Introduction
Contrast sensitivity (CS) is the ability to perceive sharp and clear outlines of very small objects.[1] It is also defined as the ability to perceive minor illuminance changes between interspersed regions not separated by defined borders. Snellen’s test types help in only perceiving sharp and clear outlines of very small objects and not the changes in illuminance.[2]
A patient can have 20/20 visual acuity in many ocular diseases with loss of CS. Sometimes the loss of CS can be more psychologically disturbing than the loss of visual acuity.[3] Schade first measured CS by using the modulation transfer function. Contrast sensitivity using sinusoidal grating was first measured in 1968 by Campbell and Green, and they concluded that it is a complex and discrete function of the retina.[4]
Contrast can be defined as the degree of blackness to the whiteness of a particular object or a target. The contrast threshold is the minimum contrast required to perceive an object clearly.[5] CS is also the reciprocal of the contrast threshold. The various types of CS are spatial and temporal. CS can be measured by Arden grating, Cambridge low contrast grating, Pelli-Robson CS chart, Bailey Lovie chart, vision contrast test system (VCTS), Vistech chart, Regan chart, and FACT chart.[6]
CS varies with the luminance, target, grating motion, and grating shape. Neural mechanism and channel theory have more profound insights into the mechanism of CS. The factors which affect CS are refractive error, age, cataract surgery, refractive surgery, glaucoma, diabetic retinopathy, optic neuropathy, pituitary adenoma, etc. This activity deals with the pathophysiology, indications, types, factors affecting, methods of measuring, and clinical implications of CS.[7]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Neural Mechanisms
Campbell and Green defined the neural mechanism for CS. They proposed different visual channels for handling the information about various bands of spatial frequencies.[8] This indicates that the retina is non-uniform. The fovea is the part of the retina specialized for high spatial frequencies. Only low-frequency channels represent the retinal periphery.[9]
For coarse gratings, the central and peripheral retina has equal contrast sensitivity per unit area of the retina, but the more the area stimulated greater the CS. In peripheral retinal diseases, the CS is reduced, and low-frequency grating use help to provide a quick check of peripheral retinal function.[10]
Campbell and Robson proposed that independent mechanisms in the nervous system exist that are highly sensitive to a limited range of spatial frequencies. There is selective orientation and transfer of interocular adaptation effect in the visual cortex at the site of neurons. This helped explain the vital role of these interactions in complex image recognition and magnification generalization.[11]
M and P Pathways
The ganglion cells are subdivided into
- P cells- These cells have a high spatial resolution
- p cells- These cells are small and slow conducting cells that give input to the parvocellular layer of the lateral geniculate body.
- M cells- These cells have higher CS and temporal resolution and lower spatial resolution.
- m cells- These are large and flat conducting axons that provide input to the magnocellular layers[12]
Channel Theory
The cerebrospinal fluid (CSF) is susceptible to particular spatial frequency and is a function of several independent and parallel detecting mechanisms. The visual system is split up into several spatial frequency components separately, and the information is further transmitted into various channels in the cortex, where it is transformed.[13]
The visual system is composed of 4 to 6 spatial frequency channels. The CSF channels depend on a series of ganglion cells with varied receptive fields so that they have maximum sensitivity to various spatial frequencies. A partial response is obtained from the ganglion cells when the stimulus size is smaller than the central receptive field. When the stimulus size is larger than the central receptive field, the response from the ganglion cells is reduced.[14]
Indications
- People applying for jobs like armed forces, driving, pilots, merchant navy, lab technicians, medical professionals, etc
- People opting for athletics as a career
- Qualitative vision loss
- Retinal or optic nerve disease
- Visual pathway diseases
- Glaucoma
- Ocular hypertension
- Retrobulbar neuritis
- Multiple sclerosis
- Amblyopia
- Diabetes mellitus
- Pituitary adenoma
- Congenital dyschromatopsia
- Optic neuritis
- Cataract
- Higher-order aberrations
- Age-Related Macular Degeneration
- Trauma
- LASIK
- PRK
Equipment
Contrast Sensitivity Measurement
When the grating frequency is presented to the subject, and the contrast below is resolution is not possible, it denotes the contrast threshold, and the reciprocal of this threshold is CS.[15]
The formula for CS measurement-
Michelson’s Formula
(L– L)/ (L+ L) where L denotes the luminance of the photocells scanning across the gratings. Lis the luminance on the lighter surface, and Lis the luminance on the darker surface.[16]
Weber’s Formula
It is defined as (LL)/ L, where b is the background luminance and t is the target luminance. This formula is used to measure the contrast of the letters.[17]
Variables in CS measurement
- The average amount of reflected light depends on the darkness of ink and the illumination of paper.
