Introduction
Indocyanine green angiography (ICGA) is used to image the choroidal circulation and its abnormalities.[1] Even though fundus fluorescein angiography (FFA) is a good tool for imaging retinal circulation in great detail, its ability to image the choroidal circulation is limited by the poor transmission of fluorescence through retinal pigment epithelium (RPE), media opacities, and retinal exudates.[2] The physical characteristics of indocyanine green (ICG) allow its visualization through RPE, lipid exudates, and serosanguineous fluid. Indocyanine green has an absorption peak at 790 to 805 nm and a peak emission spectrum at 835 nm.[3]
As its absorption and emission spectrum is of a higher wavelength than that of fluorescein, the infrared rays to and from ICG can penetrate better through the RPE, macular xanthophyll pigments, and media opacities. Also, 98% of ICG in serum is protein-bound, allowing only limited diffusion through the fenestrations of the choriocapillaris, whereas FA diffuses quickly, blurring the anatomy of the choroid.[4][5]
ICG was approved for human use by Food and Drug Administration (FDA), the USA, in 1956.[6] ICG angiography (ICGA) of the human choroid was first performed by R W Flower in 1972.[7] Initially, the clarity of images was poor as the ICG molecule has poor fluorescence efficiency compared to FA. But, technological advances in imaging systems (scanning laser ophthalmoscope or SL- based systems) led to the development of high-resolution cameras that could capture ICGA images with great clarity. In the era of anti-vascular endothelial growth factor (anti-VEGF) agents and optical coherence tomography (OCT), the monitoring of the choroidal neovascular membrane (CNVM) has become easier.[8][9]
Still, ICGA continues to be an important imaging modality in clinical practice in evaluating various disorders, including idiopathic polypoidal choroidal vasculopathy (IPCV), retinal angiomatous proliferation (RAP), central serous chorioretinopathy (CSCR), ocular inflammatory conditions including sympathetic ophthalmia (SO) and Vogt Koyanagi Harada syndrome (VKH); and ocular tumors.[10][11]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The blood supply of the choroid is from the ophthalmic artery, the first branch of the internal carotid artery.[12] The medial and lateral posterior ciliary arteries (PCAs) arise from the ophthalmic artery, which continues as long PCAs after giving 10 to 20 short PCAs. The short PCAs pierce the sclera near the optic nerve and supply the choroid, whereas the two long ciliary arteries pierce the sclera further away from the optic nerve and run in the suprachoroidal space anteriorly. The short PCAs supply the posterior part of the choroid extending from the posterior pole to the equator. The long PCAs supply whole of the choroid anterior to the equator and a small portion posterior to the equator. The PCAs behave as end arteries and do not anastomose with each other. This leads to the formation of the choroidal watershed zones.[13]
The innermost layer of the choroid is Bruch membrane. The Bruch membrane is composed of five sublayers- the basement membrane of retinal pigment epithelium, the inner collagenous layer, the middle elastic layer, the outer collagenous layer, and the basement membrane of choriocapillaris. Outside the Bruch membrane, there are three vascular layers- the inner choriocapillaris composed of a highly anastomosed capillary network, the middle Sattler layer formed by medium-sized arterioles, and the outer layer of larger arterioles, the Haller layer.[14] The choriocapillaris lobule is the functional unit of choroidal circulation that is functionally independent.[15]
The functional lobules are more evident during the filling and draining phases of the fluorescein angiogram.[16] A terminal choroidal arteriole supplies each choriocapillaris lobule. There is no anastomosis with the adjacent choriocapillaris lobule. The blood from the choroidal circulation is drained through the vortex veins. The venous system also has segmental distribution. There is no anastomosis between the veins draining to each vortex vein.[17]
The blood supply to the choroid is probably the highest among any tissue in the human body per unit of tissue weight. It is ten times higher than that of the brain. This extremely high blood flow helps maintain higher oxygen tension in the choroid than in the retina. This helps in the diffusion of oxygen from the choroid to the retina. The choroidal circulation is the major supply of oxygen to the retina. During the dark, when the photoreceptors are highly metabolically active, up to 90% of the blood supply to the retina is from the choroidal circulation. The walls of the choriocapillaris are fenestrated, which allows high permeability of glucose and other small molecules.[18]
But larger proteins are not permeable through the fenestrations. ICG is 98% protein-bound making it largely impermeable through the choriocapillaris wall.[4] On the contrary, fluorescein is only 80% protein bound.[19] So it readily diffuses out of the choriocapillaris.[20]
Indications
The indications of ICGA include:
- Exudative age-related macular degeneration (wet AMD)[21]
- Idiopathic polypoidal choroidal vasculopathy (IPCV or PCV)[22]
- Retinal angiomatous proliferation (RAP)[23]
- Central serous chorioretinopathy (CSCR)[10]
- Retinal arterial macroaneurysm (RAM)[24]
- Choroidal tumors
- Choroidal melanoma
- Choroidal hemangioma
- White Dot Syndromes[25]
- Birdshot chorioretinopathy (BSCR)
- Multifocal choroiditis
- Multiple evanescent white dot syndrome (MEWDS)
- Serpiginous choroidopathy
- Acute posterior multifocal placoid pigment epitheliopathy (APMPPE)
- Punctate inner chorioretinopathy (PIC)
- Acute zonal occult outer retinopathy (AZOOR)
- Chorioretinal atrophy
- Ocular inflammatory diseases
ICG is also used to determine liver function, hepatic blood flow, and cardiac output. ICGA has been used intraoperatively during the surgical management of intracranial aneurysms.[28][29]
Contraindications
ICG is a relatively safe and well-tolerated dye. It has only a few contraindications in ophthalmological use. In patients who are allergic to iodide or shellfish, ICGA should not be performed. Also, it is contraindicated in patients with uremia and those with a history of severe hypersensitivity.[30]
ICG is exclusively eliminated through the liver. So in patients with liver disease, ICGA is not recommended.[31] According to FDA classification, ICG is a pregnancy category C drug. That means there are no adequate studies on humans to establish safety.[32] The aqueous solution of ICG has to be used within 6 hours. An interval of at least one week is necessary after ICGA for radioactive iodine uptake studies.
Equipment
A fundus camera with excitation and a barrier filter is used for taking photographs. There are two categories of fundus cameras used for ICGA, digital flash cameras and confocal scanning laser ophthalmoscopes (SLOs). In a digital flash camera (including FF 450 plus by Zeiss and TRC-50DX by Topcon), the light source is white light. Its excitation filter transmits rays of wavelength between 640 and 780 nm and barrier filter between 820 and 900 nm. In SLOs (including Spectralis by Heidelberg, Mirante by Nidek, and California by Optos), laser monochromatic light is used for excitation. The Spectralis uses a diode laser (790 nm) for excitation.[33] A barrier filter of 830 nm is used in Spectralis. Dynamic ICGA is possible in the SLO system as it can capture 12 to 15 images per second.[34]
The standard intravenous dose of ICG for an adult individual is 25 mg in 5 ml solvent.[35] A 23 gauge scalp vein needle set, a 5 ml syringe with a needle, alcohol swab, tourniquet, and armrest are also required. A standard emergency kit for the management of anaphylaxis should always be kept ready before starting the procedure.
Personnel
The team of health care workers for carrying out ICGA includes an ophthalmologist, technician, optometrist, a nursing staff, and an anesthetist.
Preparation
Informed consent should be taken from the patient before starting the procedure. The risks and benefits of the procedure should be explained to the patient. A thorough history of the allergies and systemic comorbidities of the patient should be taken—two to four hours of fasting before the procedure are recommended. The adult dose of ICG is 25 mg in 5 ml of solvent. If SLO systems are used, 25 mg of ICG is dissolved in 3 ml of solvent, and only 1 ml of solution is injected. A 5 ml saline flush should be given immediately after injecting the dye.
It should be made sure that pupils are well dilated before starting the procedure. The emergency kit should be available. A few color fundus images should be taken to check for clarity and focus. The patient should be comfortably seated, and the arm should be placed on the armrest. The chin should be kept on the chinrest. The patient should understand that the images will be taken first in the primary gaze and later in different gazes. The scalp vein set is inserted into a vein in the ventral aspect of the forearm. It is important to ensure that the needle is inside the vein by drawing some blood or flushing with saline.
