Introduction
Retrobulbar hematoma (RBH) is a rare yet sight-threatening diagnosis.[1] Although mild cases may occur, a devastating consequence is orbital compartment syndrome, potentially leading to complete vision loss if not treated promptly. The definitive management is lateral orbital canthotomy and cantholysis, which can be vision-saving. See Image. Retrobulbar Hematoma.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The development of a retrobulbar hematoma is most commonly associated with trauma, especially orbital floor fractures. However, a retrobulbar hematoma can also develop iatrogenically following sinus or ocular surgery. The incidence of retrobulbar hematoma secondary to these etiologies is very low. For example, the incidence of RBH after retrobulbar or peribulbar injection, zygomatic fracture repair, and blepharoplasty is 2%, 0.3%, and 0.055%, respectively.[2]
Rarely, a retrobulbar hematoma can develop from Valsalva maneuvers in the context of anticoagulation. One case report describes a 31-year-old female who developed headache and blurry vision after sneezing and was found to have a spontaneous retrobulbar hematoma. Other etiologies include vascular anomalies, coagulopathies, and uncontrolled hypertension.[3]
Epidemiology
The incidence of retrobulbar hematoma varies depending on the etiology and can range from less than 1% (post-surgical) to 4% (trauma). One study, comprised of 1,386 patients with facial trauma at a tertiary care trauma center, reported the incidence of RBH to be 3.6%. The incidence of permanent blindness in this population was 0.14%.[4]
Another study, which included 426 patients that underwent orbital wall fracture repair, reported an incidence of 1.2% for post-operative RBH. In this case series, the patients that developed RBH retained their normal visual acuity. Other incidence rates reported in the literature for RBH are 0.6% and 0.055% following orbital reconstruction and blepharoplasty, respectively.[5]
Pathophysiology
The defining pathophysiology of a retrobulbar hematoma is blood collecting in the retrobulbar space, which, as its name implies, is posterior to the globe. Although a mild fluid collection in orbit is tolerable, rapid hemorrhaging is not well compensated. As blood accumulates in this confined space, intraorbital pressure rapidly rises, causing increased venous pooling and a corresponding increase in intraocular pressure (IOP), decreased arterial flow, and essentially an orbital compartment syndrome.[6]
Additionally, the increase in orbital pressure results in a forward globe displacement and stretching of the optic nerve, known as proptosis (see Image. Retrobulbar Hematoma With Proptosis Noted on Computed Tomography). Furthermore, perfusion to the intraocular structures is compromised if the orbital pressure exceeds the central retinal artery pressure.[7] A significantly elevated intraocular pressure lasting 60 to 100 minutes can cause permanent vision loss.[8]
History and Physical
Upon presentation, patients may very likely report a history of trauma. Care should be taken to elicit the mechanism of injury to assess for more emergent diagnoses such as penetrating or perforating ocular trauma and possible globe rupture. Patients may complain of diplopia, headache, nausea, and vomiting. Some common signs and symptoms are eye pain, periorbital ecchymosis, decreased visual acuity, elevated IOP, a tense and progressive proptosis, ophthalmoplegia, and optic disc swelling.[1] A thorough ophthalmic exam should be completed. Visual acuity should be assessed for the right and left eye separately. One should check direct and indirect pupillary responses to light with careful attention to the presence or absence of a relative afferent pupillary defect. Extra-ocular movements should be assessed, as a restriction in motility can be a concerning orbital.[3]
Intraocular pressure is an essential part of the physical exam. Although orbital pressure is not commonly measured directly in the clinical setting as it requires manometry, elevated IOP (normal range between 8 and 21 mmHg) and proptosis correlate well with orbital compartment pressure and are sufficient to indicate an impending orbital compartment syndrome.[9]
Patients can sometimes be unconscious or uncooperative, hindering the physician from obtaining a complete history and physical examination. Although multiple traumatic injuries and altered consciousness can make it challenging to evaluate a retrobulbar hematoma, it is imperative to obtain as much information as possible to gauge the severity of the trauma and obtain a rapid diagnosis.[2] Assessing for proptosis, resistance to retropulsion, pupillary responsiveness, IOP, and physical signs such as tense and edematous lids may indicate the presence of increased orbital pressure and aid in diagnosis. If the signs and symptoms of optic nerve ischemia from RBH are present and an IOP of 40 mmHg or more significant, immediate treatment should be initiated.[10]
Evaluation
Although radiographic testing can help to confirm a retrobulbar hematoma, the diagnosis is clinical.[5] RBH cases can range from mild, with no visual consequences, to severe, with orbital compartment syndrome (OCS). One retrospective chart review identified 32.3% of orbital wall fractures as having an associated retrobulbar hematoma via computed tomography (CT) scan. However, only 1.1% of these had orbital compartment syndrome requiring intervention.[11]
These results reinforce the importance of a thorough clinical exam. CT imaging can be used to help visualize the extent of the hematoma, as well as identify other associated injuries such as maxillofacial fractures, globe rupture, or intraocular foreign bodies. A CT scan may also reveal optic nerve tension or a distorted posterior globe. If a patient displays the signs and symptoms typical of optic nerve ischemia from RBH, however, radiographic imaging should be delayed in favor of prompt surgical intervention.
