMID: 35125152]
Reid D. The management of greater trochanteric pain syndrome: A systematic literature review. Journal of orthopaedics. 2016 Mar:13(1):15-28. doi: 10.1016/j.jor.2015.12.006. Epub 2016 Jan 22 [PubMed PMID: 26955229]
Level 1 (high-level) evidenceCohen SP, Strassels SA, Foster L, Marvel J, Williams K, Crooks M, Gross A, Kurihara C, Nguyen C, Williams N. Comparison of fluoroscopically guided and blind corticosteroid injections for greater trochanteric pain syndrome: multicentre randomised controlled trial. BMJ (Clinical research ed.). 2009 Apr 14:338():b1088. doi: 10.1136/bmj.b1088. Epub 2009 Apr 14 [PubMed PMID: 19366755]
Level 1 (high-level) evidenceMu A, Peng P, Agur A. Landmark-Guided and Ultrasound-Guided Approaches for Trochanteric Bursa Injection: A Cadaveric Study. Anesthesia and analgesia. 2017 Mar:124(3):966-971. doi: 10.1213/ANE.0000000000001864. Epub [PubMed PMID: 28079582]
Bolton WS, Kidanu D, Dube B, Grainger AJ, Rowbotham E, Robinson P. Do ultrasound guided trochanteric bursa injections of corticosteroid for greater trochanteric pain syndrome provide sustained benefit and are imaging features associated with treatment response? Clinical radiology. 2018 May:73(5):505.e9-505.e15. doi: 10.1016/j.crad.2017.11.020. Epub 2017 Dec 19 [PubMed PMID: 29273226]
Seidman AJ, Taqi M, Varacallo M. Trochanteric Bursitis. StatPearls. 2023 Jan:(): [PubMed PMID: 30860738]
Cheng J, Abdi S. COMPLICATIONS OF JOINT, TENDON, AND MUSCLE INJECTIONS. Techniques in regional anesthesia & pain management. 2007 Jul:11(3):141-147 [PubMed PMID: 18591992]
Wang Y, Wang K, Qin Y, Wang S, Tan B, Jia L, Jia G, Niu L. The effect of corticosteroid injection in the treatment of greater trochanter pain syndrome: a systematic review and meta-analysis of randomized controlled trials. Journal of orthopaedic surgery and research. 2022 May 21:17(1):283. doi: 10.1186/s13018-022-03175-5. Epub 2022 May 21 [PubMed PMID: 35598025]
Level 1 (high-level) evidenceCushman DM, Christiansen J, Kirk M, Clements ND, Cunningham S, Teramoto M, McCormick ZL. Image guidance used for large joint and bursa injections; a survey study. The Physician and sportsmedicine. 2020 May:48(2):208-214. doi: 10.1080/00913847.2019.1674122. Epub 2019 Oct 3 [PubMed PMID: 31560251]
Level 3 (low-level) evidenceCohen SP, Narvaez JC, Lebovits AH, Stojanovic MP. Corticosteroid injections for trochanteric bursitis: is fluoroscopy necessary? A pilot study. British journal of anaesthesia. 2005 Jan:94(1):100-6 [PubMed PMID: 15516348]
Level 3 (low-level) evidence