Technique or Treatment
After placing the patient's chin on the chin rest, the assistant holds the head of the patient to prevent head movements while capturing images. The moment dye is injected, control photographs are taken, which automatically switches on the timer. Pictures are taken at an interval of 1.5 to 2 seconds. After the choroidal arterial and venous system is filled with the dye, photographs are taken at a slower pace. Pictures of the fellow eye also have to be taken.
Normal ICGA Phases
- Early phase - The early phase has three stages:
- Stage 1: Begins 2 seconds after the injection of the dye. It is marked by rapid filling of choroidal arteries and choriocapillaris and early filling of choroidal veins. The choroidal watershed zone and the retinal vasculature remain dark in this stage.
- Stage 2: Three to five seconds after ICG injection, larger choroidal veins, and retinal arterioles fill the dye.
- Stage 3: (6 seconds to 3 minutes) - The choroidal watershed zone gets filled with the dye, and larger choroidal veins and choroidal arteries begin to fade.
- The middle phase (3 to 15 minutes) is characterized by fading of the retinal and choroidal vessels.
- Late phase (15 to 60 minutes) - Staining of the extrachoroidal tissue is noted. It gives an illusion that choroidal vasculature is hypofluorescent compared to the background tissue. Retinal vessels are not visualized during this phase.[3]
Complications
[36]Adverse effects of ICGA are less common compared to FA. Extravasation of the dye can cause a stinging sensation. Mild side effects like nausea and vomiting are seen in 0.15% of patients. Moderate adverse events like urticaria, vasovagal events are seen in 0.2% of patients. Urticaria can be treated using antihistamines. The incidence of severe adverse events is 0.05%. Anaphylaxis can occur in patients with iodine allergies. The incidence of adverse events is more common in patients with uremia compared to the general population.[37]
Clinical Significance
Exudative Age-Related Macular Degeneration (exudative AMD or wet AMD)
ICGA helps to delineate the extent of occult CNVM. Occult CNVM comprises 60-85% of CNV in wet AMD.[38][39] In ICGA, three morphologic variants of CNVM have been described: hot spot or focal spot, plaque (poorly defined or well defined), and mixed or combined (both hot spot and plaque are present).[35]
The combined type of CNVM may have a hot spot or multiple hot spots at the edge of the plaque (marginal hot spots), hot spots over the plaque (overlying hot spots), or hot spots away from the plaque (remote spots). In eyes with occult CNVM, a majority (around 60%) of eyes reveal plaques on ICGA, and approximately 30% of eyes show hot spots. The rest of the eyes have combined lesions. The visual prognosis of plaque may be worse compared to hot spots, and hot spots may be treated easily with PDT.[40]
ICGA helps determine the presence of CNVM in a retinal pigment epithelial detachment (PED). In a PED without CNVM (non-vascularized PED), hypocyanescence is noted throughout the phases of ICGA. In eyes with proven occult CNVM with serous PED (vascularized PED) on FFA, 62% showed plaque (size more than one disc area), 38% of eyes showed focal CNVM (with a maximum size of one optic disc area), and in 4% of eyes ICGA could not detect a CNVM.[41] Vascularized PEDs may show a notch at the margin, which may suggest the area of CNVM on FFA as described by Gass.[42]
Advantages of ICGA include the ability to visualize CNVM or other causes of subretinal or submacular hemorrhage. The causes of submacular hemorrhage, as revealed by ICGA in a study on 51 eyes, included wet AMD (around 53%), PCV (about 37%), retinal arterial macroaneurysm (about 6%), and lacquer cracks.[43] ICGA is usually not used to study classic CNVM on FFA as it may not provide clinically relevant additional information.
Clear lesion delineation is crucial in treatment modalities like photodynamic therapy (PDT) and laser photocoagulation. Anti-VEGF therapy causes regression of only immature vessels. It does not affect mature vessels.[44] ICGA helps in differentiating immature and mature vessels. This may be of great help, especially in non-regressed CNVMs after multiple anti-VEGF injections.
Retinal angiomatous proliferation (RAP) or Type 3 CNVM
RAP may contribute to up to 20% of cases of wet AMD. ICGA also aids in differentiating occult CNVM from retinal angiomatous proliferation (RAP). The feeding retinal arteriole and the draining retinal venule in RAP can be visualized in ICGA.[45] Typical features of RAP include intraretinal hemorrhage, retino-retinal anastomosis visible in the early phase of ICGA, high-flow vascular alterations, retino-choroidal anastomosis, and double retinal and choroidal circulation.[46][47]
Cystoid macular edema and PED may be associated.[48] RAP is associated with a poor functional prognosis unless treated at an early stage.[49] Also, the treatment response of RAP is better with combined anti-VEGF and photodynamic therapy compared to anti-VEGF alone.[50][51]