- The amount of darkness relative to the white background is labeled as a contrast.
- The distance between the cycles per degree of visual angle or grating period.[18]
Methods of Contrast Sensitivity Measurement
Various methods have been described for CS measurement. Bodis Wollner described the CS measurements in day-to-day clinical practice. This was labeled as a visuogram to describe the CS curve. The CS deficit is expressed in decibels, and there are three types of deficits.
- High frequency- which is characterized by an increased loss at high frequency
- Level loss type- same loss at all kinds of spatial frequencies
- Selective loss type- Spatial frequency deficits in a narrow band
Various Recommended Methods for Contrast Sensitivity Measurement
- Simple plates
- Cathode ray tube display
- Letter acuity charts
- Laser interferometer (LI)
- Visual field testing using low contrast rings
- Pattern discrimination test
- Forced choice printed test
- Visual evoked cortical potentials
- Checkerboard pattern reversal
- Two alternative forced-choice tests[19]
Arden Gratings
In 1978, Arden introduced a booklet of seven plates having one screening plate (No.1) and six diagnostic plates (No. 2 to 7). The contrast changes from top to bottom plates, and it covers 1.76 log units approximately. The patient is examined with the plates at a distance of 57 cm with a spatial frequency varying from 0.2 cycles/degree to 6.4 cycles/degree having a double frequency of the previous one. The patient is scored from 1 to 20 depending on the number of the plate covered. The upper limit of 82 is established for normal subjects, consisting of six plates having an interocular difference of less than 12.
Cambridge Low Contrast Gratings
It has a set of ten plates consisting of grating in a spiral-bound booklet. The test is performed at a distance of 6 meters with the booklet hung on the wall. The pages are shown in pairs, one above the other. It shows that one page in each pair has gratings and another page is blank, but the mean reflectance of the pages is the same. The test subject is asked to choose the pages from the top or bottom containing gratings. The pages are shown to the subjects in order of descending contrast, and are subject is stopped when the first error is made. A total of four descending series are shown in each eye separately. When an error is made on plate 5, a score of 6 is given. Depending on the total score from the four series, the CS is calculated from the conversion plate.[20]
Pelli- Robson Contrast Sensitivity Chart
This chart has letters that subtend an angle of 3 degrees at a distance of 1 meter. The chart is printed on both sides; the other side has letter sequences in a different order. The letters are arranged in a series of two triplets in each line. The contrast reduces from one triplet to the next. The log sensitivity also varies from 0 to 2.25. While examining the patient, the chart can be hung on the wall so that the chart’s center coincides with the patient’s eye. The chart is brightly illuminated so that the luminance varies from 60 and 120 cd/m, which is equal to the exposure of 1/15 to 1/30 s at f/5.6 with an ASA of 100.
The luminance is recorded with the assistance of a light meter. While recording CS with the chart, the patient is seated at a distance of 1 meter. The subject is asked to read or point out the letter on the chart, beginning from the upper left corner and going horizontally across the line. The patient can also guess when the letters are invisible. The test is terminated if the patient wrongly guesses two out of three letters. The patient’s CS is indicated by the best triplets, for which two out of three letters are named correct.[21]
Mars Letter Contrast Sensitivity Test
This chart looks similar to the Pelli-Robson test, but the chart is comparatively smaller and is viewed at a closer distance.[22]
Vistech Chart
This consists of sine-wave gratings and is conducted at a distance of 3 meters from the patient. In this, the contrast is tested at several spatial frequencies, and the patient has to pinpoint the orientation of the grating, either vertical or 15 degrees or anticlockwise.
