Introduction
A prism is a transparent, triangular refracting surface with an apex and a base.[1] The two nonparallel surfaces intersect at an angle called the apex, and the surface opposite to the apex forms the bottom of the prism. The light rays refracted through the prism bend towards the base. The amount of deviation of the path of refracted light from the incident light depends on the power of the prism measured in "prism diopters."[2]
Charles Prentice was the first to introduce the term prism diopters to describe the intensity of prism. One prism diopter represents the deviation of light by 1 centimeter and perpendicular to the initial direction of the light ray on a plane placed 1 meter away from the prism. The power of the prism in prism diopters is represented by the symbol D. Thus, a prism of 2 prism diopters would deviate a light ray by 2 centimeters, perpendicular to the direction of the initial light ray, measured 100 cm beyond the prism.[3]
Another unit of measurement of prism power is centrad. This is less frequently used as compared to prism diopters. Centrad unit is represented by the symbol Ñ. One centrad represents the deviation of light by 1 centimeter and perpendicular to the initial direction of the light ray on an arc of a circle 1 meter away from the prism.[4] Further, the deflection of the light ray after passing through the prism also depends on the refractive index of the material and the position in which the prism is held. It is essential to understand that the light ray passing through the prism deviates towards its base, but the image appears to be displaced towards the apex. Thus, the eye being tested will deviate towards the apex of the prism.[5]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
A light ray passing through the prism obeys Snell's law.[6] The light ray deviates towards the base, and this causes the image displacement away from the base of the prism, i.e., towards the apex. The change of the direction of the ray is called the angle of deviation.[7] When a prism is placed in the air, the angle of deviation of the light ray is determined by three factors angle of incidence, refracting angle of the prism, and refractive index of the prism material.[8]
The characteristics of the light deviated through prism include:
- No magnification/minification of the image
- No change in vergence of the rays
- Disperses incident pencil rays into component colors
- A virtual, erect image is formed
- The image should deviate through the apex of the prism[9]
Prentice's rule measures the deviation produced by the prism.[10]
- D = cF
- c = image displacement in cm
- F = lens power
The deviation of a light ray through prisms depends on not only the power of the prism but also the refractive index of the material it is made up of and the position in which the prism is held. Prisms can be held in three ways – position of minimum deviation, prentice position, and frontal position.[8]
- The position of minimum deviation is defined as the position in which the angle of incidence is equal to the angle of refraction. Plastic prisms are preferably used in the position of minimum deviation, but it is challenging to obtain this in clinical practice.
- Prentice position is defined as the position in which the prism is held perpendicular to the visual axis. This position is used for ophthalmic glass prisms.
- The frontal position is defined as the placement of prism parallel to the frontal plane of the patient.
Indications
The prisms are used in ophthalmology for diagnostic as well as therapeutic purposes. Prisms are made of glass or plastic material. These are available in different models such as loose prisms, prism bar, trial set prisms, or Fresnel prism. Prisms of different powers are available in different models. Prisms in a trial set range from ½ to 12 D. Prism bars range from 1 to 40 D. Fresnel prisms range from 1 to 40 D. Loose prisms range from 1 to 60 D.[11]
Diagnostic Indications
- Prisms are used in many ophthalmic devices such as slit lamp biomicroscope, applanation tonometer, gonioscope, keratometer, pupillometer, phoropter, ophthalmoscopes, operating microscope[12]
- Objective measurement of squint by prism cover test (Krimsky method), simultaneous prism cover test, modified Krimsky method[13]
- Subjective measurement of squint by Maddox rod[14]
- Measurement of fusional reserve amplitudes[15]
- Assessment of torsion[16]
- Four prism diopter test for microtropia[17]
- To detect abnormal retinal correspondence[18]
- To assess the likelihood of diplopia after proposed squint surgery[19]
- Prism adaptation test[20]
- To assess head posture after nystagmus surgery[21]
Therapeutic Indications
- Building up fusional reserve in patients with convergence insufficiency[22]
- Building up divergence capacity in patients with divergence insufficiency[23]
- To relieve diplopia in patients with small vertical squints, decompensated phorias, or paralytic squints to relieve diplopia in primary or reading positions.[24]
- To decrease the velocity of nystagmus by simulating convergence in nystagmus patients[25]
- To increase the field of vision in patients with hemianopia[26]
- Fresnel prisms are prescribed in patients with bitemporal hemianopia, glaucoma, retinitis pigmentosa, brain injury, and stroke[27]
- As for reading glasses for bedridden patients[28]
Contraindications
Though prisms have found a wide place in orthoptics' diagnostic and therapeutic world, there are no strict contraindications for prism prescription.[29] Still, we need to be careful about adaptation issues cost factors involved and check for suitability in the clinic before the final prescription. It is crucial to avoid or take extra precautions when prescribing prisms in the following situations.