Polypoidal Choroidal vasculopathy (PCV)
ICGA is highly recommended for identifying PCV lesions, and ICGA is considered the gold standard for diagnosing PCV.[35][52] ICGA should be advised to rule out PCV in the eyes with:
- Massive spontaneous subretinal or submacular hemorrhage
- Orange-red subretinal nodule
- Notched or hemorrhagic PED, and
- Poor response to anti-VEGF therapy.[52]
PCV is an abnormality of choroidal circulation in which a vascular network is formed in the inner choroidal layers with an aneurysmal bulge usually at the margin of such network. The aneurysmal bulge is clinically visible as a reddish-orange polyp-like structure.[53]
In ICGA, even though the PCV network starts getting filled with the dye earlier than the retinal vessels, it gets filled slowly. Later the polyps become visible as hypercyanescent lesions. The EVEREST study on PCV used the following criteria to diagnose PCV: early focal subretinal hypercyanescence appearing within 6 minutes of ICG administration with at least one of the following:
- associated branching vascular network,
- pulsatile polyp,
- nodular appearance on stereoscopic view,
- hypocyanescent halo around polyp within 6 minutes,
- orange subretinal nodule on stereoscopic color fundus photo that corresponds to the polyp on ICGA, and
- massive submacular hemorrhage (minimum size of 4 disc area).[54]
It is important to differentiate PCV from CNVM as PCV responds better with photodynamic therapy (PDT) or a combination of PDT and intravitreal anti-VEGF therapy rather than anti-VEGF therapy alone.[54][55] Peripheral exudative hemorrhagic chorioretinopathy (PEHCR) has been divided into two groups: with and without peripheral PCV. The peripheral PCV subtype shows polyps on ICGA in eyes with PEHCR.[56]
Central Serous Chorioretinopathy (CSCR)
ICGA of CSCR is characterized by multifocal areas of choroidal hyperpermeability in the mid and late phases.[57] These areas of hyperpermeability may surround the area of leak seen on FFA, in the unaffected retina, or in the fellow eye. The early phase shows a delay in the choroidal filling. The late phase of ICGA may show persistent hypercyanescence or washout. Chronic CSCR is characterized by multifocal areas of inner choroidal hyperpermeability. Identifying these areas of leaks helps in the treatment of chronic CSCR using PDT.[58]
ICGA also helps to differentiate CSCR from PCV and helps detect underlying CNVM in CSCR.[59] Other ICGA features of CSCR include presumed occult serous PEDs,[60] delayed arterial filling of choroid and choriocapillaris, punctate hypercyanescent spots,[61] with choriocapillaris and venous congestion.[36]
ICGA forms an important investigation for the recently described pachychoroid disease spectrum, including CSCR, PCV, pachychoroid pigment epitheliopathy (PPE), pachychoroid neovasculopathy (PNV), focal choroidal excavation,[62] and peripapillary pachychoroid syndrome (PPS).[63]
Retinal Arterial Macroaneurysm (RAM)
Retinal arterial macroaneurysm can present with pre-retinal, intraretinal, and subretinal hemorrhage. In case of significant pre-retinal hemorrhage, FA may not visualize the macroaneurysm due to the masking effect of the hemorrhage. But ICGA can visualize the macroaneurysm as the infrared rays can penetrate better through the hemorrhage.[64]
Choroidal Tumors
Choroidal melanoma - ICGA is superior to FA in identifying the tumor vasculature and borders. The tumor microcirculation patterns in ICGA, such as parallel with cross-linking, loops, arcs with branching, and networks, are associated with a higher rate of tumor growth.[65]
Choroidal hemangioma - In circumscribed choroidal hemangioma, the intrinsic vascular pattern is seen 30 seconds after injection of ICG. The lesions become intensely hypercyanescent at 1 minute. In the late phases of the angiogram, the dye washes out from the lesion rapidly compared to the background choroid making the hemangioma appear hypocyanescent.[66]
White Dot Syndromes
Birdshot chorioretinopathy - In ICGA, hypocyanescent dots correspond to the cream-colored lesions in birdshot chorioretinopathy. ICGA is superior to FA in this disease as these lesions are not usually visualized in FA.[67]
Multifocal Choroiditis - The white lesions in multifocal choroiditis are visualized as hypocyanescent dots in ICGA. ICGA can be used to monitor the treatment response as the number and size of these hypocyanescent areas decrease with successful treatment with systemic steroids.[68]
Multiple evanescent white dot syndrome (MEWDS) - MEWDS presents with unilateral diminution of vision. It is common in young females. It has a transient and self-limiting course. ICGA reveals multiple hypocyanescent spots in the mid and late phases. These spots are more apparent in ICGA compared to FA.[69]