Functional Acuity Contrast Testing
Dr. Arthur Ginsburg first described functional Acuity Contrast Testing (FACT). This includes a chart of sine-wave grating with varying frequencies. With the help of this chart, five spatial frequencies and nine levels of contrast can be tested. The contrast of the letter change in the row and decreases from left to right. The spatial frequency increases from top to bottom, and the test is performed at a distance of 10 feet. The patient sees the grating in each row like A, B, C, and D and then reports the orientation right, up, or left. The last grating for each spatial frequency is then plotted for the CS curve.[23]
Regan Low Contrast Sensitivity Letter Charts
This consists of three-letter charts printed on white cardboard, having a contrast of 97%, 7%, and 4%. It is tested at 3 meters with eight letters in each line. The patient is told to start from the top of the row until they can no longer identify the letter on the line. The letter size goes on reducing, and the contrast remains the same. Regan, in 1988 said that this has a role in detecting early vision loss in glaucoma and diabetes.[24]
Spaeth Richman Contrast Sensitivity Test
Spaeth Richman contrast sensitivity test (SPARCS) is a computerized test to assess CS. It can be accessed online with good internet access. The patient being tested is provided an identification number and instructed regarding the test. The test can be performed in 5 to 10 minutes for each eye and measures the central and peripheral CS. This test can also be employed in illiterate patients as this is based on gratings.[25]
Personnel
The paramedical staff, the mid-level ophthalmic personnel, the optometrist, or the refractionist trained in CS assessment can help test the subjects. CS is measured by log contrast. The lesser the score, the poorer the CS.
- A score of 2 means normal CS
- A score less than 1.5 indicates visual impairment
- A score of less than 1 indicates a visual disability[26]
Types of Contrast Sensitivity
Spatial
It refers to obtaining the striped pattern, which is detected at various levels of contrast and spatial frequencies. The spatial frequency is measured with the help of (Arden gratings) in which the patient is shown sine wave grating having parallel light and dark bands, and they are asked to tell the minimum level of contrast at which the bars are seen. The width of the bars is essential as it defines the spatial frequency, which denotes pairs of dark and light bars that subtend an angle of 1 degree at the eye. If the spatial frequency is high, it denotes narrow bars, and if it is low, it indicates wide bars.[27]
Temporal
Here CS is a function of time rather than spatial position. It is a time-oriented (temporal) processing in the visual system by exhibiting a uniform target field modulation sinusoidal in time.[28]
Technique or Treatment
Snellen’s Test Types Versus Contrast Sensitivity
The visual acuity tested by Snellen’s test types is of very high contrast, but in a real-world scenario, the patient may be visually handicapped due to loss of CS. In conditions with low contrast, the visual acuity becomes reduced, and the quality of vision is also reduced. The CS is considered a better predictor of visual acuity as it provides information not provided by the visual acuity alone.[29]
Contrast Sensitivity Curve
The contrast sensitivity can also be plotted as a curve, with the x-axis having a spatial frequency and the y-axis having contrast sensitivity.[30]
Contrast Sensitivity Function
Manos and Sakrison first proposed this. The graph of CS over spatial frequency range gives CS function. CS is a function of spatial frequency, denoted in cycles per degree; this is a subjective measurement of a subject’s ability to detect a low contrast stimulus, usually vertical stripes of reducing shades of black to grey. This measurement should give a more accurate representation of the eye’s visual function. The peak value range from 1 to 8 cycles/ degree, and the high frequencies are not distinguished due to a limited number of photoreceptors. Neural and optical mechanisms limit the higher spatial CS.[31]
Modulation Transfer Function
This indicates the ability of the optical system to transform minute details (spatial frequencies) from object to image. The units are denoted by the ratio of image contrast over object contrast, a function of spatial frequency. MTF is the optical component of the CS function.[32]
Gratings
There are a series of pairs of light and dark bars in this. One adjacent pair make up one cycle. The thickness is denoted by spatial frequency in cycle per degree of the visual angle of the eye. Many gratings can be accommodated within a degree of visual angle. They are broader with low spatial frequencies. The spatial phase describes the position. A change in spatial phase by 180 degrees denotes that the grating is displaced by a half cycle.[33]
Sine Wave Gratings
These lack a sharp outline, and sinusoidal grating is preferred because they are free from defocus, light scatter, aberration and diffraction. It affects only the contrast and spatial positions.[34]
Square Wave Gratings
These grating have sharp edges.[35]
Clinical Significance
Patients with CS loss can have glare and halos during the night and may need extra illumination to read an object. After straining, the eyes may have congestion; the eyes may not be able to see clothes, dishes, and small objects. The patients may not be able to notice facial gestures.