- Prism adaptation – If prism adaptation occurs, there occurs an increase in underlying deviation and thus needs to be closely observed by the prescribing orthoptist.[30]
- If the underlying disease/mechanism causing original deviation is still progressive, the patient can adapt to the added prism and can redevelop the deviation.[31]
- If the prism is added continuously, the deviation might increase over time and become permanent.[32]
- Dragged fovea syndrome – In patients with pathology at the fovea like an epiretinal membrane, the patient's fovea might get displaced. This leads to a spatial disparity between the two foveae leading to central binocular diplopia. The prisms might reduce the central diplopia temporarily, but the diplopia reoccurs as the peripheral fusion takes over the central fusion.[33]
Equipment
Prisms used in ophthalmology are of different types. These include:
- Dispersive prisms – Abbes, triangular[34]
- Polarizing prisms – Nicol, Wollaston[35]
- Reflective prisms – Penta, Porro, Dove prisms[36]
Nicol Prisms
These are made up of calcite crystal cut diagonally, and the two halves are cemented with Canada balsam or an optical cement with a low refractive index. The incident light is split into ordinary and extra-ordinary linearly polarized rays. These prisms are used in Haidinger brushes.[37]
Wollaston Prisms
These two right-angled prisms composed of double refracting surfaces like quartz or calcite are cemented to form a rectangular unit. An incident beam of unpolarized light emerges as two oppositely polarized diverging beams from the opposite end. This type of prism is used in keratometers.[38]
Porro Prisms
This is a type of reflection prism used to alter the orientation of the image, i.e., the image traveling through the prism is rotated by 180 degrees. These prisms are used in slit lamps. The net effect of a beam passing through this prism is a parallel displaced image rotated by 180 degrees.[39]
The prisms used in orthoptics are available in different forms. These include:
- Loose prisms[40]
- Prisms in a trial frame
- Prism bar[41]
- Fresnel prisms[42]
- Rotating prisms[43]
- Risley double prisms–2 rotating prisms of the same strength on a rotating frame[44]
- Prism flippers[45]
- Vari prisms – prisms power can be changed by rotating two glasses[46]
Fresnel Prisms
These are made of polyvinyl chloride material. Parallel tiny prisms are stacked with an apex of one adjacent to the base of the previous prism, which can be struck on the base surface of the spectacles. This provides an overall prismatic effect of a single prism. The Fresnel prism is placed so that the base of prisms is directed towards the side of the defect.[29]
Personnel
The orthoptists, optometrists, and ophthalmologists are all actively involved and expected to understand the basics of prisms, the effects of prism in glasses, and the prismatic effect created by glass displacement in spectacles. After a detailed evaluation, it is essential to give the correct prescription and dispense the prisms with or without refractive correction.[47] There are two different notations used while ordering prisms.
One way to order prisms is by specifying the amount of prism required along with the direction of the prism's base. Example:
- Right - prism 3 UP 2out
- Left – prism 2 DN 2 out
An alternative method is to mention the direction of the prism using a 360-degree notation, where 0 is positioned towards the left of the lens, 90 superiorly, 180 right, and 270 inferiorly. So, the same prescription can be mentioned as:
- Right - prism 3 base 90 2 base 180
- Left – prism 2 base 270 2 base 0
Any refractive add for near or distance needs to be mentioned separately in the usual way of dispensing the spectacles.[48]
Preparation
While preparing glasses, it is essential to understand the prismatic effects of spherical lenses and Prentice's rule for prisms. The prismatic effect of the spherical lens is essential whenever the patient being evaluated has an underlying refractive error. A plus or a hyperopic lens behaves like two prism lenses stacked base to base.[49]
A minus or a myopic lens behaves like two prism lenses stacked apex to apex. Thus, the refractive correction affects the measured deviation and must be born in the mind. The measured deviation will be lesser with a plus lens and more when measured with a minus lens in situ.
Prentice's Rule
This law is named after a famous optician Charles F. Prentice. As per this rule, the prismatic power of the lens at any point on its surface equals the distance from its optical center, measured in centimeters multiplied by the power of the lens in diopters. There is no prismatic power at the center of the lens. Thus, it is vital that to avoid any prismatic effect, the lens's optical center should be fitted directly in front of the pupil.
Formula
Prismatic effect = power of the lens (DD) 'Distance off from the optic center in mm
Technique or Treatment
The technique of dispensing prisms depends on the disparity of single binocular vision. It is advisable to prescribe the smallest amount of relieving prism that neutralizes the distinction. The prism base should be oriented based on the deviation being corrected. The bottom of the prism is placed in the direction opposite to the deviation.[50]
The Direction of Prism in the Spectacles or for Neutralizing
|
S. No |
Deviation |
Right Eye |
Left Eye |
|
1 |
Exophoria/tropia |
Base in |
Base in
|
|
2 |
Esophoria/tropia
|
Base out |
Base out |
|
3 |
R/L Hyper |
Base-down |
Base-up
|
|
4 |
L/R Hyper |
Base-up |
Base-down
|
There are essential guidelines that need to be followed when considering the prescription of prism glasses to a patient. A few of the important ones include:
- Split the amount of correction equally between two eyes
- The base of the prism should be oriented opposite to the direction of the deviation of the eye
- Prisms of the range varying from 0.5D to 10D can be advised in patients with phoria.
- Both vertical or horizontal prisms can be prescribed individually or in combination in an oblique axis.
- Prisms of up to 6D can be tolerated in one eye and half in the other eye.
- Prisms can be prescribed in the form of glass prisms or Fresnel prisms stuck onto the glasses.[51]
Complications
Prisms are an effective way to relieve diplopia and improve vergence facilities. But some patients may experience side effects with prism glasses themselves.[51] A few fundamental problems associated with the use of prism glasses include:
- Headache
- Eyestrain
- Nausea/vomiting
- Double vision
- Confusion
- Deterioration of vision
Reasons for the discomfort experienced with prism correction glasses:
- Misalignment of lenses- There can be errors in the initial alignment of the axis or the optical center while fitting the prisms. Sometimes, they can get misaligned due to the regular use of prism correction glasses.