Serpiginous choroidopathy - In serpiginous choroidopathy, ICGA reveals choroidal alterations even if there is no clinical or FA evidence. In ICGA, the active lesions appear to be larger compared to FA. Thus it helps in the identification of active lesions. Also, choroidal activity can be present even after the cessation of retinal activity. This can be identified using ICGA.[70]
Acute posterior multifocal placoid pigment epitheliopathy (APMPPE) - In acute APMPPE, ICGA reveals hypocyanescent lesions in both the early and late phases of the angiogram. This is hypothesized to be due to choroidal hypoperfusion secondary to occlusive vasculitis.[71]
Punctate inner chorioretinopathy (PIC) - Hypocyanescent spots are noted in all phases of ICGA, which may be more in number than is visible on fundus photo or FFA.[72][73]
Acute zonal occult outer retinopathy (AZOOR) - Fundus autofluorescence shows very typical features. ICGA may be normal or may show hypocyanescence. In late-stage AZOOR, a trizonal pattern may be noted. The area outside the lesion shows normal cyanescence (zone 1). The margin shows late extrachoroidal leakage (minimal) (zone 2). Zone 3 or the area inside the lesson shows hypocyanescence due to choriocapillaris atrophy.[74]
Chorioretinal Atrophy
In Stargardt disease, there is a complete loss of choriocapillaris ('dark atrophy' or complete absence of choriocapillaris on ICGA) whereas, in geographical atrophy secondary to age-related macular degeneration (ARMD), residual choriocapillaris are present. ICGA aids in differentiating between late-onset Stargardt disease from chorioretinal atrophy. Hypocyanescence is seen in the late phases of ICGA in the case of Stargardt disease.[75] In dry AMD with geographic atrophy, the areas of atrophy become isocyanescent in the late phase of ICGA.
Ocular inflammatory Diseases
Sympathetic Ophthalmia: ICGA shows hypocyanescent patches, some of which may become isocyanescent in the late phase.[76]
Vogt Koyanagi Harada (VKH) syndrome: The ICGA features in the acute phase include early hypercyanescence and leakage from choroidal stromal vessels, hypocyanescent spots, fuzzy large choroidal vessels, and hypercyanescence of the optic disc.[77] The hypocyanescent spots resolve with adequate therapy. The persistence of such ICGA lesions despite therapy may denote the presence of subclinical inflammation that may lead to sunset glow fundus and suggest the need to increase the immunosuppression in such cases.[77] ICGA may be used to detect subclinical recurrence of VKH syndrome.[78]
Enhancing Healthcare Team Outcomes
The team of the ophthalmologist and the assisting nurse takes consent and counsels the patient before the procedure. Pushing the ICG dye while the ophthalmologist or the technician is capturing the images, monitoring the patient for any adverse reactions during the procedure is also carried out by the nursing staff. Anesthetists or critical care specialists are required in cases of severe allergy and anaphylactic reaction. An interprofessional team approach helps to prevent and manage complications. It helps in carrying out ICG angiography with minimal risk.
Media
(Click Image to Enlarge)
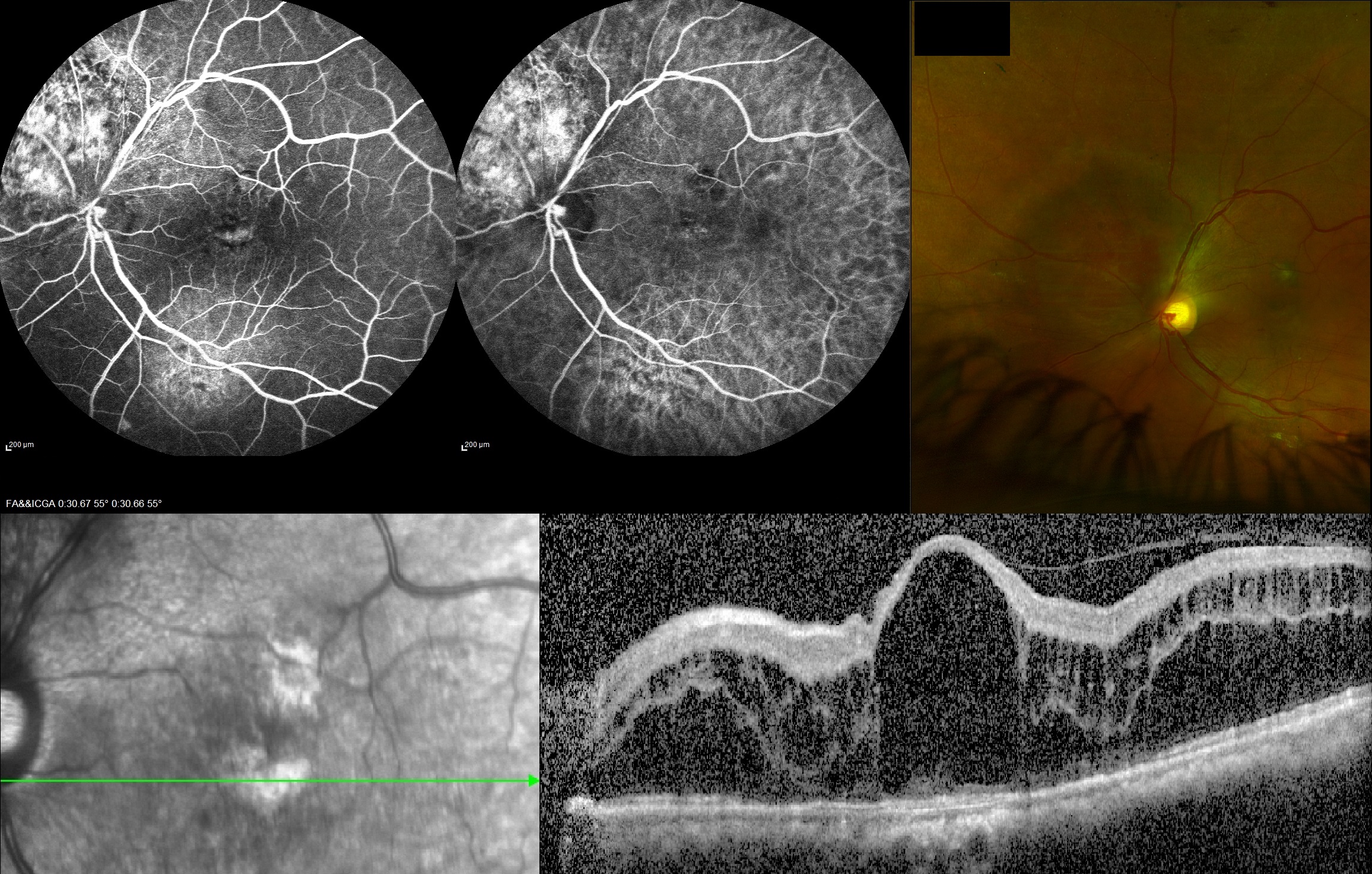
FA (A), ICGA (B), color fundus photo (C) and optical coherence tomography image (D) of the left eye of a patient with circumscribed choroidal hemangioma with macular edema Contributed by Sabareesh Muraleedharan,MS, Aravind eye hospital, Madurai
(Click Image to Enlarge)
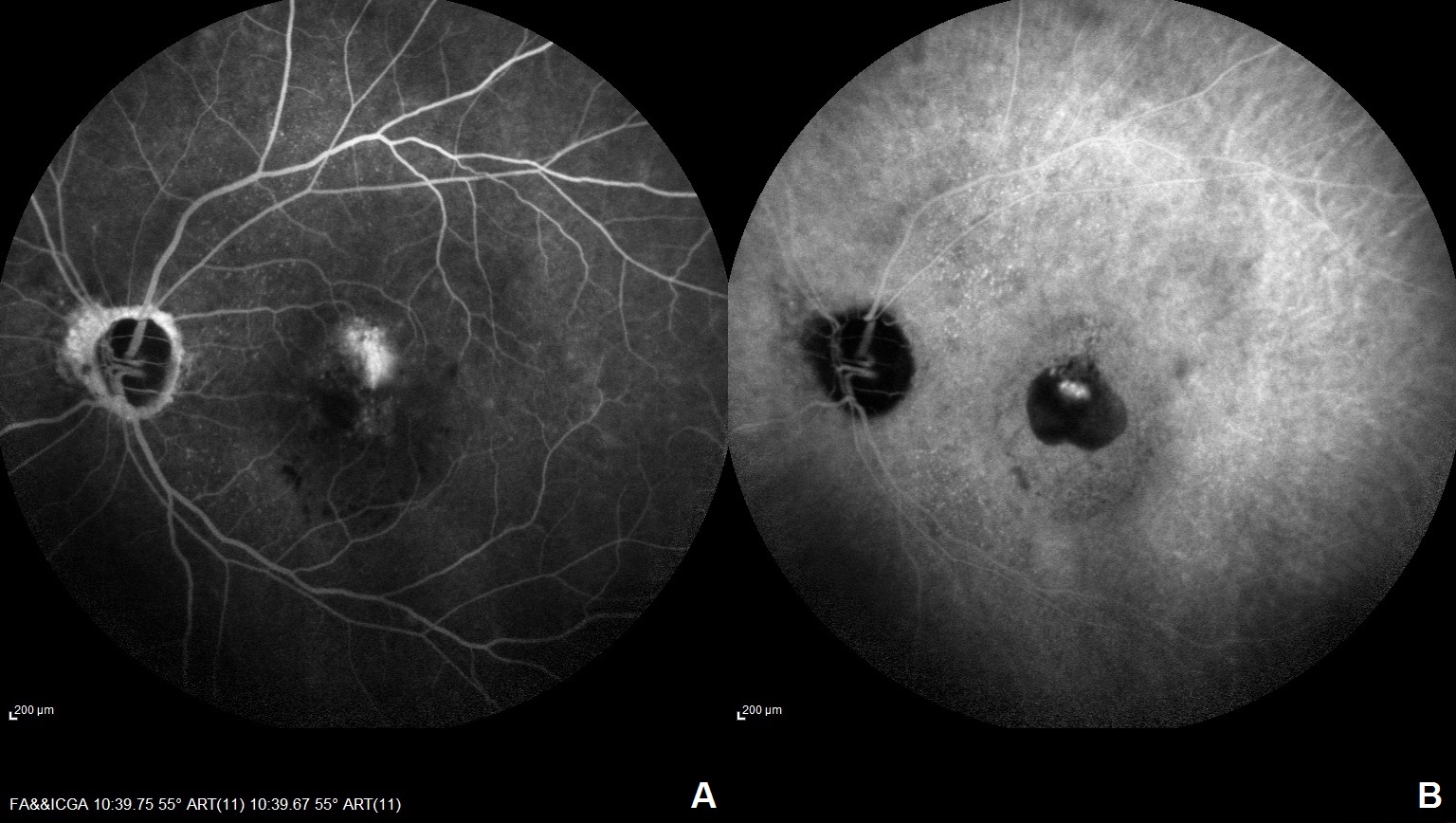
Polypoidal Choroidal Vasculopathy. These images show features of a left eye with polypoidal choroidal vasculopathy via fluorescein angiography (A) and indocyanine green angiography (B).
Contributed by Sabareesh Muraleedharan,MS, Aravind eye hospital, Madurai
(Click Image to Enlarge)
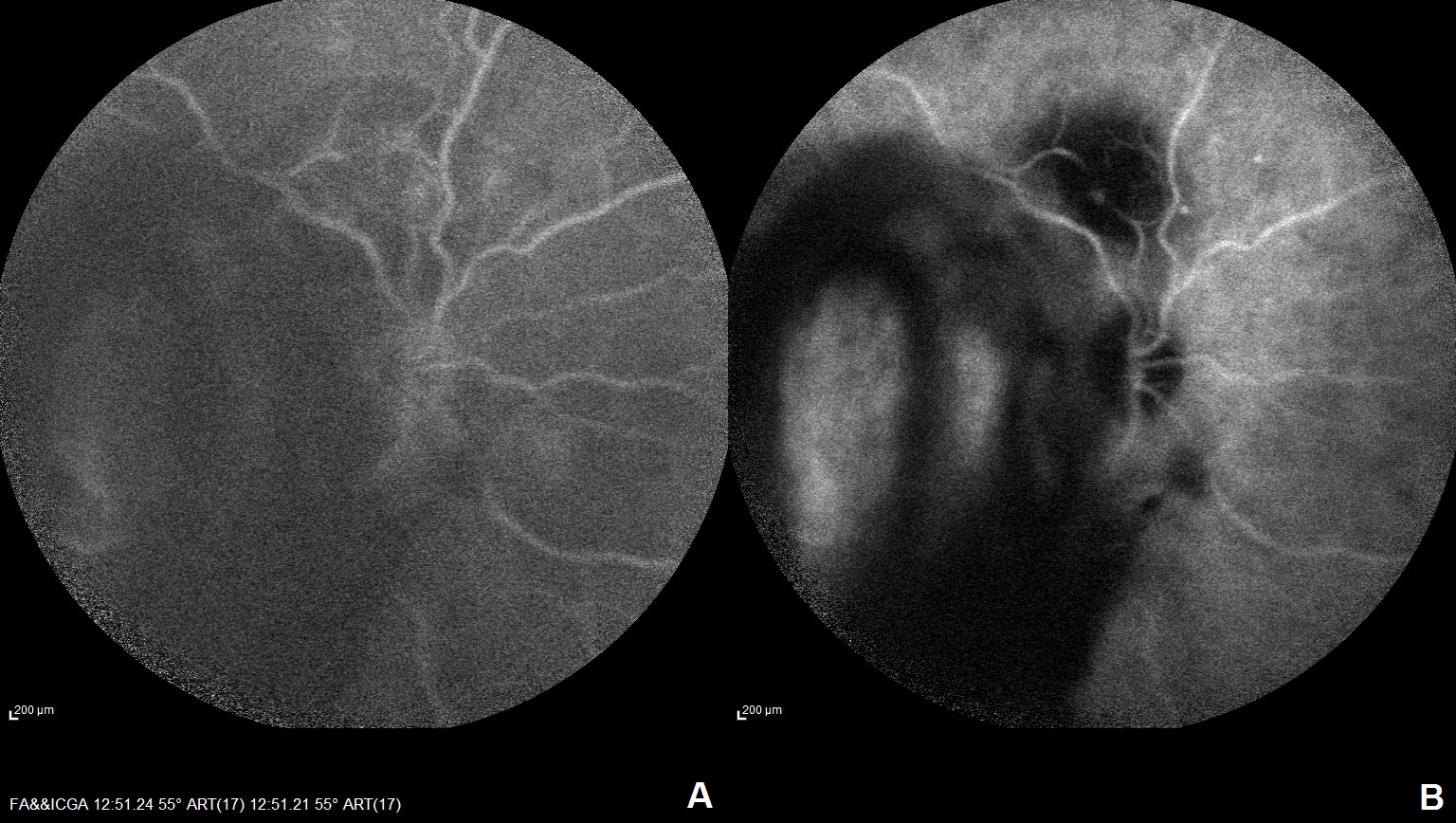
FA (A) and ICGA (B) of the right eye of a patient with RAM at superotemporal arcade with vitreous hemorrhage Contributed by Sabareesh Muraleedharan,MS, Aravind eye hospital, Madurai
(Click Image to Enlarge)
FA (A), ICGA (B) and color fundus photo (C) of the right eye of a patient with MEWDS Contributed by Sabareesh Muraleedharan,MS, Aravind eye hospital, Madurai
(Click Image to Enlarge)
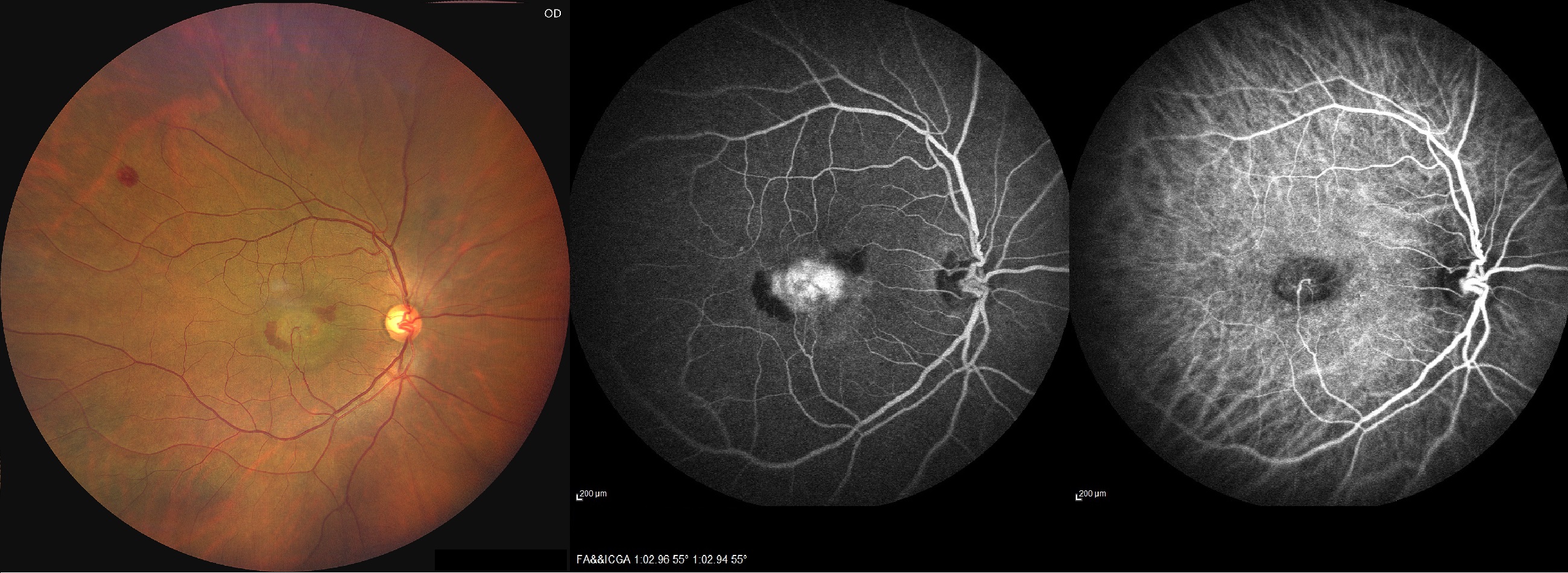
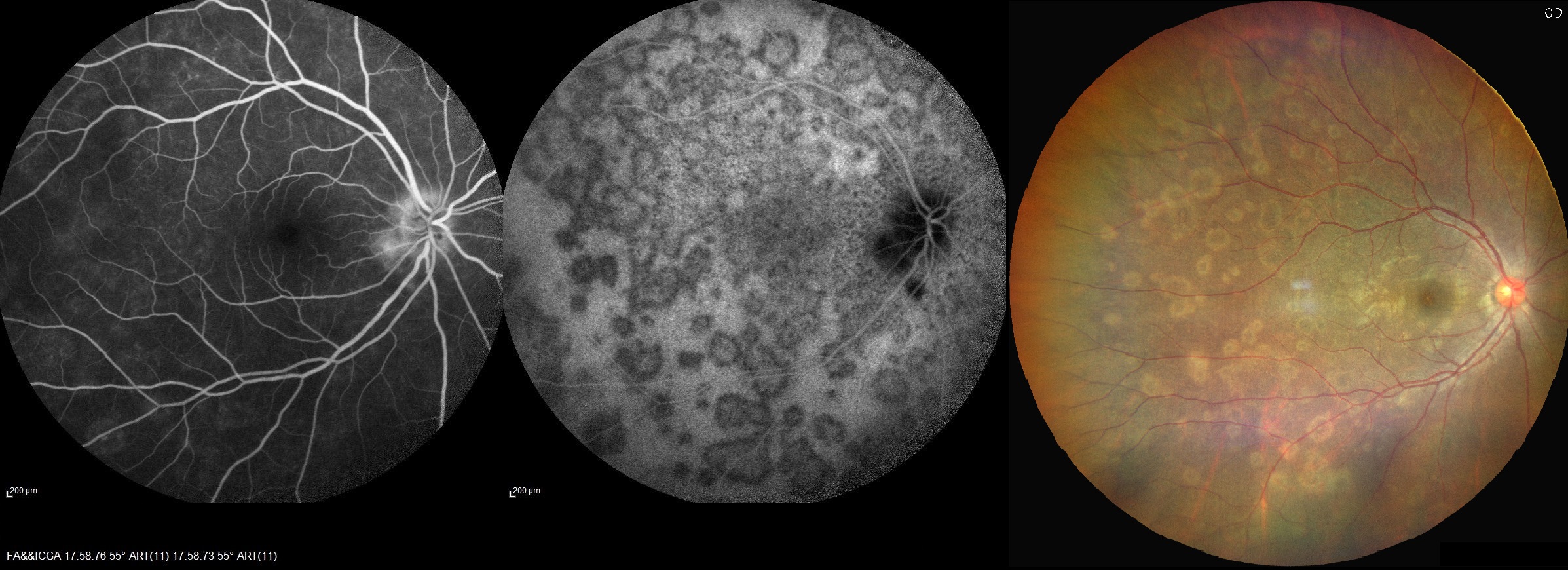
Color fundus photo (A), FA (B) and ICGA (C) of the right eye of a patient with RAP Contributed by Sabareesh Muraleedharan,MS, Aravind eye hospital, Madurai
References
Yannuzzi LA. Indocyanine green angiography: a perspective on use in the clinical setting. American journal of ophthalmology. 2011 May:151(5):745-751.e1. doi: 10.1016/j.ajo.2011.01.043. Epub [PubMed PMID: 21501704]
Level 3 (low-level) evidenceRuia S, Tripathy K. Fluorescein Angiography. StatPearls. 2024 Jan:(): [PubMed PMID: 35015403]
Dzurinko VL, Gurwood AS, Price JR. Intravenous and indocyanine green angiography. Optometry (St. Louis, Mo.). 2004 Dec:75(12):743-55 [PubMed PMID: 15624671]
