Introduction
The human crystalline lens accounts for +15 to +20 (approximately 17) diopters of the refractive power of the eye.[1] The cornea contributes another 43 diopters.[1] Cataract surgery involves the removal of the opacified crystalline lens, making the eye aphakic. Before the invention of intraocular lenses (IOLs) by Sir Harold Ridley to correct aphakia, spectacle correction was the norm.[2][3]
Aphakic spectacles were unsightly and heavy. They cause spherical aberrations and distortion in vision.[4][5] Removal of the entire crystalline lens by intracapsular cataract extraction (ICCE) necessitated implantation of the intraocular lens in the anterior chamber. This led to the invention of various designs of lenses after the original Ridley lens.[5][6][7]
Peter Choyce and Sir Harold Ridley formed the International Intraocular implant club in 1966. This led to the gradual acceptance of intraocular lenses. Intracapsular cataract extraction with anterior chamber IOL[7][8] was gradually replaced by extracapsular cataract surgery with posterior chamber IOLs.[3][9] However, the original Ridley lens was implanted after extracapsular cataract surgery, which involves leaving the posterior capsule of the lens behind.[1]
Charles Kelman revolutionized cataract surgery by inventing the technique of phacoemulsification.[10] Howard Gimbel invented the technique of capsulorhexis, due to which intraocular lenses could be implanted in the bag.[11][12] Femtosecond laser technology further improved the precision with which surgery could be performed.[13]
Intraocular lenses have transitioned from anterior chamber IOLs to posterior chamber IOLs, which have undergone further modification from rigid polymethylmethacrylate (PMMA) lenses to silicone and acrylic lenses. Lens materials and designs have undergone many improvements. Hydrophilic and hydrophobic lens materials are both in vogue. Open looped, closed-loop, plate haptic, and square-edged designs are currently being implanted, each modification attempting to decrease the incidence of complications, including posterior capsular opacification. Monofocal intraocular lenses to correct distance vision are the most commonly implanted intraocular lenses.[14]
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
The function of intraocular lenses is to correct aphakia caused by removing the crystalline lens. Before the invention of IOLs, the removal of cataracts led to the patient being highly hyperopic. Spectacle lenses of + 10 D to + 12 D were routinely prescribed for distance. Near vision usually needed another +3 D (+13 to +15 D). The spectacles were heavy, cosmetically unsightly, and had high spherical and chromatic aberrations.[15][16]
The indication of an intraocular lens is the visual correction of aphakia after cataract extraction.
Lens materials - Monofocal intraocular lenses may be made of polymethyl methacrylate (PMMA), which is rigid. Foldable IOL materials include silicone, hydrophobic acrylic materials, and hydrophilic acrylic materials.
The refractive indices of different IOL materials are:
- PMMA: 1.49
- Silicone IOL: 1.41 - 1.46
- Hydrophilic acrylic: 1.44 – 1.55
- Hydrophobic acrylic: 1.43 - 1.46.
The central, usually round part of the IOL is called an optic. The optic size varies from 5.25 mm to 6.5 mm. The total length of the IOL includes the total diameter of central optic and peripheral haptics. It varies from 12 to 13.5 mm. The optic may be plano-convex, biconvex, or concavo-convex (meniscus IOLs used to manage pathological myopes).
The anterior surface may be spherical or aspheric. The lens optic and the haptic may be made up of a single material (single piece IOL), or the haptics may be made of a separate material including polypropylene and nylon in a three-piece (multi-piece or 3-piece) IOL. The haptic may be J or C shaped. The haptic may be plate-shaped.
Monofocal intraocular lenses may be implanted after intracapsular cataract surgery. Anterior chamber IOL (Kelman multiflex type), in which the haptics are fixated in the angles of the anterior chamber, is most commonly used nowadays if an anterior chamber lens is implanted. It has 4 point fixation in the angle of the anterior chamber. Earlier, there were many models of anterior chamber lenses such as Choyce Mark IV, Sputnik lens, and Singh and Worst iris claw lens.[17][18] Posteriorly placed IOLs may be placed in the sulcus, implanted in the capsular bag, scleral fixated, iris-sutured, or posteriorly fixated (retropupillary) iris-claw lens.
The original Ridley lens was replaced by different models of lenses. Lens materials, shape, and size have undergone many modifications. The purpose of an intraocular lens is to correct aphakia. The lens material has to be inert. The shape should ensure proper placement and avoid decentration in the long term and should not cause loss of corneal endothelium while implanting or in the long- term.
Issues of Concern
Biocompatibility
Any foreign material that remains in the eye for a long time must be inert. The original Ridley lens was made of PMMA. This material from the canopy of aircraft was found to lie inert in the eye of injured pilots for a long period.[19]
Aqueous Absorption by IOL
The IOL should not absorb water in the eye. Some IOL materials may absorb aqueous and form glistening, which may not affect vision.[20][21] As water enters the lens, it accumulates in low polymer density areas and forms vacuoles. When the vacuoles enlarge, they are visible under slit-lamp biomicroscopy as glistenings.[21] Hygroscopy of a material denotes the ability to absorb or draw water and hold water.