- Incorrect or expired prescription: A wrong or expired prescription for prism correction can lead to discomfort. It is essential to give the patient an adequate adaptation time in the clinic before providing the final prescription.
Clinical Significance
Optical Uses
Prisms are an essential part of ophthalmology. These are the basics behind many instruments used routinely in ophthalmic practice, from basic investigations to the outpatient department to the operating theatre.[52] Prims are part of ophthalmic instruments like slit lamp biomicroscope, applanation tonometer, gonioscope, keratometer, pupillometer, phoropter, Haidinger brushes, ophthalmoscopes, operating microscope.[53] In the sub-specialty of strabismus and neuro-ophthalmology, prisms find their role as part of diagnostic and therapeutic interventions.[54]
Prism Adaptation Test
This test is helpful in patients with partially accommodative esotropia. Patients wearing full hyperopic correction are advised to press on base out prisms and review every two weeks. If the esotropia has increased further, additional power prisms are prescribed till a stable angle is achieved. The surgeon then operates on the full prism-adapted angle; this helps in reducing the chances of under correction.[55]
Prism Alternate Cover Test
This test measures the total deviation, including the latent phoria. The first Hirschberg test estimates the tropia, followed by an alternate cover test to estimate the total deviation, i.e., tropia plus phoria. A prism of the estimated amount by an alternate cover test is placed over one eye to neutralize the deviation. An alternate cover test is repeated, and prism power increases or decreases until no refixation movement is noted.[56][57]
Simultaneous Prism Cover Test
This test helps in small-angle strabismus to measure the tropia without dissociating the phoria. The Hirschberg test measures the size of tropia, and a prism of the estimated amount is placed in front of the non-fixing eye to neutralize the tropia. The fixing eye is covered simultaneously with an occluder to prevent fusion. The process is repeated with increasing or decreasing prisms' powers until no refixation movement is noted on removing the occlude.[58]
Fusional Vergence Amplitudes
These are measured using a prism bar. Fusional convergence amplitudes are measured by placing the prism bar with the base in front of one eye in increasing steps until the patient reports double vision or inability to fuse. Similarly, fusional divergence amplitudes are measured with base in prism bar by increasing prism powers in steps till the patient reports double vision or failure to fuse.[59]
Vertical Prism Test
This test assesses fixation preference. A 10 to 15 D base up or down prism is placed over one eye, inducing vertical strabismus. For example, when a 12 D base-up prism is placed in front of the fixing eye, both the eyes will show an infraduction. But, when the same prism is placed in front of the non-fixating or the amblyopic eye, there will be no deviation of either eye.[60]
4D Prism Test
This test is used to diagnose microtropia.[17]
To Measure the AC/A Ratio
Prisms are used to measure the AC/A ratio by the fixation disparity method. Changes in fixation disparity induced by prisms and that induced by spherical lenses are noted, which indicates the AC/A ratio. The advantage is that fusion is maintained throughout the test.[61]
Prisms as Low Vision Aids
These are convex spherical lenses of powers ranging from +5 to +16D are prescribed as reading aids. These work on providing a magnified image, thus useful as low vision aids.[62]
Fresnel Prisms
These prisms have advantages over loose prisms as they are lighter, more comfortable to wear, cosmetically better acceptable by the patient, higher power can be prescribed compared to loose prisms.[42]
Field Expansion Lenses
They are composed of two 12 D lateral prisms and one 8D inferior prism. The apex of lenses is placed towards the central non-channel. The lens system is designed for various degrees of peripheral field loss. It is recommended for patients with glaucoma retinitis pigmentosa.[63]
Prisms in Age-Related Macular Degeneration (ARMD)
These are based on the principle of image relocation. Prisms are added to the glass prescription to produce image relocation to the presumed retinal locus. The effect is probably created by the facilitation of oculomotor function resulting from the reduction of fixation instability.[64]
Ankylosing Spondylitis
Patients with head or neck problems, such as severe ankylosing spondylitis, may benefit from prisms. For example, any patient with chin down posture bilateral equal power base up yoke prisms can improve straight-ahead vision and thus facilitate mobility.[65]
Prism as Reading Glasses
These are 15-30D base-down prisms in the form of recumbent spectacles, which allow bedridden patients to read or watch television comfortably in a lying-down position.[66]
Prisms in Nystagmus
Prisms are used to move the image towards the null point, thus helping by dampening the nystagmus. Examples include:
- Base out prisms stimulate fusional convergence, thus improving visual acuity by dampening the nystagmus
- In patients with left face turn, the null position is in dextroversion. Thus placing a base in prism in front of the right eye and base-out prism in front of the left eye will shift the image towards the right, thus correcting the abnormal head posture.
- Prisms in contact lens- prisms are used to stabilize the near vision portion in a segmental bifocal contact lens and stabilize a toric contact lens using prism ballast.[57]
Enhancing Healthcare Team Outcomes
The prescription of prisms is complex and requires expertise. Optometrists, orthoptics, and ophthalmologists need to work in coordination and understand the underlying pathology causing symptoms to treat it. Patients may present with complaints of headache, eye strain, or other asthenopic symptoms to anyone involved in eye healthcare. Thus it is essential to understand the basics for evaluation and prescription of prims.