Invernizzi A, Pellegrini M, Cornish E, Yi Chong Teo K, Cereda M, Chabblani J. Imaging the Choroid: From Indocyanine Green Angiography to Optical Coherence Tomography Angiography. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2020 Jul-Aug:9(4):335-348. doi: 10.1097/APO.0000000000000307. Epub [PubMed PMID: 32739938]
Hu J, Qu J, Piao Z, Yao Y, Sun G, Li M, Zhao M. Optical Coherence Tomography Angiography Compared with Indocyanine Green Angiography in Central Serous Chorioretinopathy. Scientific reports. 2019 Apr 16:9(1):6149. doi: 10.1038/s41598-019-42623-x. Epub 2019 Apr 16 [PubMed PMID: 30992527]
Slakter JS, Yannuzzi LA, Guyer DR, Sorenson JA, Orlock DA. Indocyanine-green angiography. Current opinion in ophthalmology. 1995 Jun:6(3):25-32 [PubMed PMID: 10151085]
Level 3 (low-level) evidenceCraandijk A, Van Beek CA. Indocyanine green fluorescence angiography of the choroid. The British journal of ophthalmology. 1976 May:60(5):377-85 [PubMed PMID: 952809]
Wadekar B, Tripathy K, Chawla R, Venkatesh P, Sharma YR, Vohra R. An 18-year-old female with unilateral painless vision loss. Oman journal of ophthalmology. 2016 Sep-Dec:9(3):193 [PubMed PMID: 27843243]
Tripathy K. Choroidal neovascular membrane in intraocular tuberculosis. GMS ophthalmology cases. 2017:7():Doc24. doi: 10.3205/oc000075. Epub 2017 Sep 1 [PubMed PMID: 28944155]
Level 3 (low-level) evidenceGupta A, Tripathy K. Central Serous Chorioretinopathy. StatPearls. 2024 Jan:(): [PubMed PMID: 32644399]
Paulbuddhe V, Addya S, Gurnani B, Singh D, Tripathy K, Chawla R. Sympathetic Ophthalmia: Where Do We Currently Stand on Treatment Strategies? Clinical ophthalmology (Auckland, N.Z.). 2021:15():4201-4218. doi: 10.2147/OPTH.S289688. Epub 2021 Oct 20 [PubMed PMID: 34707340]
Hayreh SS. THE OPHTHALMIC ARTERY: III. BRANCHES. The British journal of ophthalmology. 1962 Apr:46(4):212-47 [PubMed PMID: 18170772]
Hayreh SS. In vivo choroidal circulation and its watershed zones. Eye (London, England). 1990:4 ( Pt 2)():273-89 [PubMed PMID: 2199236]
Level 3 (low-level) evidenceBorrelli E, Sarraf D, Freund KB, Sadda SR. OCT angiography and evaluation of the choroid and choroidal vascular disorders. Progress in retinal and eye research. 2018 Nov:67():30-55. doi: 10.1016/j.preteyeres.2018.07.002. Epub 2018 Jul 27 [PubMed PMID: 30059755]
Zouache MA, Eames I, Klettner CA, Luthert PJ. Form, shape and function: segmented blood flow in the choriocapillaris. Scientific reports. 2016 Oct 25:6():35754. doi: 10.1038/srep35754. Epub 2016 Oct 25 [PubMed PMID: 27779198]
Hirata Y, Nishiwaki H, Miura S, Ieki Y, Honda Y, Yumikake K, Sugino Y, Okazaki Y. Analysis of choriocapillaris flow patterns by continuous laser-targeted angiography in monkeys. Investigative ophthalmology & visual science. 2004 Jun:45(6):1954-62 [PubMed PMID: 15161863]
Level 3 (low-level) evidenceHayreh SS. Segmental nature of the choroidal vasculature. The British journal of ophthalmology. 1975 Nov:59(11):631-48 [PubMed PMID: 812547]
Level 3 (low-level) evidenceNickla DL, Wallman J. The multifunctional choroid. Progress in retinal and eye research. 2010 Mar:29(2):144-68. doi: 10.1016/j.preteyeres.2009.12.002. Epub 2009 Dec 29 [PubMed PMID: 20044062]
Level 3 (low-level) evidenceO'goshi K, Serup J. Safety of sodium fluorescein for in vivo study of skin. Skin research and technology : official journal of International Society for Bioengineering and the Skin (ISBS) [and] International Society for Digital Imaging of Skin (ISDIS) [and] International Society for Skin Imaging (ISSI). 2006 Aug:12(3):155-61 [PubMed PMID: 16827689]
Grayson MC, Laties AM. Ocular localization of sodium fluorescein. Effects of administration in rabbit and monkey. Archives of ophthalmology (Chicago, Ill. : 1960). 1971 May:85(5):600-3 passim [PubMed PMID: 4996602]
Level 3 (low-level) evidenceLee A, Ra H, Baek J. Choroidal vascular densities of macular disease on ultra-widefield indocyanine green angiography. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2020 Sep:258(9):1921-1929. doi: 10.1007/s00417-020-04772-y. Epub 2020 Jun 3 [PubMed PMID: 32494872]
Cheung CMG, Lai TYY, Teo K, Ruamviboonsuk P, Chen SJ, Kim JE, Gomi F, Koh AH, Kokame G, Jordan-Yu JM, Corvi F, Invernizzi A, Ogura Y, Tan C, Mitchell P, Gupta V, Chhablani J, Chakravarthy U, Sadda SR, Wong TY, Staurenghi G, Lee WK. Polypoidal Choroidal Vasculopathy: Consensus Nomenclature and Non-Indocyanine Green Angiograph Diagnostic Criteria from the Asia-Pacific Ocular Imaging Society PCV Workgroup. Ophthalmology. 2021 Mar:128(3):443-452. doi: 10.1016/j.ophtha.2020.08.006. Epub 2020 Aug 11 [PubMed PMID: 32795496]
Level 3 (low-level) evidenceParravano M, Pilotto E, Musicco I, Varano M, Introini U, Staurenghi G, Menchini U, Virgili G. Reproducibility of fluorescein and indocyanine green angiographic assessment for RAP diagnosis: a multicenter study. European journal of ophthalmology. 2012 Jul-Aug:22(4):598-606. doi: 10.5301/ejo.5000087. Epub [PubMed PMID: 22139618]