IOL Opacification
Opacification of the IOL may occur in hydrophilic IOLs.[22][23] Opacification of hydrophilic lenses has been described after pars plana vitrectomy and intraocular gas injection.[22] A decrease in vision may necessitate an explantation of the IOLs. Opacification of hydrophilic IOLs has also been described after endothelial keratoplasty.[24][25]
Calcium deposits in the anterior surface of the lens may be caused by factors such as air injection or gas injection intraocularly, causing an electrolyte imbalance in the anterior chamber. Chronic inflammation and systemic diseases such as diabetes mellitus may be other factors.[24][25]
Compatibility with the Site of Placement
- Compatibility with iris in case of an anterior chamber IOL and anterior fixated iris-claw lens:[26] In a retrospective analysis of 171 eyes of 151 patients who underwent implantation of the iris-claw lens after cataract surgery, due to either complicated surgery, ectopia lentis, or trauma. The authors found a higher incidence of raised intraocular pressure and macular edema in anteriorly fixated claw lenses. In the long term, endothelial cell loss was also more after anterior fixation of the iris-claw lens compared to retropupillary fixation of the iris-claw lens.[26]
- Compatibility with ciliary sulcus in case of sulcus fixated IOL: In a study of 559 pseudophakic cadaver eyes obtained from eye banks, hydrophobic acrylic IOLs were noted in 256 eyes and had anterior and posterior square optic edges.[27] Out of these IOLs, 18 had asymmetric or sulcus fixation. Six of these IOLs were single-piece, and 12 were 3-piece IOLs. When compared to eyes with symmetric in the bag IOLs, there was IOL decentration, tilt, pigment dispersion in the anterior segment, and iris transillumination defects. Sulcus fixation in the case of the single-piece lens may lead to uveitis glaucoma hyphema syndrome. Three-piece lenses may be implanted after complications in surgery, and all the findings may not be attributable to sulcus fixation.[27] Posterior capsular rent and retained cortical matter may cause chronic uveitis and cystoid macular edema.
- Compatibility with the capsular bag in cases of in the bag IOL: Small capsulorhexis, pseudoexfoliation syndrome, retinitis pigmentosa, and closed-loop haptic lenses may all predispose to capsular bag phimosis.[28] Phimosis of the capsular bag may lead to the folding of IOL haptics over the optics in severe cases. This may cause a decrease in the visual acuity, necessitating the explantation of the IOL with the capsular bag and replacement with scleral fixated IOL.[28] The edge of the rhexis may be seen even in small pupils, causing a decrease in visual acuity. As more and more lenses are implanted "in the bag" and not in the ciliary sulcus, capsular bag contraction is more often encountered.[29] The intraocular lens should maintain its centration and resist capsular bag contraction. Capsular bag contraction under various circumstances has been described.[30] Highly myopic eyes, weak zonules, and pseudoexfoliation syndrome may predispose to capsular bag contraction in the long term.[31][32] This can lead to IOL decentration and dislocation. YAG laser has been used to relieve the capsular phimosis with some success.[33][28]
- Compatibility with the iris in case of posterior (retropupillary) fixation of the iris-claw lens:[34] In a retrospective study, 49 patients with posterior capsular loss had retropupillary implantation of the iris-claw lens along with pars plana vitrectomy, and 126 eyes that had dislocation of IOL also were managed by retropupillary fixation of the iris-claw lens. Visual outcomes in both groups were comparable, and intraocular pressure was also within normal limits.[34]
- Compatibility with pars plana (ciliary body) in case of scleral fixated IOL: In a retrospective study of 45 eyes of 42 patients who underwent glueless, sutureless scleral fixation of intraocular lens, visual acuity improved from a median LogMAR of 1.48 to 0.6 LogMAR.[35] Vitreous hemorrhage was seen in 13 % of cases, and postoperative hypotony was noted in 11% of cases. The other complications were cystoid macular edema, rise in intraocular pressure (IOP), hyphema, IOL tilt, and retinal detachment.[35].
Protection from Ultraviolet Rays
Intraocular lenses should provide protection from ultraviolet (UV) rays.[36] The human adult crystalline lens absorbs UV radiation between 300 and 400 nm. Removal of the crystalline lens during cataract surgery removes this protection. The preferred choice is to replace the crystalline lens with UV blocking intraocular lenses, with a 10 % cut-off near 400 nm.
UV light and other light of short wavelengths such as blue light may cause damage to the outer segments of the photoreceptor and the retinal pigment epithelium. The development of blue filtering intraocular lenses (BFIOL), which are yellow or orange tilted, may further improve protection from possible phototoxicity to the macula, improve contrast sensitivity, and reduce the chromatic aberrations.[37][38]
IOL can be rigid or foldable. In a study comparing the results of rigid PMMA lenses implanted through a 5 mm sclerocorneal tunnel and hydrophilic acrylic lenses implanted through a 2.5 mm corneal incision, visual outcomes were found to be comparable after one year. However, posterior capsular opacification was higher in the PMMA group (36%) than in the foldable group (23%).[39]
Posterior Capsular Opacification (PCO)
The lens design should prevent posterior capsular opacification by preventing the migration of Elschnig's pearls. PCO may be associated with capsular bag distension and cyst-like structures at the posterior capsule.[40] Mastromonaco et al. examined the capsular bags with IOLs in 190 donor eyes.[41]
PCO is caused by the deposition of extracellular matrix (ECM) by cells with myofibroblast phenotype arising from the lens epithelial cells after epithelial to mesenchymal transition. Higher expression of smooth muscle actin (SMA) and fibronectin (FN) which are the components of the ECM, was seen in bags with single-piece haptic IOLs compared to three-piece lenses. Capsular bags with silicone lenses had lesser SMA and FN expression than acrylic IOLs. Lens epithelial cells (LEC) behaved differently depending on the lens biocompatibility.[41]
Different lens coatings have been tried to prevent posterior capsular opacification.[42] The most important factors for the prevention of PCO include:
- Sharp truncated edges of IOL optic were found to have a lesser incidence of posterior capsular opacification than round-edged IOLs.[43][42][44] The square edge around the optic is absent in some older models at the optic-haptic junction through which the lens epithelial cells from the equator of the capsular bag can potentially migrate behind the optic. Newer IOLs have a 360-degree square edge or enhanced edge to avoid this problem.
- Maximal touch of the IOL optic to the posterior capsule, angulated haptics enhancing the contact of the optic to the posterior capsule, and bioadhesive material to promote a 'shrink-wrap' of the capsular bag around the optic.
- The biocompatibility of IOL materials: The rate of PCO is highest with hydrogel IOL, intermediate with PMMA, and lowest with silicone and acrylic material of the optic.[45]
- A continuous curvilinear capsulorhexis with a 360-degree overlap of the anterior capsulorhexis margin over the IOL optic creates a 'shrink-wrap' around the IOL optic.