The clinical significance of CS is governed by the factors which affect the CS.
- Refractive errors - Low spatial frequencies are not affected; only high spatial frequencies are affected by refractive error.
- Cataract - Early cataract reduces CS for low spatial frequencies; this is not related to visual acuity. Brannan et al., in their analysis, found that CS reduced from 37% to 19% within six months of performing the cataract surgery.
- Age - The CS decreases with age. After the second decade, it has been documented that CS scores decline by 10% each decade. The average decline is equal to the CS range within the normal population at any age.
- Systemic disease - Contrast sensitivity is reduced in several systemic diseases listed above.[36]
Diagnostic Applications
Contrast sensitivity is labeled as a diagnostic indicator of visual function. It is reduced in various ocular and systemic conditions, as listed above. It is also known that CS (modulation transfer function) is a complete statement for the relationship between spatial frequency and visual field intricacies, the contrast needed for resolution, and stimulus luminance. The use of yellow-tinted glasses helps in improving CS. These glasses increase the sharpness perception during the daytime. These should be avoided while driving to prevent glare, and anti-reflective coating glasses can be used to reduce glare. Yellow or copper tinted lenses help improve contrast and working environment in low ambient light.[37]
Enhancing Healthcare Team Outcomes
When patients present to the outpatient department with diminished or blurred vision, they should be examined in detail to pinpoint the pathology. A reduced CS should be suspected if the patient complains of reduced visual acuity despite 20/20 vision. The optometrist plays a crucial role in assessing the contrast sensitivity of the subject with the available charts. The examining ophthalmology should also keep a high suspicion of reduced CS in these cases. In case of reduced CS, the patient should be counseled well regarding the ocular condition and all symptoms the patient can have during nighttime. The patient should be explained the prognosis based on the ocular pathology.[38]
Nursing, Allied Health, and Interprofessional Team Interventions
The nursing and allied staff help examine the patient with CS charts, explaining the prognosis and nature of underlying pathology.