The optometrists and orthoptists should check the fusional vergences in any patient complaining of asthenopic symptoms despite wearing correct refractive power. Vision therapy exercises should be prescribed to patients with any underlying fusional weakness. Patients complaining of double vision need a complete detailed evaluation by the ophthalmologist. Appropriate referrals should be made to a physician or neurologist to rule out underlying associations.
Systemic conditions like myasthenia gravis Graves disease can often present to the ophthalmologist first, and thus detailed examination and a high index of suspicion can lead to the correct diagnosis. Neurological lesions may present with gaze palsy, skew deviation, or internuclear ophthalmoplegia. Thus it is essential to evaluate the patient thoroughly and refer the patient to the radiologist for necessary investigations. Opinions from neurologists or neurosurgeons can be lifesaving in some emergency conditions, and a lower threshold should be used for the same.[3]
Nursing, Allied Health, and Interprofessional Team Monitoring
Patients prescribed with prisms need to be followed up closely for compliance. Those prescribed prisms for exercise might experience an initial exacerbation of asthenopic symptoms and thus require the motivation to continue the exercise till the fusional reserves improve. Patients might experience confusion and practical difficulties with the use of prisms. Therefore, it is essential to review them closely and attend to the patients' issues.
A few patients might show an increased angle of deviation with the prescribed prisms, and thus close monitoring is again vital in these cases. In patients presenting with long-standing palsies or partially accommodative esotropias, a decision might be taken to operate the residual squints. Thus, nurses and counselors need to motivate the patients and follow them closely after surgical intervention.[4]
Media
(Click Image to Enlarge)

Digital image depicting prism trial box containing prisms from 0.5 D to 50 D Contributed by Dr. Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS
(Click Image to Enlarge)
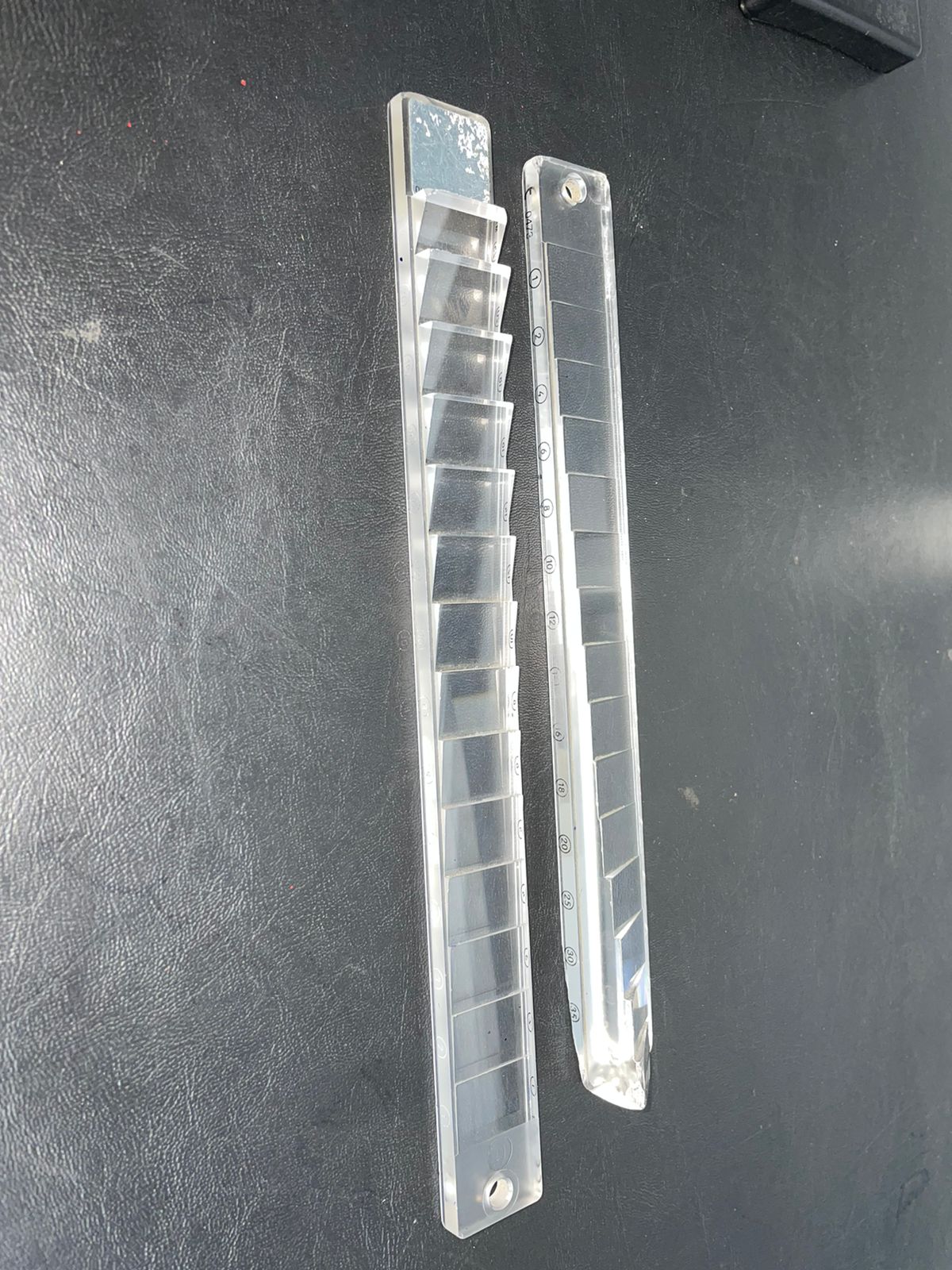
Digital image showing prism bars showing prisms of increasing power with base out and base down Contributed by Dr. Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS
(Click Image to Enlarge)

Digital image showing a Fresnel prism of power 40 PD Contributed by Dr. Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS
(Click Image to Enlarge)
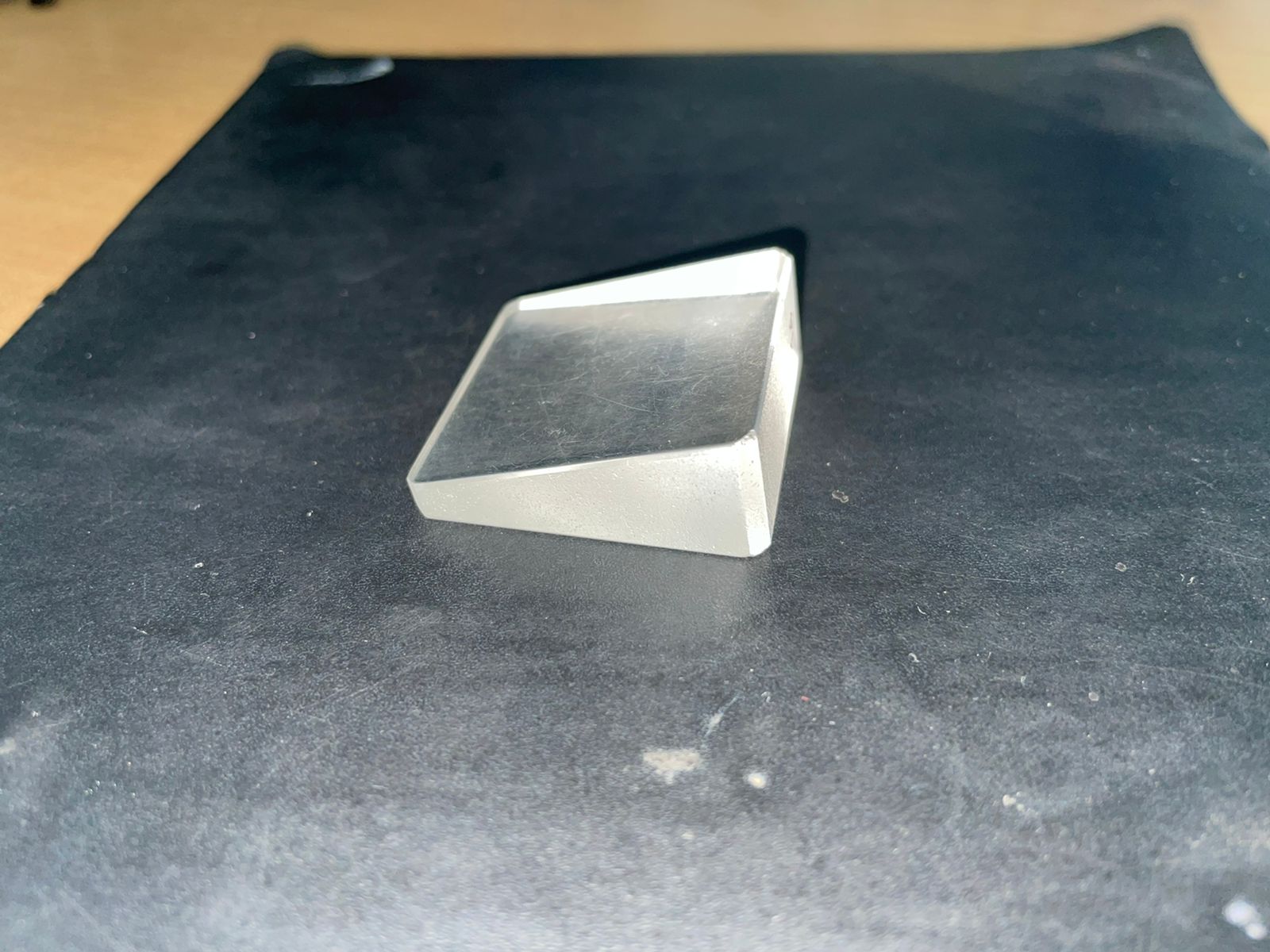
Digital image showing a loose prism of 40 PD Contributed by Dr. Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS
References
Peli E, Vargas-Martin F, Kurukuti NM, Jung JH. Multi-periscopic prism device for field expansion. Biomedical optics express. 2020 Sep 1:11(9):4872-4889. doi: 10.1364/BOE.399028. Epub 2020 Aug 5 [PubMed PMID: 33014587]
Gray LS. The prescribing of prisms in clinical practice. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2008 May:246(5):627-9. doi: 10.1007/s00417-008-0799-2. Epub 2008 Apr 1 [PubMed PMID: 18379815]
Irsch K. Optical Issues in Measuring Strabismus. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):265-70. doi: 10.4103/0974-9233.159691. Epub [PubMed PMID: 26180462]
Thompson JT, Guyton DL. Ophthalmic prisms. Deviant behavior at near. Ophthalmology. 1985 May:92(5):684-90 [PubMed PMID: 4011143]