- Meticulous cortical cleanup assisted by hydrodissection, and
- Implantation of the IOL in the capsular bag.[46]
The rate of PCO is higher with rigid IOLs compared to foldable IOLs.[46] Active oxygen processing (with ultraviolet and ozone) of IOLs may reduce the PCO rates.[47][48]
Endothelial Cell Loss
IOL should not cause endothelial cell loss while being implanted or long-term. The location of the IOL and the complications encountered during the procedure rather than the lens material causes endothelial cell loss. The use of different viscoelastic materials protects the corneal endothelium during various stages of cataract surgery and while implanting the intraocular lens.[49]
Endothelial cell loss has been evaluated during phacoemulsification. Francisco Sorrentino studied endothelial cell loss in 50 eyes after phacoemulsification. The main damage to endothelial cells was found to be in the second phase of phacoemulsification (quadrant removal as opposed to sculpting).[50] Intraocular lens implantation was not noted to cause endothelial cell loss.
Aberrations
Spherical and chromatic aberrations have been studied with various monofocal IOLs after IOL implantation. Nakajima et al. studied longitudinal chromatic aberrations (LCA) after implantation of three different types of yellow-colored IOLs. Alcon IOL and IOL from HOYA corp were found to have the same LCA as phakic eyes. The LCA in all the lenses did not affect the visual function.[51]
A study comparing chromatic aberrations after implanting monofocal, multifocal and extended depth of focus lenses did not find a significant difference between the three types of lenses.[52]
Nanavaty et al., while comparing monofocal IOL with enhanced depth of focus IOL, did not find differences in corrected distance visual acuity (CDVA) or significant differences in aberrations with normal pupil size.[53]
Inflammation and Infections
The surface should be resistant to bacterial adherence. Lens material has been found to be the most important factor determining bacterial adherence. Silicone and hydrophobic acrylic material allow bacterial adherence more readily than hydrophilic material.[54] Bacterial growth and replication occur following the adhesion to the IOL, forming microcolonies.[55] A slime layer forms and the bacteria are embedded in it. The perfect material to prevent biofilm adhesion is yet to be discovered. Silicone and PMMA are more prone to bacterial adhesion than hydrophilic and hydrophobic acrylic material.[55][54]
Endophthalmitis
Amongst all the complications after cataract surgery, endophthalmitis is the most devastating.[56][57] In a meta-analysis of 39 studies including 5,878,114 eyes, the incidence of endophthalmitis was 0.092% after phacoemulsification. The incidence of endophthalmitis decreased decade after decade, probably due to povidone-iodine prophylaxis and the use of intracameral cefuroxime or moxifloxacin.[56][58][59]
Dysphotopsia
Photic phenomena perceived by patients after cataract surgery can be noted, including arcs, rings, flashes, and haloes seen near the central axis of vision (positive dysphotopsia) or seen as blockage of light from certain parts of the retina, which appears as a dark shadow in the temporal field of vision (negative dysphotopsia).[60]
The incidence varies from 0.2 %, as reported by Davison in patients who had hydrophobic acrylic IOLs implanted, to 15.2% on the first preoperative day, which decreased to 2.4% after two years, as reported by Osher. Most of the time, there is no need for IOL explantation.[61][62][63]
Clinical Significance
Before the invention of the intraocular lens, aphakia due to the removal of the crystalline lens was corrected by spectacles or by contact lens. The high hyperopia needed thick convex lenses, which were heavy, cosmetically unsightly, and caused distortion in vision due to spherical aberrations, coma, and prismatic effect. More than 100 million intraocular lenses have been implanted since 1973 when IOLs gained acceptance.
The materials and designs are constantly undergoing modifications. The original Ridley lens was made of polymethylmethacrylate. Even today, rigid intraocular lenses are implanted after extracapsular cataract surgery and manual small incision cataract surgery. The cost of manufacturing these lenses is minimal, and smaller lenses can be implanted in the capsular bag. The disadvantage of the rigid lens is the need for a large incision size which may be sutured in case of extracapsular surgery and may not need sutures in manual small incision surgery.
Most cataract surgeries are now being performed by phacoemulsification through a 2.2 or 2.8 mm incision, which may be clear corneal or through a scleral tunnel. The lens materials are amenable to being folded and inserted through these incisions. The lenses may be single-piece with the optics and haptics made of the same material. The optics may be made of modified acrylic material, and the haptics may be polypropylene.
Intraocular lenses have undergone many changes over the years. The design of lens optics has changed from the original Ridley lens, which was biconvex. The optics are either spherical or aspheric.[64][65] The haptics may be round or square-edged.[66] Lens material may be hydrophobic or hydrophilic.[67]
The modifications that monofocal lenses have undergone over the years have been to ensure better centration in the capsular bag, reduce posterior capsular opacification, reduce spherical and chromatic aberrations, improve ease of implantation, ensure protection from UV light, and prevent bacterial adherence to the lens material.[54][68]
Other Issues
Monofocal lenses were the standard of care over a long period. With the increased demand for spectacle independence and the increasing use of computers and other screen devices, the need for better intermediate and near acuity also arose. Bifocal intraocular lenses, which corrected both distance and near, were manufactured.
Reduction of contrast sensitivity and nighttime glare/haloes were some issues accompanying the bifocal IOLs. The intermediate vision needed correction with spectacles, or the distance at which the devices were used had to be adjusted. Enhanced optics lenses were manufactured, which could give better near acuity without spectacle correction than monofocal lenses.[69]
Furthermore, enhanced depth of focus lenses (EDOF) gave better intermediate vision without the use of spectacles.[70] Trifocal IOLs also solved the problem of intermediate vision while giving good distance and near vision without spectacle correction.[71]
Toric versions have been introduced in monofocal, bifocal, or trifocal IOLs to take care of corneal astigmatism so that astigmatism for distance vision is reduced and the need for glasses for distance is minimized.