Media
(Click Image to Enlarge)
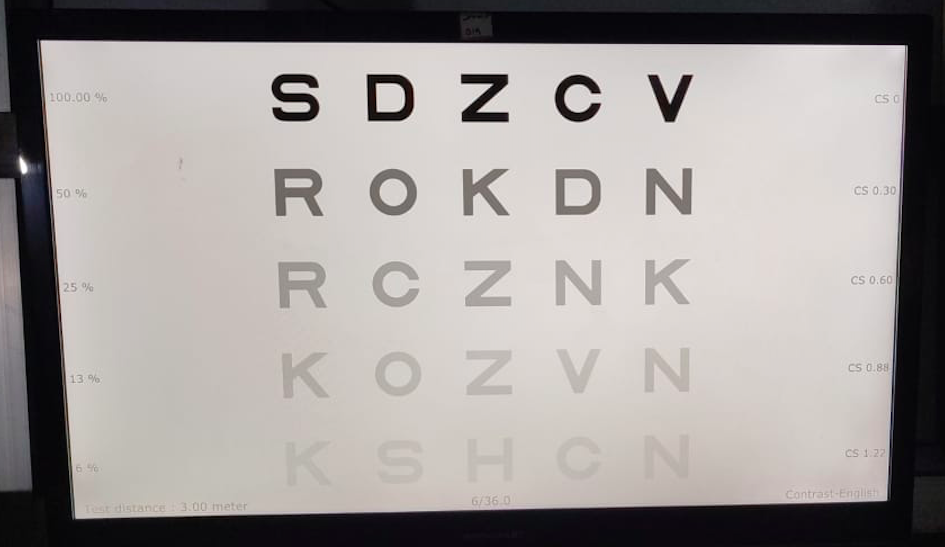
Digital image depicting Pelli-Robson contrast sensitivity chart Contributed by Dr Kirandeep Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS
References
Stalin A, Dalton K. Relationship of Contrast Sensitivity Measured Using Quick Contrast Sensitivity Function With Other Visual Functions in a Low Vision Population. Investigative ophthalmology & visual science. 2020 Jun 3:61(6):21. doi: 10.1167/iovs.61.6.21. Epub [PubMed PMID: 32516407]
Tidbury LP, Czanner G, Newsham D. Fiat Lux: the effect of illuminance on acuity testing. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2016 Jun:254(6):1091-7. doi: 10.1007/s00417-016-3329-7. Epub 2016 Apr 22 [PubMed PMID: 27106623]
Sabel BA, Wang J, Cárdenas-Morales L, Faiq M, Heim C. Mental stress as consequence and cause of vision loss: the dawn of psychosomatic ophthalmology for preventive and personalized medicine. The EPMA journal. 2018 Jun:9(2):133-160. doi: 10.1007/s13167-018-0136-8. Epub 2018 May 9 [PubMed PMID: 29896314]
Leroux CE, Bouchet E, Espinasse P, Fontvieille C, Bardin F. Correlation between Contrast Sensitivity and Modulation Transfer Functions. Optometry and vision science : official publication of the American Academy of Optometry. 2021 Nov 1:98(11):1263-1269. doi: 10.1097/OPX.0000000000001795. Epub [PubMed PMID: 34510142]
O'Carroll DC, Wiederman SD. Contrast sensitivity and the detection of moving patterns and features. Philosophical transactions of the Royal Society of London. Series B, Biological sciences. 2014:369(1636):20130043. doi: 10.1098/rstb.2013.0043. Epub 2014 Jan 6 [PubMed PMID: 24395970]
Level 3 (low-level) evidencePesudovs K, Hazel CA, Doran RM, Elliott DB. The usefulness of Vistech and FACT contrast sensitivity charts for cataract and refractive surgery outcomes research. The British journal of ophthalmology. 2004 Jan:88(1):11-6 [PubMed PMID: 14693761]
Tahir HJ, Parry NR, Brahma A, Ikram K, Murray IJ. The importance of grating orientation in contrast sensitivity following refractive surgery. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2009 Sep:29(5):518-25. doi: 10.1111/j.1475-1313.2009.00676.x. Epub [PubMed PMID: 19689547]
McMahon MJ, Lankheet MJ, Lennie P, Williams DR. Fine structure of parvocellular receptive fields in the primate fovea revealed by laser interferometry. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2000 Mar 1:20(5):2043-53 [PubMed PMID: 10684905]
Level 3 (low-level) evidenceHaun AM. What is visible across the visual field? Neuroscience of consciousness. 2021:2021(1):niab006. doi: 10.1093/nc/niab006. Epub 2021 Jun 1 [PubMed PMID: 34084558]
Anderson RS, Zlatkova MB, Beirne RO. The contrast sensitivity function for detection and resolution of blue-on-yellow gratings in foveal and peripheral vision. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2002 Sep:22(5):420-6 [PubMed PMID: 12358313]
Blakemore C, Campbell FW. On the existence of neurones in the human visual system selectively sensitive to the orientation and size of retinal images. The Journal of physiology. 1969 Jul:203(1):237-60 [PubMed PMID: 5821879]