Level 2 (mid-level) evidenceSingh D, Tripathy K. Retinal Macroaneurysm. StatPearls. 2024 Jan:(): [PubMed PMID: 35015432]
Mount GR, Kaufman EJ. White Dot Syndromes. StatPearls. 2023 Jan:(): [PubMed PMID: 32491777]
Moshfeghi AA, Harrison SA, Ferrone PJ. Indocyanine green angiography findings in sympathetic ophthalmia. Ophthalmic surgery, lasers & imaging : the official journal of the International Society for Imaging in the Eye. 2005 Mar-Apr:36(2):163-6 [PubMed PMID: 15792321]
Level 3 (low-level) evidenceAgrawal RV, Biswas J, Gunasekaran D. Indocyanine green angiography in posterior uveitis. Indian journal of ophthalmology. 2013 Apr:61(4):148-59. doi: 10.4103/0301-4738.112159. Epub [PubMed PMID: 23685486]
Ma CY, Shi JX, Wang HD, Hang CH, Cheng HL, Wu W. Intraoperative indocyanine green angiography in intracranial aneurysm surgery: Microsurgical clipping and revascularization. Clinical neurology and neurosurgery. 2009 Dec:111(10):840-6. doi: 10.1016/j.clineuro.2009.08.017. Epub 2009 Sep 10 [PubMed PMID: 19747765]
Level 3 (low-level) evidenceHardesty DA, Thind H, Zabramski JM, Spetzler RF, Nakaji P. Safety, efficacy, and cost of intraoperative indocyanine green angiography compared to intraoperative catheter angiography in cerebral aneurysm surgery. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2014 Aug:21(8):1377-82. doi: 10.1016/j.jocn.2014.02.006. Epub 2014 Apr 13 [PubMed PMID: 24736193]
Level 2 (mid-level) evidenceBischoff PM, Flower RW. Ten years experience with choroidal angiography using indocyanine green dye: a new routine examination or an epilogue? Documenta ophthalmologica. Advances in ophthalmology. 1985 Sep 30:60(3):235-91 [PubMed PMID: 2414083]
Level 3 (low-level) evidenceCosta DL, Huang SJ, Orlock DA, Freund KB, Yannuzzi LA, Spaide RF, Gross NE. Retinal-choroidal indocyanine green dye clearance and liver dysfunction. Retina (Philadelphia, Pa.). 2003 Aug:23(4):557-61 [PubMed PMID: 12972775]
Level 3 (low-level) evidenceFineman MS, Maguire JI, Fineman SW, Benson WE. Safety of indocyanine green angiography during pregnancy: a survey of the retina, macula, and vitreous societies. Archives of ophthalmology (Chicago, Ill. : 1960). 2001 Mar:119(3):353-5 [PubMed PMID: 11231768]
Level 3 (low-level) evidenceHassenstein A, Meyer CH. Clinical use and research applications of Heidelberg retinal angiography and spectral-domain optical coherence tomography - a review. Clinical & experimental ophthalmology. 2009 Jan:37(1):130-43. doi: 10.1111/j.1442-9071.2009.02017.x. Epub [PubMed PMID: 19338610]
Cheung CMG, Teo KYC, Tun SBB, Busoy JM, Barathi VA, Spaide RF. Correlation of choriocapillaris hemodynamic data from dynamic indocyanine green and optical coherence tomography angiography. Scientific reports. 2021 Aug 2:11(1):15580. doi: 10.1038/s41598-021-95270-6. Epub 2021 Aug 2 [PubMed PMID: 34341447]
Stanga PE, Lim JI, Hamilton P. Indocyanine green angiography in chorioretinal diseases: indications and interpretation: an evidence-based update. Ophthalmology. 2003 Jan:110(1):15-21; quiz 22-3 [PubMed PMID: 12511340]
Level 1 (high-level) evidencePrünte C, Flammer J. Choroidal capillary and venous congestion in central serous chorioretinopathy. American journal of ophthalmology. 1996 Jan:121(1):26-34 [PubMed PMID: 8554078]
Level 3 (low-level) evidenceHope-Ross M, Yannuzzi LA, Gragoudas ES, Guyer DR, Slakter JS, Sorenson JA, Krupsky S, Orlock DA, Puliafito CA. Adverse reactions due to indocyanine green. Ophthalmology. 1994 Mar:101(3):529-33 [PubMed PMID: 8127574]
Haddad WM, Coscas G, Soubrane G. Eligibility for treatment and angiographic features at the early stage of exudative age related macular degeneration. The British journal of ophthalmology. 2002 Jun:86(6):663-9 [PubMed PMID: 12034690]
Level 2 (mid-level) evidenceFreund KB, Yannuzzi LA, Sorenson JA. Age-related macular degeneration and choroidal neovascularization. American journal of ophthalmology. 1993 Jun 15:115(6):786-91 [PubMed PMID: 7685148]
Guyer DR, Yannuzzi LA, Slakter JS, Sorenson JA, Hanutsaha P, Spaide RF, Schwartz SG, Hirschfeld JM, Orlock DA. Classification of choroidal neovascularization by digital indocyanine green videoangiography. Ophthalmology. 1996 Dec:103(12):2054-60 [PubMed PMID: 9003339]
Yannuzzi LA, Hope-Ross M, Slakter JS, Guyer DR, Sorenson JA, Ho AC, Sperber DE, Freund KB, Orlock DA. Analysis of vascularized pigment epithelial detachments using indocyanine green videoangiography. Retina (Philadelphia, Pa.). 1994:14(2):99-113 [PubMed PMID: 7518607]
Gass JD. Serous retinal pigment epithelial detachment with a notch. A sign of occult choroidal neovascularization. Retina (Philadelphia, Pa.). 1984 Fall-Winter:4(4):205-20 [PubMed PMID: 6085179]
Level 3 (low-level) evidenceKim H, Lee SC, Kim SM, Lee JH, Koh HJ, Kim SS, Byeon SH, Kim M, Lee CS. Identification of Underlying Causes of Spontaneous Submacular Hemorrhage by Indocyanine Green Angiography. Ophthalmologica. Journal international d'ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 2015:233(3-4):146-54. doi: 10.1159/000380830. Epub 2015 Mar 26 [PubMed PMID: 25833061]