Enhancing Healthcare Team Outcomes
The implantation of an intraocular lens is the final link in a long series of events. The process starts with an examination of the patient in an outpatient clinic by the optometrist, who checks the patient's vision and refractive error.
A decrease in the best-corrected visual acuity, which is attributable to the development of cataracts, is confirmed by the ophthalmologist, who then recommends cataract surgery. The optometrist then performs biometry for the calculation of the IOL power. Keratometry and measurement of the axial length (by optical biometry or ultrasonic biometry) of the eye are done for regression formulas such as the Sanders-Reztlaff-Kraff (SRK) formula.[72][73]
Newer formulas like Holladay, Barret's, and Lada's Super formula have improved the predictability of postoperative refractive error in highly hyperopic or highly myopic, or post-refractive surgery eyes.[74] Similarly, IOL power calculation after silicone oil removal or combined phacoemulsification with posterior lamellar corneal surgery may need different formulas.[75][76][77]
Swept-source biometry by devices such as IOL master has improved the accuracy of IOL power calculations.[78] Accurate calculation of the IOL power is important. The role of the optometrist in IOL power calculation cannot be overemphasized.
Following this, pre-anesthetic evaluation is done by the clinician and anesthetist in patients with comorbidities. Many comorbidities must be addressed. Control of diabetes, hypertension, and chronic obstructive pulmonary disease is taken care of by the physician. The ability to lie flat for the duration of the procedure is essential.[79]
Diseases such as ankylosing spondylitis may make positioning the patient difficult. Drug history assumes its own importance. Certain medications like tamsulosin may cause floppy iris during surgery.[80][81]
Stopping blood thinners prior to cataract surgery is debatable. Patients who have undergone mitral or aortic valve replacement, have stents placed for coronary thrombosis, or have suffered strokes due to thrombosis, may be receiving blood thinners like aspirin, clopidogrel, or heparin. Such patients may be given topical instead of local anesthesia. When complicated or longer procedures are anticipated, such as small pupil, floppy iris, or hard cataract, local anesthesia in the form of peribulbar block may be needed. In such cases, the anesthetist or the attending clinician has to make the judgment call on stopping the blood thinners prior to surgery and assess the risk to life.
When congenital cataract surgery with monofocal lens implantation is performed, general anesthesia is chosen. IOL power calculation is done under GA. Here, the clinician, anesthetist, and nursing staff are all involved in preoperative, intraoperative, and postoperative care.[82][83]
Nursing, Allied Health, and Interprofessional Team Interventions
The nursing staff provides preoperative and postoperative care. They also perform proper dilation of the patient's eye with topical phenylephrine, tropicamide, or cycloplegics such as homatropine 2% or cyclopentolate 1%. If allergy to any topical drop has previously been documented, it must be avoided.
Vital parameters have to be recorded. Pulse, blood pressure, and blood sugar must be monitored. In the case of peribulbar anesthesia, a xylocaine sensitivity test may be done. Asthmatic patients or those with chronic obstructive pulmonary disease may need nebulization before surgery.
Perioperative use of an oxygen concentrator may be required in such patients. Proper positioning on the operating table, easing the patient's anxiety, and sometimes use of anxiolytics or mild sedatives may be done by the anesthesia team and the nursing staff.[84]
Nursing, Allied Health, and Interprofessional Team Monitoring
Cataract surgery has advanced from simple intracapsular surgery to phacoemulsification and femtosecond laser-assisted cataract surgery with topical anesthesia through a 2.2 mm clear corneal incision that heals rapidly and restores vision within hours after the procedure. However, proper planning from preoperative patient evaluation by the optometrist and the ophthalmologist, followed by clinician evaluation, perioperative monitoring, and post-operative care, involves many medical and allied specialties.
Trained operating room personnel help to ensure operating room (OR) sterility. Engineers ensure the proper functioning of Femto laser machines and phacoemulsification machines. Sterilization of instruments is taken care of by the OR staff who also ensure proper humidity and temperature in the operating room, making a cataract surgery procedure a team effort.
Cataract surgery is one of the most common surgeries performed on humans. The interprofessional collaboration makes the current cataract surgery a safe procedure ensuring the best outcomes for the patients.[85]
Media
(Click Image to Enlarge)