Solomon SG. Retinal ganglion cells and the magnocellular, parvocellular, and koniocellular subcortical visual pathways from the eye to the brain. Handbook of clinical neurology. 2021:178():31-50. doi: 10.1016/B978-0-12-821377-3.00018-0. Epub [PubMed PMID: 33832683]
Olstad EW, Ringers C, Hansen JN, Wens A, Brandt C, Wachten D, Yaksi E, Jurisch-Yaksi N. Ciliary Beating Compartmentalizes Cerebrospinal Fluid Flow in the Brain and Regulates Ventricular Development. Current biology : CB. 2019 Jan 21:29(2):229-241.e6. doi: 10.1016/j.cub.2018.11.059. Epub 2019 Jan 3 [PubMed PMID: 30612902]
Reinhard K, Münch TA. Visual properties of human retinal ganglion cells. PloS one. 2021:16(2):e0246952. doi: 10.1371/journal.pone.0246952. Epub 2021 Feb 16 [PubMed PMID: 33592045]
Howell ER, Mitchell DE, Keith CG. Contrast thresholds for sine gratings of children with amblyopia. Investigative ophthalmology & visual science. 1983 Jun:24(6):782-7 [PubMed PMID: 6853106]
Wang YC, Shyu LH, Chang CP. The comparison of environmental effects on michelson and fabry-perot interferometers utilized for the displacement measurement. Sensors (Basel, Switzerland). 2010:10(4):2577-86. doi: 10.3390/s100402577. Epub 2010 Mar 24 [PubMed PMID: 22319261]
Rahimi-Nasrabadi H, Jin J, Mazade R, Pons C, Najafian S, Alonso JM. Image luminance changes contrast sensitivity in visual cortex. Cell reports. 2021 Feb 2:34(5):108692. doi: 10.1016/j.celrep.2021.108692. Epub [PubMed PMID: 33535047]
Wang GJ, Pomerantzeff O. A new set of variable-contrast visual acuity charts. Optometry and vision science : official publication of the American Academy of Optometry. 1991 Jan:68(1):34-40 [PubMed PMID: 2023714]
Nakamura A, Akio T, Matsuda E, Wakami Y. Pattern visual evoked potentials in malingering. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2001 Mar:21(1):42-5 [PubMed PMID: 11315983]
Yap M, Grey C, Collinge A, Hurst M. The Arden gratings in optometric practice. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 1985:5(2):179-83 [PubMed PMID: 4022650]
Elliott DB, Sanderson K, Conkey A. The reliability of the Pelli-Robson contrast sensitivity chart. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 1990 Jan:10(1):21-4 [PubMed PMID: 2330208]
Dougherty BE, Flom RE, Bullimore MA. An evaluation of the Mars Letter Contrast Sensitivity Test. Optometry and vision science : official publication of the American Academy of Optometry. 2005 Nov:82(11):970-5 [PubMed PMID: 16317373]
Level 3 (low-level) evidenceChen Z, Zhuang Y, Xu Z, Chan LYL, Zhang S, Ye Q, Feng L, Lu ZL, Li J. Sensitivity and Stability of Functional Vision Tests in Detecting Subtle Changes Under Multiple Simulated Conditions. Translational vision science & technology. 2021 Jun 1:10(7):7. doi: 10.1167/tvst.10.7.7. Epub [PubMed PMID: 34100925]
Spellman DC, Alexander KR, Fishman GA, Derlacki DJ. Letter contrast sensitivity in retinitis pigmentosa patients assessed by Regan charts. Retina (Philadelphia, Pa.). 1989:9(4):287-91 [PubMed PMID: 2629044]
Level 3 (low-level) evidenceRichman J, Zangalli C, Lu L, Wizov SS, Spaeth E, Spaeth GL. The Spaeth/Richman contrast sensitivity test (SPARCS): design, reproducibility and ability to identify patients with glaucoma. The British journal of ophthalmology. 2015 Jan:99(1):16-20. doi: 10.1136/bjophthalmol-2014-305223. Epub 2014 Jul 22 [PubMed PMID: 25053760]