Treatment / Management
Once the diagnosis of a retrobulbar hematoma is confirmed, ophthalmology should be emergently consulted. However, if optic nerve ischemia is suspected and intraocular pressure is greater than or equal to 40 mmHg, the attending physician should not delay definitive management.[7] Adequate anesthesia and antiemetics should be provided to aid in patient comfort and help prevent Valsalva maneuvers such as vomiting. A vital part of management is immediate orbital decompression with lateral orbital canthotomy and cantholysis (LOCC).
If possible, the surgical area should be prepped sterilely and cleaned with povidone-iodine solution. Otherwise, saline irrigation may be sufficient in this emergent situation. Adequate anesthesia (1 to 2 milliliters of lidocaine 1% to 2% with epinephrine 1 to 100,00) should be administered into the cutaneous and deep tissues of the lateral canthus. Care should be taken to point the needle away from the globe when injecting. Next, the surgical area must be irrigated with sterile water to visualize important landmarks and flush away any foreign debris that may be present. Once there is adequate visualization, a hemostat can be used to clamp horizontally across the lateral canthus for approximately one minute to aid in hemostasis and create a physical marker for cutting. After this, forceps should be used to raise the skin of the lower eyelid, and the lateral canthus should be cut 1 to 2 cm with Wescott scissors.[2]
The canthotomy will expose the lateral canthal tendon, which can also be identified with a strumming motion using scissors. The lateral canthal tendon can be further exposed by pulling down on the lateral lower lid with a hemostat or forceps. The tendon’s inferior crus should be cut by pointing the scissors inferoposteriorly. At this point, the lower eyelid should be completely mobile. LOCC helps alleviate the increased intraorbital pressure by freeing the lower eyelid from the orbit. The lateral canthal incision may need to be repaired at a later date.[7]
Mild cases of RBH without signs or symptoms of optic nerve compromise should be managed by observation and/or medical treatment.[10] Patients with RBH and no symptoms or elevated IOP can be monitored without intervention. IOP should be reassessed approximately 6 hours after the initial evaluation to ensure that there is no interim elevation which could signify a possible rebleed and be an indication for intervention. Alternative methods described in the literature for mild to moderate cases are direct needle aspiration of the hematoma and the use of topical, oral, or intravenous medications such as beta-blockers (timolol maleate), steroids, and osmotic agents (mannitol).[5]
Reports have shown these to help lower intraocular pressure. Acetazolamide is another well-studied drug that can be administered orally or intravenously to successfully lower IOP.[12] Steroids may also protect against traumatic optic neuropathy. For all cases, appropriate follow-up with ophthalmology should be established. The frequency of monitoring will depend on the patient’s severity of RBH.
In cases of postoperative RBH, prevention may be an effective form of management. Although specific risk factors for postoperative RBH have not been well-established in the literature, surgical optimization may be preventative. Case series have reported the development of RBH in patients using anticoagulants at the time of orbital wall fracture repair and orbitotomy. In light of this, it may be advisable to inform patients to stop non-essential anticoagulants before surgical repair. Perioperatively, adequate hemostasis should be achieved. The prevention of Valsalva maneuvers during the procedure may also be helpful.[5]
Differential Diagnosis
Other conditions to consider in patients with the signs and symptoms mentioned above, especially in the setting of trauma, including globe rupture and orbital fractures with entrapment.[1]
Prognosis
The prognosis for most patients that receive timely intervention is favorable. Most patients treated within 2 hours of presentation have been shown to attain a visual acuity better than 20/40. This is in contrast to those receiving treatment after 2 hours, only 25% of which may achieve 20/40 vision or better.[13] Case reports of patients with traumatic RBH and ‘No Light Perception’ vision have described the recovery of some vision after LOCC.[7]
Some factors that may point toward a poorer prognosis are a presenting visual acuity worse than 20/200, the presence of a relative afferent pupillary defect, an eyelid laceration, and increased time to treatment.[14] Retrobulbar hematoma associated with a traumatic etiology and a greater number of symptoms also has a poorer prognosis.[15]
With traumatic retrobulbar hemorrhage and acute vision loss, the risk of permanent blindness is 44 to 52%.[10] As stated earlier, the incidence of permanent visual loss from RBH is much lower for post-surgical etiologies.