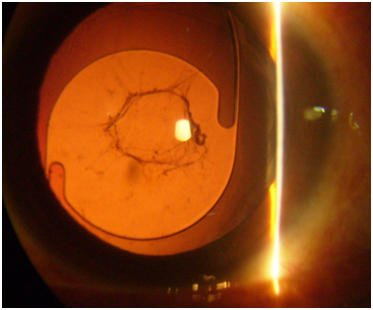
slit lamp photograph of monofocal posterior chamberintraocular lens taken in retroillumination. Yag laser capsulotomy opening is seen. Contributed by Uma Sridhar- Cornea illustrated- aguide to clinical diagnosis
References
Kolb H, Fernandez E, Nelson R, Nguyen J, Werner L. Intraocular Lenses for Cataract Surgery. Webvision: The Organization of the Retina and Visual System. 1995:(): [PubMed PMID: 29437325]
Ridley H. Intra-ocular acrylic lenses after cataract extraction. 1952. Bulletin of the World Health Organization. 2003:81(10):758-61 [PubMed PMID: 14758438]
Trivedi RH, Apple DJ, Pandey SK, Werner L, Izak AM, Vasavada AR, Ram J. Sir Nicholas Harold Ridley. He changed the world, so that we might better see it. Indian journal of ophthalmology. 2003 Sep:51(3):211-6 [PubMed PMID: 14601845]
Pouw CA,Zegers RH, [The development of cataract surgery after 1745]. Nederlands tijdschrift voor geneeskunde. 2013; [PubMed PMID: 23548190]
Marmamula S, Khanna RC, Shekhar K, Rao GN. Outcomes of Cataract Surgery in Urban and Rural Population in the South Indian State of Andhra Pradesh: Rapid Assessment of Visual Impairment (RAVI) Project. PloS one. 2016:11(12):e0167708. doi: 10.1371/journal.pone.0167708. Epub 2016 Dec 5 [PubMed PMID: 27918589]
Pandey SK, Apple DJ. Professor Peter Choyce: an early pioneer of intraocular lenses and corneal/refractive surgery. Clinical & experimental ophthalmology. 2005 Jun:33(3):288-93 [PubMed PMID: 15932534]
Alió JL, Kelman C. The Duet-Kelman lens: A new exchangeable angle-supported phakic intraocular lens. Journal of refractive surgery (Thorofare, N.J. : 1995). 2003 Sep-Oct:19(5):488-95 [PubMed PMID: 14518737]
Level 3 (low-level) evidenceHennig A,Evans JR,Pradhan D,Johnson GJ,Pokhrel RP,Gregson RM,Hayes R,Wormald RP,Foster A, Randomised controlled trial of anterior-chamber intraocular lenses. Lancet (London, England). 1997 Apr 19; [PubMed PMID: 9113011]
Level 1 (high-level) evidenceQuentin CD, Behrens-Baumann W, Lindemann K, Hilgers R, Vogel M. [Cystoid macular edema and visual acuity with intracapsular cataract extraction and Choyce anterior chamber lens vs. extracapsular cataract extraction and posterior chamber lens in the partner eye]. Der Ophthalmologe : Zeitschrift der Deutschen Ophthalmologischen Gesellschaft. 1993 Aug:90(4):364-6 [PubMed PMID: 8374234]
Level 1 (high-level) evidenceKelman CD. Phaco-Emulsification and Aspiration: A New Technique of Cataract Removal: A Preliminary Report. American journal of ophthalmology. 2018 Jul:191():xxx-xl. doi: 10.1016/j.ajo.2018.04.014. Epub [PubMed PMID: 29929630]
Gimbel HV, Neuhann T. Continuous curvilinear capsulorhexis. Journal of cataract and refractive surgery. 1991 Jan:17(1):110-1 [PubMed PMID: 2005552]
Level 3 (low-level) evidenceGimbel HV,Neuhann T, Development, advantages, and methods of the continuous circular capsulorhexis technique. Journal of cataract and refractive surgery. 1990 Jan; [PubMed PMID: 2299571]
Pirogova ES, Fabrikantov OL, Nikolashin SI. [Femtolaser-assisted phacoemulsification of intumescent cataract]. Vestnik oftalmologii. 2022:138(1):13-22. doi: 10.17116/oftalma202213801113. Epub [PubMed PMID: 35234416]
Calladine D, Evans JR, Shah S, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Sao Paulo medical journal = Revista paulista de medicina. 2015 Feb:133(1):68. doi: 10.1590/1516-3180.20151331T2. Epub 2015 Jan 1 [PubMed PMID: 25626855]
Fletcher A, Vijaykumar V, Selvaraj S, Thulasiraj RD, Ellwein LB. The Madurai Intraocular Lens Study. III: Visual functioning and quality of life outcomes. American journal of ophthalmology. 1998 Jan:125(1):26-35 [PubMed PMID: 9437310]
Level 1 (high-level) evidencePrajna NV, Chandrakanth KS, Kim R, Narendran V, Selvakumar S, Rohini G, Manoharan N, Bangdiwala SI, Ellwein LB, Kupfer C. The Madurai Intraocular Lens Study. II: Clinical outcomes. American journal of ophthalmology. 1998 Jan:125(1):14-25 [PubMed PMID: 9437309]
Level 1 (high-level) evidenceHirji N, Nanavaty MA. Management of corneal decompensation 4 decades after Sputnik intraocular lens implantation. Eye & contact lens. 2015 Jan:41(1):e1-4. doi: 10.1097/ICL.0b013e31829e8f03. Epub [PubMed PMID: 24113460]
Level 3 (low-level) evidenceTouriño Peralba R, Lamas-Francis D, Sarandeses-Diez T, Martínez-Pérez L, Rodríguez-Ares T. Iris-claw intraocular lens for aphakia: Can location influence the final outcomes? Journal of cataract and refractive surgery. 2018 Jul:44(7):818-826. doi: 10.1016/j.jcrs.2018.05.010. Epub [PubMed PMID: 30055690]
Sarwar H, Modi N. Sir Harold Ridley: innovator of cataract surgery. Journal of perioperative practice. 2014 Sep:24(9):210-2 [PubMed PMID: 25326942]
Tripathy K, Sridhar U. Optical coherence tomography of intraocular lens glistening. Indian journal of ophthalmology. 2019 Jan:67(1):138-139. doi: 10.4103/ijo.IJO_1031_18. Epub [PubMed PMID: 30574921]