Barry JC, Backes A. [Measuring the effect of eyeglasses on determination of squint angle with Purkinje reflexes and the prism cover test]. Klinische Monatsblatter fur Augenheilkunde. 1998 Apr:212(4):234-9 [PubMed PMID: 9644670]
Schechter RJ. Snell's Law: optimum pathway analysis. Survey of ophthalmology. 1977 May-Jun:21(6):464-6 [PubMed PMID: 898012]
Level 3 (low-level) evidenceThomas R, Braganza A, George T. Practical approach to diagnosis of strabismus. Indian journal of ophthalmology. 1996 Jun:44(2):103-12 [PubMed PMID: 8916600]
Hagen N, Tkaczyk TS. Compound prism design principles, I. Applied optics. 2011 Sep 1:50(25):4998-5011 [PubMed PMID: 22423145]
Hagen N, Tkaczyk TS. Compound prism design principles, III: linear-in-wavenumber and optical coherence tomography prisms. Applied optics. 2011 Sep 1:50(25):5023-5030 [PubMed PMID: 22423147]
Tang CY. Spherical lens decentration errors by Prentice's rule. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 1989 Jan:9(1):86-90 [PubMed PMID: 2594387]
Cossack M, Salini B. Prism Glasses. StatPearls. 2023 Jan:(): [PubMed PMID: 31082166]
Fairlamb MS, Whitaker AM, Bain FE, Spies M, Freudenthal BD. Construction of a Three-Color Prism-Based TIRF Microscope to Study the Interactions and Dynamics of Macromolecules. Biology. 2021 Jun 23:10(7):. doi: 10.3390/biology10070571. Epub 2021 Jun 23 [PubMed PMID: 34201434]
Joo KS, Koo H, Moon NJ. Measurement of strabismic angle using the distance Krimsky test. Korean journal of ophthalmology : KJO. 2013 Aug:27(4):276-81. doi: 10.3341/kjo.2013.27.4.276. Epub 2013 Jul 18 [PubMed PMID: 23908574]
Dolman P. The Maddox Rod Screen Test. Transactions of the American Ophthalmological Society. 1919:17():235-49 [PubMed PMID: 16692471]
Hatt SR, Leske DA, Mohney BG, Brodsky MC, Holmes JM. Fusional convergence in childhood intermittent exotropia. American journal of ophthalmology. 2011 Aug:152(2):314-9. doi: 10.1016/j.ajo.2011.01.042. Epub 2011 May 31 [PubMed PMID: 21621744]
Level 2 (mid-level) evidenceFelius J, Locke KG, Hussein MA, Stager DR Jr, Stager DR Sr. Photographic assessment of changes in torsional strabismus. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2009 Dec:13(6):593-5. doi: 10.1016/j.jaapos.2009.09.008. Epub [PubMed PMID: 20006824]
Frantz KA, Cotter SA, Wick B. Re-evaluation of the four prism diopter base-out test. Optometry and vision science : official publication of the American Academy of Optometry. 1992 Oct:69(10):777-86 [PubMed PMID: 1436999]
Porter A. A simple method of detecting abnormal retinal correspondence. The British journal of ophthalmology. 1979 May:63(5):353-4 [PubMed PMID: 465411]
Level 3 (low-level) evidenceWang JY, Leske DA, Hatt SR, Holmes JM. Diplopia after strabismus surgery for adults with nondiplopic childhood-onset strabismus. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2019 Dec:23(6):313.e1-313.e5. doi: 10.1016/j.jaapos.2019.07.005. Epub 2019 Oct 3 [PubMed PMID: 31586582]
Akbari MR, Mehrabi Bahar MR, Mirmohammadsadeghi A, Bayat R, Masoumi A. Short prism adaptation test in patients with acquired nonaccommodative esotropia; clinical findings and surgical outcome. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2018 Oct:22(5):352-355. doi: 10.1016/j.jaapos.2018.05.018. Epub 2018 Sep 15 [PubMed PMID: 30227245]