Hlushchuk R, Baum O, Gruber G, Wood J, Djonov V. The synergistic action of a VEGF-receptor tyrosine-kinase inhibitor and a sensitizing PDGF-receptor blocker depends upon the stage of vascular maturation. Microcirculation (New York, N.Y. : 1994). 2007 Nov-Dec:14(8):813-25 [PubMed PMID: 17907017]
Level 3 (low-level) evidenceMassacesi AL, Sacchi L, Bergamini F, Bottoni F. The prevalence of retinal angiomatous proliferation in age-related macular degeneration with occult choroidal neovascularization. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2008 Jan:246(1):89-92 [PubMed PMID: 17653567]
Kuhn D, Meunier I, Soubrane G, Coscas G. Imaging of chorioretinal anastomoses in vascularized retinal pigment epithelium detachments. Archives of ophthalmology (Chicago, Ill. : 1960). 1995 Nov:113(11):1392-8 [PubMed PMID: 7487600]
Bressler NM. Retinal anastomosis to choroidal neovascularization: a bum rap for a difficult disease. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 Dec:123(12):1741-3 [PubMed PMID: 16344449]
Ghazi NG, Knape RM, Kirk TQ, Tiedeman JS, Conway BP. Intravitreal bevacizumab (avastin) treatment of retinal angiomatous proliferation. Retina (Philadelphia, Pa.). 2008 May:28(5):689-95. doi: 10.1097/IAE.0b013e318162d982. Epub [PubMed PMID: 18463511]
Level 2 (mid-level) evidenceBottoni F, Massacesi A, Cigada M, Viola F, Musicco I, Staurenghi G. Treatment of retinal angiomatous proliferation in age-related macular degeneration: a series of 104 cases of retinal angiomatous proliferation. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 Dec:123(12):1644-50 [PubMed PMID: 16344434]
Level 2 (mid-level) evidenceRouvas AA, Papakostas TD, Vavvas D, Vergados I, Moschos MM, Kotsolis A, Ladas ID. Intravitreal ranibizumab, intravitreal ranibizumab with PDT, and intravitreal triamcinolone with PDT for the treatment of retinal angiomatous proliferation: a prospective study. Retina (Philadelphia, Pa.). 2009 Apr:29(4):536-44. doi: 10.1097/IAE.0b013e318196b1de. Epub [PubMed PMID: 19190547]
Level 1 (high-level) evidenceSaito M, Shiragami C, Shiraga F, Kano M, Iida T. Comparison of intravitreal triamcinolone acetonide with photodynamic therapy and intravitreal bevacizumab with photodynamic therapy for retinal angiomatous proliferation. American journal of ophthalmology. 2010 Mar:149(3):472-81.e1. doi: 10.1016/j.ajo.2009.09.016. Epub 2010 Jan 6 [PubMed PMID: 20053392]
Level 2 (mid-level) evidenceKoh AH, Expert PCV Panel, Chen LJ, Chen SJ, Chen Y, Giridhar A, Iida T, Kim H, Yuk Yau Lai T, Lee WK, Li X, Han Lim T, Ruamviboonsuk P, Sharma T, Tang S, Yuzawa M. Polypoidal choroidal vasculopathy: evidence-based guidelines for clinical diagnosis and treatment. Retina (Philadelphia, Pa.). 2013 Apr:33(4):686-716. doi: 10.1097/IAE.0b013e3182852446. Epub [PubMed PMID: 23455233]
Level 1 (high-level) evidenceYannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina (Philadelphia, Pa.). 1990:10(1):1-8 [PubMed PMID: 1693009]
Koh A, Lee WK, Chen LJ, Chen SJ, Hashad Y, Kim H, Lai TY, Pilz S, Ruamviboonsuk P, Tokaji E, Weisberger A, Lim TH. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina (Philadelphia, Pa.). 2012 Sep:32(8):1453-64 [PubMed PMID: 22426346]
Level 1 (high-level) evidenceLai TY, Chan WM, Liu DT, Luk FO, Lam DS. Intravitreal bevacizumab (Avastin) with or without photodynamic therapy for the treatment of polypoidal choroidal vasculopathy. The British journal of ophthalmology. 2008 May:92(5):661-6. doi: 10.1136/bjo.2007.135103. Epub 2008 Mar 20 [PubMed PMID: 18356265]
Level 2 (mid-level) evidenceGoldman DR, Freund KB, McCannel CA, Sarraf D. Peripheral polypoidal choroidal vasculopathy as a cause of peripheral exudative hemorrhagic chorioretinopathy: a report of 10 eyes. Retina (Philadelphia, Pa.). 2013 Jan:33(1):48-55. doi: 10.1097/IAE.0b013e31825df12a. Epub [PubMed PMID: 22836900]
Level 3 (low-level) evidenceSpaide RF, Hall L, Haas A, Campeas L, Yannuzzi LA, Fisher YL, Guyer DR, Slakter JS, Sorenson JA, Orlock DA. Indocyanine green videoangiography of older patients with central serous chorioretinopathy. Retina (Philadelphia, Pa.). 1996:16(3):203-13 [PubMed PMID: 8789858]
Yannuzzi LA, Slakter JS, Gross NE, Spaide RF, Costa D, Huang SJ, Klancnik JM Jr, Aizman A. Indocyanine green angiography-guided photodynamic therapy for treatment of chronic central serous chorioretinopathy: a pilot study. Retina (Philadelphia, Pa.). 2003 Jun:23(3):288-98 [PubMed PMID: 12824827]
Level 3 (low-level) evidenceYannuzzi LA, Freund KB, Goldbaum M, Scassellati-Sforzolini B, Guyer DR, Spaide RF, Maberley D, Wong DW, Slakter JS, Sorenson JA, Fisher YL, Orlock DA. Polypoidal choroidal vasculopathy masquerading as central serous chorioretinopathy. Ophthalmology. 2000 Apr:107(4):767-77 [PubMed PMID: 10768341]