Yildirim TM, Schickhardt SK, Wang Q, Friedmann E, Khoramnia R, Auffarth GU. Quantitative evaluation of microvacuole formation in five intraocular lens models made of different hydrophobic materials. PloS one. 2021:16(4):e0250860. doi: 10.1371/journal.pone.0250860. Epub 2021 Apr 30 [PubMed PMID: 33930084]
Marcovich AL, Tandogan T, Bareket M, Eting E, Kaplan-Ashiri I, Bukelman A, Auffarth GU, Khoramnia R. Opacification of hydrophilic intraocular lenses associated with vitrectomy and injection of intraocular gas. BMJ open ophthalmology. 2018:3(1):e000157. doi: 10.1136/bmjophth-2018-000157. Epub 2018 Dec 15 [PubMed PMID: 30623024]
Kanclerz P, Yildirim TM, Khoramnia R. A review of late intraocular lens opacifications. Current opinion in ophthalmology. 2021 Jan:32(1):31-44. doi: 10.1097/ICU.0000000000000719. Epub [PubMed PMID: 33165018]
Level 3 (low-level) evidenceTarnawska D, Balin K, Jastrzębska M, Talik A, Wrzalik R. Physicochemical Analysis of Sediments Formed on the Surface of Hydrophilic Intraocular Lens after Descemet's Stripping Endothelial Keratoplasty. Materials (Basel, Switzerland). 2020 Sep 17:13(18):. doi: 10.3390/ma13184145. Epub 2020 Sep 17 [PubMed PMID: 32957729]
Fernández J, Sánchez-García A, Rodríguez-Vallejo M, Piñero DP. Systematic review of potential causes of intraocular lens opacification. Clinical & experimental ophthalmology. 2020 Jan:48(1):89-97. doi: 10.1111/ceo.13650. Epub 2019 Oct 22 [PubMed PMID: 31581356]
Level 1 (high-level) evidenceAl-Dwairi R, Saleh O, Aleshawi A, Alladkanie Z, Al Deyabat O, Alasheh A, Adi S, Al-Howthi M. Anterior Versus Retropupillary Iris-Claw Intraocular Lens: Indications, Visual Outcome and Postoperative Complications. Ophthalmology and therapy. 2022 Apr:11(2):771-784. doi: 10.1007/s40123-022-00474-2. Epub 2022 Feb 11 [PubMed PMID: 35149965]
Kirk KR, Werner L, Jaber R, Strenk S, Strenk L, Mamalis N. Pathologic assessment of complications with asymmetric or sulcus fixation of square-edged hydrophobic acrylic intraocular lenses. Ophthalmology. 2012 May:119(5):907-13. doi: 10.1016/j.ophtha.2011.10.022. Epub 2012 Mar 15 [PubMed PMID: 22424575]
Naik M, Sethi H, Mehta A. Capsular bag phimosis. American journal of ophthalmology case reports. 2020 Dec:20():100999. doi: 10.1016/j.ajoc.2020.100999. Epub 2020 Dec 3 [PubMed PMID: 33319123]
Level 3 (low-level) evidenceGimbel HV, Van Westenbrugge JA, Sanders DR, Raanan MG. Effect of sulcus vs capsular fixation on YAG-induced pressure rises following posterior capsulotomy. Archives of ophthalmology (Chicago, Ill. : 1960). 1990 Aug:108(8):1126-9 [PubMed PMID: 2383202]
Wormstone IM, Damm NB, Kelp M, Eldred JA. Assessment of intraocular lens/capsular bag biomechanical interactions following cataract surgery in a human in vitro graded culture capsular bag model. Experimental eye research. 2021 Apr:205():108487. doi: 10.1016/j.exer.2021.108487. Epub 2021 Feb 8 [PubMed PMID: 33571531]
Wang W, Xu D, Liu X, Xu W. Case series: "Double arch" changes caused by capsule contraction syndrome after cataract surgery in highly myopic eyes. BMC ophthalmology. 2021 Oct 18:21(1):367. doi: 10.1186/s12886-021-02113-z. Epub 2021 Oct 18 [PubMed PMID: 34663265]
Level 2 (mid-level) evidenceVanags J, Erts R, Laganovska G. Anterior Capsule Opening Contraction and Late Intraocular Lens Dislocation after Cataract Surgery in Patients with Weak or Partially Absent Zonular Support. Medicina (Kaunas, Lithuania). 2021 Jan 3:57(1):. doi: 10.3390/medicina57010035. Epub 2021 Jan 3 [PubMed PMID: 33401604]
Gamidov AA, Andgelova DV, Averkina EA, Surnina ZV. [Role of ultrasound biomicroscopy in assessing the results of laser treatment in capsular contraction syndrome]. Vestnik oftalmologii. 2021:137(6):26-32. doi: 10.17116/oftalma202113706126. Epub [PubMed PMID: 34965064]
Zaleski M, Stahel M, Eberhard R, Alexander Blum R, Barthelmes D. OUTCOMES OF RETROPUPILLARY IRIS CLAW INTRAOCULAR LENS IMPLANTATION COMBINED WITH PARS PLANA VITRECTOMY. Retina (Philadelphia, Pa.). 2022 Jul 1:42(7):1284-1291. doi: 10.1097/IAE.0000000000003443. Epub 2022 Feb 17 [PubMed PMID: 35174810]
Mohanty A, Mahapatra SK, Mannem N. Multipiece posterior chamber intraocular lens as sutureless, glueless scleral fixated intraocular lens. Oman journal of ophthalmology. 2022 Jan-Apr:15(1):69-72. doi: 10.4103/ojo.ojo_115_21. Epub 2022 Mar 2 [PubMed PMID: 35388260]
Augustin AJ. [Reliable UV-light protection in intraocular lenses--scientific rationale and quality requirements]. Klinische Monatsblatter fur Augenheilkunde. 2014 Sep:231(9):901-8. doi: 10.1055/s-0034-1368566. Epub 2014 Jul 3 [PubMed PMID: 24992237]
Level 2 (mid-level) evidenceSee LC, Li PR, Lin KK, Hou CH, Lee JS. Effect of Blue Light-Filtering Intraocular Lenses on Insomnia After Cataract Surgery: A Nationwide Cohort Study With 10-Year Follow-up. American journal of ophthalmology. 2022 Jul:239():26-36. doi: 10.1016/j.ajo.2022.01.012. Epub 2022 Feb 4 [PubMed PMID: 35123954]
Downes SM. Ultraviolet or blue-filtering intraocular lenses: what is the evidence? Eye (London, England). 2016 Feb:30(2):215-21. doi: 10.1038/eye.2015.267. Epub 2016 Jan 8 [PubMed PMID: 26742866]