Lee J. Surgical management of nystagmus. Journal of the Royal Society of Medicine. 2002 May:95(5):238-41 [PubMed PMID: 11983764]
Hashemi H, Nabovati P, Khabazkhoob M, Yekta A, Ostadimoghaddam H, Doostdar A, Ramin S, Aghamirsalim M. The Prevalence of Fusional Vergence Dysfunction in a Population in Iran. Journal of current ophthalmology. 2021 Apr-Jun:33(2):112-117. doi: 10.4103/JOCO.JOCO_61_20. Epub 2021 Jul 5 [PubMed PMID: 34409219]
Pineles SL. Divergence Insufficiency Esotropia: Surgical Treatment. The American orthoptic journal. 2015:65():35-9. doi: 10.3368/aoj.65.1.35. Epub [PubMed PMID: 26564924]
Iliescu DA, Timaru CM, Alexe N, Gosav E, De Simone A, Batras M, Stefan C. Management of diplopia. Romanian journal of ophthalmology. 2017 Jul-Sep:61(3):166-170 [PubMed PMID: 29450393]
Abadi RV. Mechanisms underlying nystagmus. Journal of the Royal Society of Medicine. 2002 May:95(5):231-4 [PubMed PMID: 11983762]
Goodwin D. Homonymous hemianopia: challenges and solutions. Clinical ophthalmology (Auckland, N.Z.). 2014:8():1919-27. doi: 10.2147/OPTH.S59452. Epub 2014 Sep 22 [PubMed PMID: 25284978]
Peli E. 2017 Charles F. Prentice Award Lecture: Peripheral Prisms for Visual Field Expansion: A Translational Journey. Optometry and vision science : official publication of the American Academy of Optometry. 2020 Oct:97(10):833-846. doi: 10.1097/OPX.0000000000001590. Epub [PubMed PMID: 33055514]
Krause HK. [Pitfalls in the prescription of reading glasses]. Der Ophthalmologe : Zeitschrift der Deutschen Ophthalmologischen Gesellschaft. 2011 Apr:108(4):324-30. doi: 10.1007/s00347-011-2343-8. Epub [PubMed PMID: 21505967]
Haller T, Furr BA. Fresnel prism use among orthoptists. The American orthoptic journal. 2014:64():71-5. doi: 10.3368/aoj.64.1.71. Epub [PubMed PMID: 25313114]
Gietzelt C, Fricke J, Neugebauer A, Hedergott A. Prism adaptation test before strabismus surgery in patients with decompensated esophoria and decompensated microesotropia. International ophthalmology. 2022 Jul:42(7):2195-2204. doi: 10.1007/s10792-022-02219-3. Epub 2022 Jan 17 [PubMed PMID: 35038124]
Alvarez TL, Kim EH, Granger-Donetti B. Adaptation to Progressive Additive Lenses: Potential Factors to Consider. Scientific reports. 2017 May 31:7(1):2529. doi: 10.1038/s41598-017-02851-5. Epub 2017 May 31 [PubMed PMID: 28566706]
Tamhankar MA, Ying GS, Volpe NJ. Success of prisms in the management of diplopia due to fourth nerve palsy. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2011 Sep:31(3):206-9. doi: 10.1097/WNO.0b013e318211daa9. Epub [PubMed PMID: 21378578]
Level 2 (mid-level) evidenceDe Pool ME, Campbell JP, Broome SO, Guyton DL. The dragged-fovea diplopia syndrome: clinical characteristics, diagnosis, and treatment. Ophthalmology. 2005 Aug:112(8):1455-62 [PubMed PMID: 15953644]
Level 2 (mid-level) evidenceEsfahlani H, Karkar S, Lissek H, Mosig JR. Acoustic dispersive prism. Scientific reports. 2016 Jan 7:6():18911. doi: 10.1038/srep18911. Epub 2016 Jan 7 [PubMed PMID: 26739504]
Wang ZP, Sun WM, Ruan SL, Kang C, Huang ZJ, Zhang SQ. Polarization-preserving totally reflecting prisms with a single medium layer. Applied optics. 1997 May 1:36(13):2802-6 [PubMed PMID: 18253275]
Schonbrun E, Abashin M, Blair J, Wu Q, Park W, Fainman Y, Summers CJ. Total internal reflection photonic crystal prism. Optics express. 2007 Jun 25:15(13):8065-75 [PubMed PMID: 19547134]