Level 2 (mid-level) evidenceShah K, Naidoo K, Chagunda M, Loughman J. Evaluations of refraction competencies of ophthalmic technicians in Mozambique. Journal of optometry. 2016 Jul-Sep:9(3):148-57. doi: 10.1016/j.optom.2015.01.003. Epub 2015 Feb 7 [PubMed PMID: 25662363]
Fernandes TP, de Almeida NL, Butler PD, Santos NA. Spatial contrast sensitivity: effects of reliability, test-retest repeatability and sample size using the Metropsis software. Eye (London, England). 2019 Oct:33(10):1649-1657. doi: 10.1038/s41433-019-0477-0. Epub 2019 Jun 5 [PubMed PMID: 31165771]
Rasengane TA, Allen D, Manny RE. Development of temporal contrast sensitivity in human infants. Vision research. 1997 Jul:37(13):1747-54 [PubMed PMID: 9274761]
Bennett CR, Bex PJ, Bauer CM, Merabet LB. The Assessment of Visual Function and Functional Vision. Seminars in pediatric neurology. 2019 Oct:31():30-40. doi: 10.1016/j.spen.2019.05.006. Epub 2019 May 11 [PubMed PMID: 31548022]
Chung ST, Legge GE. Comparing the Shape of Contrast Sensitivity Functions for Normal and Low Vision. Investigative ophthalmology & visual science. 2016 Jan 1:57(1):198-207. doi: 10.1167/iovs.15-18084. Epub [PubMed PMID: 26795826]
Everson RM, Prashanth AK, Gabbay M, Knight BW, Sirovich L, Kaplan E. Representation of spatial frequency and orientation in the visual cortex. Proceedings of the National Academy of Sciences of the United States of America. 1998 Jul 7:95(14):8334-8 [PubMed PMID: 9653187]
Level 3 (low-level) evidenceCunningham IA, Fenster A. A method for modulation transfer function determination from edge profiles with correction for finite-element differentiation. Medical physics. 1987 Jul-Aug:14(4):533-7 [PubMed PMID: 3626992]
Gray R, Regan D. Spatial frequency discrimination and detection characteristics for gratings defined by orientation texture. Vision research. 1998 Sep:38(17):2601-17 [PubMed PMID: 12116706]
Jamar JH, Koenderink JJ. Sine-wave gratings: scale invariance and spatial integration at suprathreshold contrast. Vision research. 1983:23(8):805-10 [PubMed PMID: 6623940]
Tolhurst DJ. Adaptation to square-wave gratings: inhibition between spatial frequency channels in the human visual system. The Journal of physiology. 1972 Oct:226(1):231-48 [PubMed PMID: 4343317]
Shandiz JH, Derakhshan A, Daneshyar A, Azimi A, Moghaddam HO, Yekta AA, Yazdi SH, Esmaily H. Effect of cataract type and severity on visual acuity and contrast sensitivity. Journal of ophthalmic & vision research. 2011 Jan:6(1):26-31 [PubMed PMID: 22454703]
Thomas M, Silverman RF, Vingopoulos F, Kasetty M, Yu G, Kim EL, Omari AA, Joltikov KA, Choi EY, Kim LA, Zacks DN, Miller JB. Active Learning of Contrast Sensitivity to Assess Visual Function in Macula-off Retinal Detachment. Journal of vitreoretinal diseases. 2021 Jul 1:5(4):313-320. doi: 10.1177/2474126420961957. Epub 2020 Nov 5 [PubMed PMID: 34458662]
Pelli DG, Bex P. Measuring contrast sensitivity. Vision research. 2013 Sep 20:90():10-4. doi: 10.1016/j.visres.2013.04.015. Epub 2013 May 3 [PubMed PMID: 23643905]