Hennig A, Puri LR, Sharma H, Evans JR, Yorston D. Foldable vs rigid lenses after phacoemulsification for cataract surgery: a randomised controlled trial. Eye (London, England). 2014 May:28(5):567-75. doi: 10.1038/eye.2014.26. Epub 2014 Feb 21 [PubMed PMID: 24556879]
Level 1 (high-level) evidenceTripathy K. Posterior Capsular Cyst on Anterior Segment OCT. Ophthalmology. 2018 Sep:125(9):1324. doi: 10.1016/j.ophtha.2018.06.033. Epub 2018 Aug 21 [PubMed PMID: 30143089]
Mastromonaco C, Balazsi M, Coblentz J, Dias ABT, Zoroquiain P, Burnier MN Jr. Histopathological analysis of residual lens cells in capsular opacities after cataract surgery using objective software. Indian journal of ophthalmology. 2022 May:70(5):1617-1625. doi: 10.4103/ijo.IJO_291_21. Epub [PubMed PMID: 35502038]
Han Y,Tang J,Xia J,Wang R,Qin C,Liu S,Zhao X,Chen H,Lin Q, Anti-Adhesive And Antiproliferative Synergistic Surface Modification Of Intraocular Lens For Reduced Posterior Capsular Opacification. International journal of nanomedicine. 2019 [PubMed PMID: 31819418]
Level 2 (mid-level) evidenceMaedel S, Evans JR, Harrer-Seely A, Findl O. Intraocular lens optic edge design for the prevention of posterior capsule opacification after cataract surgery. The Cochrane database of systematic reviews. 2021 Aug 16:8(8):CD012516. doi: 10.1002/14651858.CD012516.pub2. Epub 2021 Aug 16 [PubMed PMID: 34398965]
Level 1 (high-level) evidencePeng Q, Visessook N, Apple DJ, Pandey SK, Werner L, Escobar-Gomez M, Schoderbek R, Solomon KD, Guindi A. Surgical prevention of posterior capsule opacification. Part 3: Intraocular lens optic barrier effect as a second line of defense. Journal of cataract and refractive surgery. 2000 Feb:26(2):198-213 [PubMed PMID: 10683787]
Level 2 (mid-level) evidenceHollick EJ, Spalton DJ, Ursell PG, Meacock WR, Barman SA, Boyce JF. Posterior capsular opacification with hydrogel, polymethylmethacrylate, and silicone intraocular lenses: two-year results of a randomized prospective trial. American journal of ophthalmology. 2000 May:129(5):577-84 [PubMed PMID: 10844047]
Level 2 (mid-level) evidenceApple DJ, Peng Q, Visessook N, Werner L, Pandey SK, Escobar-Gomez M, Ram J, Auffarth GU. Eradication of posterior capsule opacification: documentation of a marked decrease in Nd:YAG laser posterior capsulotomy rates noted in an analysis of 5416 pseudophakic human eyes obtained postmortem. Ophthalmology. 2001 Mar:108(3):505-18 [PubMed PMID: 11237905]
Farukhi MA, Werner L, Kohl JC, Gardiner GL, Ford JR, Cole SC, Vasavada SA, Noristani R, Mamalis N. Evaluation of uveal and capsule biocompatibility of a single-piece hydrophobic acrylic intraocular lens with ultraviolet-ozone treatment on the posterior surface. Journal of cataract and refractive surgery. 2015 May:41(5):1081-7. doi: 10.1016/j.jcrs.2014.11.043. Epub 2015 Apr 29 [PubMed PMID: 25935337]
Matsushima H, Iwamoto H, Mukai K, Obara Y. Active oxygen processing for acrylic intraocular lenses to prevent posterior capsule opacification. Journal of cataract and refractive surgery. 2006 Jun:32(6):1035-40 [PubMed PMID: 16814067]
Level 3 (low-level) evidenceHessemer V, Dick B. [Viscoelastic substances in cataract surgery. Principles and current overview]. Klinische Monatsblatter fur Augenheilkunde. 1996 Aug-Sep:209(2-3):55-61 [PubMed PMID: 8992084]
Level 3 (low-level) evidenceSorrentino FS. Qualitative Alterations on Corneal Endothelial Cell Morphometry and Hexagonality After Cataract Surgery. Clinical ophthalmology (Auckland, N.Z.). 2021:15():4847-4853. doi: 10.2147/OPTH.S338001. Epub 2021 Dec 29 [PubMed PMID: 35002220]
Level 2 (mid-level) evidencePérez-Merino P, Dorronsoro C, Llorente L, Durán S, Jiménez-Alfaro I, Marcos S. In vivo chromatic aberration in eyes implanted with intraocular lenses. Investigative ophthalmology & visual science. 2013 Apr 12:54(4):2654-61. doi: 10.1167/iovs.13-11912. Epub 2013 Apr 12 [PubMed PMID: 23493299]
A Bartol-Puyal FD, Giménez G, Altemir I, Larrosa JM, Polo V, Pablo L. Optical aberrations in three different intraocular lens designs of a same platform. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2021 Apr-Jun:35(2):126-130. doi: 10.4103/1319-4534.337865. Epub 2022 Feb 18 [PubMed PMID: 35391809]
Nanavaty MA,Ashena Z,Gallagher S,Borkum S,Frattaroli P,Barbon E, Visual Acuity, Wavefront Aberrations, and Defocus Curves With an Enhanced Monofocal and a Monofocal Intraocular Lens: A Prospective, Randomized Study. Journal of refractive surgery (Thorofare, N.J. : 1995). 2022 Jan [PubMed PMID: 35020542]
Level 1 (high-level) evidenceBaillif S, Ecochard R, Hartmann D, Freney J, Kodjikian L. [Intraocular lens and cataract surgery: comparison between bacterial adhesion and risk of postoperative endophthalmitis according to intraocular lens biomaterial]. Journal francais d'ophtalmologie. 2009 Sep:32(7):515-28. doi: 10.1016/j.jfo.2009.04.026. Epub 2009 Jun 17 [PubMed PMID: 19539399]