Simon MC, Echarri RM. Internal total reflection in monoaxial crystals. Applied optics. 1987 Sep 15:26(18):3878-83. doi: 10.1364/AO.26.003878. Epub [PubMed PMID: 20490157]
Montarou CC, Gaylord TK. Analysis and design of modified Wollaston prisms. Applied optics. 1999 Nov 1:38(31):6604-16 [PubMed PMID: 18324196]
Liu YD, Gao C, Qi X. Field rotation and polarization properties of the Porro prism. Journal of the Optical Society of America. A, Optics, image science, and vision. 2009 May:26(5):1157-60 [PubMed PMID: 19412232]
Level 2 (mid-level) evidenceWessels IF, Thomas S, Wessels DA. Hook and loop fastener on loose prisms assists in measuring ocular deviation. Ophthalmic surgery and lasers. 1998 Sep:29(9):774-7 [PubMed PMID: 9760618]
Level 2 (mid-level) evidenceKaye SB, Ansons AM, Green JR, Wylie J. The prism bar--Prentice and frontal positions. Eye (London, England). 1989:3 ( Pt 4)():404-8 [PubMed PMID: 2606213]
Véronneau-Troutman S. Fresnel prisms and their effects on visual acuity and binocularity. Transactions of the American Ophthalmological Society. 1978:76():610-53 [PubMed PMID: 754384]
Level 3 (low-level) evidenceWaddell JH. Rotating prism design for continuous image compensation cameras. Applied optics. 1966 Jul 1:5(7):1211-23. doi: 10.1364/AO.5.001211. Epub [PubMed PMID: 20049049]
Zhao Y, Yuan Y. First-order approximation error analysis of Risley-prism-based beam directing system. Applied optics. 2014 Dec 1:53(34):8020-31. doi: 10.1364/AO.53.008020. Epub [PubMed PMID: 25607958]
Santos EM, Yaramothu C, Alvarez TL. Comparison of symmetrical prism adaptation to asymmetrical prism adaptation in those with normal binocular vision. Vision research. 2018 Aug:149():59-65. doi: 10.1016/j.visres.2018.06.004. Epub 2018 Jun 28 [PubMed PMID: 29940191]
Jung JH, Peli E. Impact of high power and angle of incidence on prism corrections for visual field loss. Optical engineering (Redondo Beach, Calif.). 2014 Jan 17:53(6):. doi: 10.1117/1.OE.53.6.061707. Epub [PubMed PMID: 24497649]
Schroth V, Joos R, Jaschinski W. Effects of Prism Eyeglasses on Objective and Subjective Fixation Disparity. PloS one. 2015:10(10):e0138871. doi: 10.1371/journal.pone.0138871. Epub 2015 Oct 2 [PubMed PMID: 26431525]
du Toit R. How to prescribe spectacles for presbyopia. Community eye health. 2006 Mar:19(57):12-3 [PubMed PMID: 17491738]
Waddell K. Spherical refraction for general eye workers. Community eye health. 2000:13(33):6-7 [PubMed PMID: 17491944]
Schroth V, Joos R, Alshuth E, Jaschinski W. Effects of aligning prisms on the objective and subjective fixation disparity in far distance. Journal of eye movement research. 2019 Dec 11:12(4):. doi: 10.16910/jemr.12.4.8. Epub 2019 Dec 11 [PubMed PMID: 33828739]
Giorgi RG, Woods RL, Peli E. Clinical and laboratory evaluation of peripheral prism glasses for hemianopia. Optometry and vision science : official publication of the American Academy of Optometry. 2009 May:86(5):492-502. doi: 10.1097/OPX.0b013e31819f9e4d. Epub [PubMed PMID: 19357552]
Lee SH, Jun W, London R. Optical Management Using Monovision and Yoked Prism for Acquired Strabismus and Nystagmus Secondary to a Neurodegenerative Disease. Neuro-ophthalmology (Aeolus Press). 2015 Jun:39(3):147-151 [PubMed PMID: 27928348]
Peli E, Bowers AR, Keeney K, Jung JH. High-Power Prismatic Devices for Oblique Peripheral Prisms. Optometry and vision science : official publication of the American Academy of Optometry. 2016 May:93(5):521-33. doi: 10.1097/OPX.0000000000000820. Epub [PubMed PMID: 26866438]