Level 3 (low-level) evidenceGuyer DR, Yannuzzi LA, Slakter JS, Sorenson JA, Ho A, Orlock D. Digital indocyanine green videoangiography of central serous chorioretinopathy. Archives of ophthalmology (Chicago, Ill. : 1960). 1994 Aug:112(8):1057-62 [PubMed PMID: 8053819]
Tsujikawa A, Ojima Y, Yamashiro K, Ooto S, Tamura H, Nakagawa S, Yoshimura N. Punctate hyperfluorescent spots associated with central serous chorioretinopathy as seen on indocyanine green angiography. Retina (Philadelphia, Pa.). 2010 May:30(5):801-9. doi: 10.1097/IAE.0b013e3181c72068. Epub [PubMed PMID: 20094008]
Level 2 (mid-level) evidenceChung H, Byeon SH, Freund KB. FOCAL CHOROIDAL EXCAVATION AND ITS ASSOCIATION WITH PACHYCHOROID SPECTRUM DISORDERS: A Review of the Literature and Multimodal Imaging Findings. Retina (Philadelphia, Pa.). 2017 Feb:37(2):199-221. doi: 10.1097/IAE.0000000000001345. Epub [PubMed PMID: 27749784]
Cheung CMG, Lee WK, Koizumi H, Dansingani K, Lai TYY, Freund KB. Pachychoroid disease. Eye (London, England). 2019 Jan:33(1):14-33. doi: 10.1038/s41433-018-0158-4. Epub 2018 Jul 11 [PubMed PMID: 29995841]
Schneider U, Wagner AL, Kreissig I. Indocyanine green videoangiography of hemorrhagic retinal arterial macroaneurysms. Ophthalmologica. Journal international d'ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 1997:211(2):115-8 [PubMed PMID: 9097320]
Level 3 (low-level) evidenceMueller AJ, Freeman WR, Schaller UC, Kampik A, Folberg R. Complex microcirculation patterns detected by confocal indocyanine green angiography predict time to growth of small choroidal melanocytic tumors: MuSIC Report II. Ophthalmology. 2002 Dec:109(12):2207-14 [PubMed PMID: 12466160]
Arevalo JF, Shields CL, Shields JA, Hykin PG, De Potter P. Circumscribed choroidal hemangioma: characteristic features with indocyanine green videoangiography. Ophthalmology. 2000 Feb:107(2):344-50 [PubMed PMID: 10690837]
Howe LJ, Stanford MR, Graham EM, Marshall J. Choroidal abnormalities in birdshot chorioretinopathy: an indocyanine green angiography study. Eye (London, England). 1997:11 ( Pt 4)():554-9 [PubMed PMID: 9425423]
Slakter JS, Giovannini A, Yannuzzi LA, Scassellati-Sforzolini B, Guyer DR, Sorenson JA, Spaide RF, Orlock D. Indocyanine green angiography of multifocal choroiditis. Ophthalmology. 1997 Nov:104(11):1813-9 [PubMed PMID: 9373111]
Dell'omo R, Wong R, Marino M, Konstantopoulou K, Pavesio C. Relationship between different fluorescein and indocyanine green angiography features in multiple evanescent white dot syndrome. The British journal of ophthalmology. 2010 Jan:94(1):59-63. doi: 10.1136/bjo.2009.163550. Epub 2009 Aug 18 [PubMed PMID: 19692364]
Level 2 (mid-level) evidenceGiovannini A, Mariotti C, Ripa E, Scassellati-Sforzolini B. Indocyanine green angiographic findings in serpiginous choroidopathy. The British journal of ophthalmology. 1996 Jun:80(6):536-40 [PubMed PMID: 8759265]
Howe LJ, Woon H, Graham EM, Fitzke F, Bhandari A, Marshall J. Choroidal hypoperfusion in acute posterior multifocal placoid pigment epitheliopathy. An indocyanine green angiography study. Ophthalmology. 1995 May:102(5):790-8 [PubMed PMID: 7777278]
Level 3 (low-level) evidenceTiffin PA, Maini R, Roxburgh ST, Ellingford A. Indocyanine green angiography in a case of punctate inner choroidopathy. The British journal of ophthalmology. 1996 Jan:80(1):90-1 [PubMed PMID: 8664243]
Level 3 (low-level) evidenceLevy J, Shneck M, Klemperer I, Lifshitz T. Punctate inner choroidopathy: resolution after oral steroid treatment and review of the literature. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2005 Oct:40(5):605-8 [PubMed PMID: 16391624]
Level 3 (low-level) evidenceMrejen S, Khan S, Gallego-Pinazo R, Jampol LM, Yannuzzi LA. Acute zonal occult outer retinopathy: a classification based on multimodal imaging. JAMA ophthalmology. 2014 Sep:132(9):1089-98. doi: 10.1001/jamaophthalmol.2014.1683. Epub [PubMed PMID: 24945598]
Level 2 (mid-level) evidenceGiani A, Pellegrini M, Carini E, Peroglio Deiro A, Bottoni F, Staurenghi G. The dark atrophy with indocyanine green angiography in Stargardt disease. Investigative ophthalmology & visual science. 2012 Jun 26:53(7):3999-4004. doi: 10.1167/iovs.11-9258. Epub 2012 Jun 26 [PubMed PMID: 22589445]
Level 2 (mid-level) evidenceBernasconi O, Auer C, Zografos L, Herbort CP. Indocyanine green angiographic findings in sympathetic ophthalmia. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 1998 Aug:236(8):635-8 [PubMed PMID: 9717662]
Level 3 (low-level) evidenceHerbort CP, Mantovani A, Bouchenaki N. Indocyanine green angiography in Vogt-Koyanagi-Harada disease: angiographic signs and utility in patient follow-up. International ophthalmology. 2007 Apr-Jun:27(2-3):173-82 [PubMed PMID: 17457515]
Bouchenaki N, Herbort CP. Indocyanine green angiography guided management of vogt-koyanagi-harada disease. Journal of ophthalmic & vision research. 2011 Oct:6(4):241-8 [PubMed PMID: 22454746]