Complications
Complications of LOCC include a persistently elevated IOP, which may indicate inadequate cantholysis. In this case, one should ensure that an adequate inferior cantholysis was performed.[6] Once this is ascertained, an additional cantholysis may still need to be performed on the superior crus of the lateral canthal tendon in order to achieve adequate orbital decompression. Other complications from performing a lateral orbital canthotomy include damage to nearby ocular structures, globe rupture, infection, bleeding, and eyelid malpositioning.[7]
Loss of lower eyelid suspension can produce cosmetic concerns, which can be addressed non-urgently by ophthalmologists trained in oculoplastic surgery once the immediate threat of vision loss has subsided.
Postoperative and Rehabilitation Care
After a complete LOCC, visual acuity, IOP, pupillary function, and other signs of optic nerve ischemia should be reassessed. The patient may require adjuvant therapy with topical IOP-lowering drops or systemic agents. The surgical site should also be monitored at appropriate intervals for signs of infection. Topical ophthalmic antibiotic ointment (e.g., erythromycin, bacitracin) should be applied over the surgical site.
Consultations
An ophthalmology consult is warranted in the evaluation and management of RBH. Depending on the extent of the condition or associated injuries, other services may be required. Oral maxillofacial surgery (OMFS) or otolaryngology (ENT) should be consulted for orbital wall fractures as per the established trauma protocols of the treating facility.
Deterrence and Patient Education
Patients should be educated on the importance of prevention and ocular safety. Appropriate eye protection, especially in high-risk areas (construction, sports, military, etc.), should be prioritized. The use of helmets, face shields, and safety goggles should be encouraged in the appropriate situation. Eye protection should especially be advocated for in monocular patients.
Pearls and Other Issues
Obtain ophthalmology consultation emergently, but do not delay definitive management if an orbital compartment syndrome from retrobulbar hematoma is suspected or confirmed.
Enhancing Healthcare Team Outcomes
Although the development of a retrobulbar hematoma is rare, ocular trauma is fairly common and can have devastating consequences. The majority of these cases are present in the emergency room setting. The on-call ophthalmologist should be consulted immediately. However, the presence of rapidly deteriorating vision, signs and symptoms of orbital compartment syndrome, and unavailability of timely ophthalmologic consultation should prompt treatment by the available physician.[7] Emergency room physicians should be equipped to perform a LOCC if necessary, improving outcomes for patients with clinically significant retrobulbar hematoma.
Studies have shown that further education is needed in regards to performing a lateral canthotomy and cantholysis. This is primarily due to the low frequency of RBH, which prevents emergency medicine physicians from having ample opportunity to perform this procedure. One study conducted in a level one trauma center in the United States revealed an average of only five lateral canthotomies per year.[16]
A 2019 prospective cohort study revealed that only 37.1% of non-ophthalmic emergency medicine physicians would perform a LOCC when necessary. An overwhelming 92.2% reported an unwillingness to perform a LOCC themselves due to inadequate training. This study underscores the need for collaborative training in this area among emergency medicine physicians and ophthalmologists. The use of porcine models for LOCC practice has been documented as an excellent teaching method for residents.[10] Such training can be vital since irreversible vision loss can be prevented if LOCC is performed within two hours of patient presentation.[7][16] [Level 3]
Media
(Click Image to Enlarge)

Retrobulbar Hematoma. The patient developed severe pain in the left eye and orbit after an uneventful upper blepharoplasty. The patient was not seen and examined until the following morning when this photograph was taken. The patient has no perception of light in the left eye. A canthotomy, cantholysis, and evacuation of orbital hemorrhage did not help this patient, as this should have been performed much earlier.
Contributed by Prof. BCK Patel MD, FRCS
(Click Image to Enlarge)
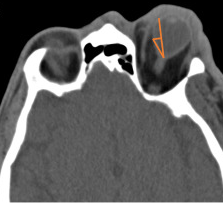
Retrobulbar Hematoma With Proptosis Noted on Computed Tomography.