Saxena R, Singh D, Jethani J, Sharma P, Sinha R, Sharma N, Sachdev Writing Committee MS, Prepared in Association with the AIOS Pediatric and. Pediatric ophthalmology, strabismus and neuro-ophthalmology practice in the COVID-19 era: All India Ophthalmological Society guidelines. Indian journal of ophthalmology. 2020 Jul:68(7):1300-1305. doi: 10.4103/ijo.IJO_1789_20. Epub [PubMed PMID: 32587154]
Choe HR, Yang HK, Hwang JM. Long-term outcomes of prismatic correction in partially accommodative esotropia. PloS one. 2019:14(12):e0225654. doi: 10.1371/journal.pone.0225654. Epub 2019 Dec 2 [PubMed PMID: 31790473]
Hull S, Tailor V, Balduzzi S, Rahi J, Schmucker C, Virgili G, Dahlmann-Noor A. Tests for detecting strabismus in children aged 1 to 6 years in the community. The Cochrane database of systematic reviews. 2017 Nov 6:11(11):CD011221. doi: 10.1002/14651858.CD011221.pub2. Epub 2017 Nov 6 [PubMed PMID: 29105728]
Level 1 (high-level) evidenceBaranowska-George T. [The effect of treatment with prisms on head position in persons with nystagmus--preliminary report]. Klinika oczna. 1996 Mar:98(3):195-6 [PubMed PMID: 9019587]
Deacon MA, Gibson F. Strabismus measurements using the alternating and simultaneous prism cover tests: a comparative study. Journal of pediatric ophthalmology and strabismus. 2001 Sep-Oct:38(5):267-72 [PubMed PMID: 11587174]
Level 2 (mid-level) evidenceFray KJ. Fusional amplitudes: exploring where fusion falters. The American orthoptic journal. 2013:63():41-54. doi: 10.3368/aoj.63.1.41. Epub [PubMed PMID: 24141750]
Level 1 (high-level) evidenceGolnik KC, Lee AG, Eggenberger ER. The monocular vertical prism dissociation test. American journal of ophthalmology. 2004 Jan:137(1):135-7 [PubMed PMID: 14700656]
Murray C MRes, BSc HONS, Newsham D PhD, MSc, DBO. The Normal Accommodative Convergence/Accommodation (AC/A) Ratio. Journal of binocular vision and ocular motility. 2018 Oct-Dec:68(4):140-147. doi: 10.1080/2576117X.2018.1529450. Epub 2018 Oct 25 [PubMed PMID: 30358493]
Agarwal R, Tripathi A. Current Modalities for Low Vision Rehabilitation. Cureus. 2021 Jul:13(7):e16561. doi: 10.7759/cureus.16561. Epub 2021 Jul 22 [PubMed PMID: 34466307]
Apfelbaum H, Peli E. Tunnel Vision Prismatic Field Expansion: Challenges and Requirements. Translational vision science & technology. 2015 Dec:4(6):8 [PubMed PMID: 26740910]
Al-Karmi R, Markowitz SN. Image relocation with prisms in patients with age-related macular degeneration. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2006 Jun:41(3):313-8 [PubMed PMID: 16767185]
Level 2 (mid-level) evidenceGarcia-Montoya L, Gul H, Emery P. Recent advances in ankylosing spondylitis: understanding the disease and management. F1000Research. 2018:7():. pii: F1000 Faculty Rev-1512. doi: 10.12688/f1000research.14956.1. Epub 2018 Sep 21 [PubMed PMID: 30345001]
Level 3 (low-level) evidenceScheiman M, Cotter S, Rouse M, Mitchell GL, Kulp M, Cooper J, Borsting E, Convergence Insufficiency Treatment Trial Study Group. Randomised clinical trial of the effectiveness of base-in prism reading glasses versus placebo reading glasses for symptomatic convergence insufficiency in children. The British journal of ophthalmology. 2005 Oct:89(10):1318-23 [PubMed PMID: 16170124]
Level 1 (high-level) evidence