Contributed by l Mohseni, MD
References
Mohseni M, Blair K, Gurnani B, Bragg BN. Blunt Eye Trauma. StatPearls. 2024 Jan:(): [PubMed PMID: 29261988]
Pamukcu C, Odabaşı M. Acute retrobulbar haemorrhage: An ophthalmologic emergency for the emergency physician. Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES. 2015 Jul:21(4):309-14. doi: 10.5505/tjtes.2015.16768. Epub [PubMed PMID: 26374422]
Deveer M, Cullu N, Beydilli H, Sozen H, Yeniceri O, Parlak S. Spontaneous Retrobulbar Haematoma. Case reports in radiology. 2015:2015():796834. doi: 10.1155/2015/796834. Epub 2015 May 10 [PubMed PMID: 26090258]
Level 3 (low-level) evidenceFattahi T,Brewer K,Retana A,Ogledzki M, Incidence of retrobulbar hemorrhage in the emergency department. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2014 Dec; [PubMed PMID: 25249171]
Park JH, Kim I, Son JH. Incidence and management of retrobulbar hemorrhage after blowout fracture repair. BMC ophthalmology. 2021 Apr 22:21(1):186. doi: 10.1186/s12886-021-01943-1. Epub 2021 Apr 22 [PubMed PMID: 33888073]
Rowh AD, Ufberg JW, Chan TC, Vilke GM, Harrigan RA. Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. The Journal of emergency medicine. 2015 Mar:48(3):325-30. doi: 10.1016/j.jemermed.2014.11.002. Epub 2014 Dec 16 [PubMed PMID: 25524455]
Level 3 (low-level) evidenceDesai NM, Shah SU. Lateral Orbital Canthotomy. StatPearls. 2024 Jan:(): [PubMed PMID: 32491408]
Kloss BT,Patel R, Orbital compartment syndrome from retrobulbar hemorrhage. International journal of emergency medicine. 2010 Oct 23; [PubMed PMID: 21373353]
Enz TJ, Papazoglou A, Tappeiner C, Menke MN, Benitez BK, Tschopp M. Minimally invasive measurement of orbital compartment pressure and implications for orbital compartment syndrome: a pilot study. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2021 Nov:259(11):3413-3419. doi: 10.1007/s00417-021-05222-z. Epub 2021 Jun 7 [PubMed PMID: 34097110]
Level 3 (low-level) evidenceBallard SR, Enzenauer RW, O'Donnell T, Fleming JC, Risk G, Waite AN. Emergency lateral canthotomy and cantholysis: a simple procedure to preserve vision from sight threatening orbital hemorrhage. Journal of special operations medicine : a peer reviewed journal for SOF medical professionals. 2009 Summer:9(3):26-32. doi: 10.55460/1CLD-XJUV. Epub [PubMed PMID: 19739474]
Kondoff M, Nassrallah G, Ross M, Deschênes J. Incidence and outcomes of retrobulbar hematoma diagnosed by computed tomography in cases of orbital fracture. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2019 Oct:54(5):606-610. doi: 10.1016/j.jcjo.2019.01.006. Epub 2019 Apr 2 [PubMed PMID: 31564352]
Level 3 (low-level) evidenceLoiselle AR, de Kleine E, van Dijk P, Jansonius NM. Intraocular and intracranial pressure in glaucoma patients taking acetazolamide. PloS one. 2020:15(6):e0234690. doi: 10.1371/journal.pone.0234690. Epub 2020 Jun 18 [PubMed PMID: 32555666]
McCallum E, Keren S, Lapira M, Norris JH. Orbital Compartment Syndrome: An Update With Review Of The Literature. Clinical ophthalmology (Auckland, N.Z.). 2019:13():2189-2194. doi: 10.2147/OPTH.S180058. Epub 2019 Nov 7 [PubMed PMID: 31806931]
Bailey LA, van Brummen AJ, Ghergherehchi LM, Chuang AZ, Richani K, Phillips ME. Visual Outcomes of Patients With Retrobulbar Hemorrhage Undergoing Lateral Canthotomy and Cantholysis. Ophthalmic plastic and reconstructive surgery. 2019 Nov/Dec:35(6):586-589. doi: 10.1097/IOP.0000000000001401. Epub [PubMed PMID: 31693632]
Christie B,Block L,Ma Y,Wick A,Afifi A, Retrobulbar hematoma: A systematic review of factors related to outcomes. Journal of plastic, reconstructive [PubMed PMID: 29239798]
Level 1 (high-level) evidenceRaikin J, Hall RV, Papanagnou D. "Trauma to the Eye"-A Low Fidelity Resident Teaching Module for Identifying and Treating a Retrobulbar Hematoma. MedEdPORTAL : the journal of teaching and learning resources. 2021 Jan 25:17():11075. doi: 10.15766/mep_2374-8265.11075. Epub 2021 Jan 25 [PubMed PMID: 33521252]