Kodjikian L, Roques C, Pellon G, Renaud F, Hartmann D, Freney J, Burillon C. [Bacterial adhesion to intraocular lenses and endophthalmitis prevention: review of the literature]. Journal francais d'ophtalmologie. 2006 Jan:29(1):74-81 [PubMed PMID: 16465128]
Shi SL, Yu XN, Cui YL, Zheng SF, Shentu XC. Incidence of endophthalmitis after phacoemulsification cataract surgery: a Meta-analysis. International journal of ophthalmology. 2022:15(2):327-335. doi: 10.18240/ijo.2022.02.20. Epub 2022 Feb 18 [PubMed PMID: 35186695]
Level 1 (high-level) evidenceSimakurthy S, Tripathy K. Endophthalmitis. StatPearls. 2024 Jan:(): [PubMed PMID: 32644505]
Tripathy K. Re: Haripriya et al.: Endophthalmitis reduction with intracameral moxifloxacin prophylaxis: analysis of 600 000 surgeries (Ophthalmology. 2017;124:768-775). Ophthalmology. 2017 Sep:124(9):e72. doi: 10.1016/j.ophtha.2017.04.019. Epub [PubMed PMID: 28823359]
Haripriya A, Chang DF, Ravindran RD. Endophthalmitis Reduction with Intracameral Moxifloxacin Prophylaxis: Analysis of 600 000 Surgeries. Ophthalmology. 2017 Jun:124(6):768-775. doi: 10.1016/j.ophtha.2017.01.026. Epub 2017 Feb 14 [PubMed PMID: 28214101]
Wenzel M,Langenbucher A,Eppig T, [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klinische Monatsblatter fur Augenheilkunde. 2019 Jun [PubMed PMID: 28837979]
Davison JA. Positive and negative dysphotopsia in patients with acrylic intraocular lenses. Journal of cataract and refractive surgery. 2000 Sep:26(9):1346-55 [PubMed PMID: 11020620]
Level 3 (low-level) evidenceOsher RH. Differentiating transient and permanent negative dysphotopsia. Journal of cataract and refractive surgery. 2010 Sep:36(9):1619; author reply 161-9. doi: 10.1016/j.jcrs.2010.06.018. Epub [PubMed PMID: 20692588]
Level 3 (low-level) evidenceOsher RH. Negative dysphotopsia: long-term study and possible explanation for transient symptoms. Journal of cataract and refractive surgery. 2008 Oct:34(10):1699-707. doi: 10.1016/j.jcrs.2008.06.026. Epub [PubMed PMID: 18812121]
Rocha KM, Soriano ES, Chamon W, Chalita MR, Nosé W. Spherical aberration and depth of focus in eyes implanted with aspheric and spherical intraocular lenses: a prospective randomized study. Ophthalmology. 2007 Nov:114(11):2050-4 [PubMed PMID: 17445897]
Level 1 (high-level) evidencePlaceres Dabán J, Elvira JC, Azrak C, Rial L, Piñero DP, Belda JI. Long-Term Clinically Significant Posterior Capsular Opacification Development Pattern in Eyes Implanted with an Aspheric Monofocal Intraocular Lens with a Square Optic Edge. Journal of ophthalmology. 2021:2021():4566436. doi: 10.1155/2021/4566436. Epub 2021 Sep 30 [PubMed PMID: 34631162]
Belda JI, Dabán JP, Elvira JC, O'Boyle D, Puig X, Pérez-Vives C, Zou M, Sun S. Nd:YAG capsulotomy incidence associated with five different single-piece monofocal intraocular lenses: a 3-year Spanish real-world evidence study of 8293 eyes. Eye (London, England). 2022 Nov:36(11):2205-2210. doi: 10.1038/s41433-021-01828-z. Epub 2021 Nov 11 [PubMed PMID: 34764439]
Trakos N, Ioachim E, Tsanou E, Aspiotis M, Psilas K, Kalogeropoulos C. Findings of an experimental study in a rabbit model on posterior capsule opacification after implantation of hydrophobic acrylic and hydrophilic acrylic intraocular lenses. Clinical ophthalmology (Auckland, N.Z.). 2008 Dec:2(4):997-1005 [PubMed PMID: 19668459]
Fazly Bazzaz BS, Jalalzadeh M, Sanati M, Zarei-Ghanavati S, Khameneh B. Biofilm Formation by Staphylococcus epidermidis on Foldable and Rigid Intraocular Lenses. Jundishapur journal of microbiology. 2014 May:7(5):e10020. doi: 10.5812/jjm.10020. Epub 2014 May 1 [PubMed PMID: 25147711]
Huh J, Eom Y, Yang SK, Choi Y, Kim HM, Song JS. A comparison of clinical outcomes and optical performance between monofocal and new monofocal with enhanced intermediate function intraocular lenses: a case-control study. BMC ophthalmology. 2021 Oct 16:21(1):365. doi: 10.1186/s12886-021-02124-w. Epub 2021 Oct 16 [PubMed PMID: 34656091]
Level 2 (mid-level) evidenceSchmid R, Luedtke H, Borkenstein AF. Enhanced Depth-of-focus Intraocular Lenses: Latest Wavefront-shaped Optics versus Diffractive Optics. Optometry and vision science : official publication of the American Academy of Optometry. 2022 Apr 1:99(4):335-341. doi: 10.1097/OPX.0000000000001894. Epub [PubMed PMID: 35383733]
Britton JJL, El-Defrawy S, Wong BM, Chandrakumar M, Omali NB, Pham S, Hatch W. Patient Satisfaction and Visual Function Following Implantation of Trifocal or Extended Range of Vision Intraocular Lenses. Clinical ophthalmology (Auckland, N.Z.). 2022:16():669-676. doi: 10.2147/OPTH.S339385. Epub 2022 Mar 5 [PubMed PMID: 35282167]
Paritekar P, Nayak A, Umesh Y, Sirivella I, Manoharan S, Khatib Z. Comparison of newer Kane formula with Sanders Retzlaff Kraff/Theoretical and Barrett Universal II for calculation of intraocular lens power in Indian eyes. Indian journal of ophthalmology. 2022 Apr:70(4):1203-1207. doi: 10.4103/ijo.IJO_2014_21. Epub [PubMed PMID: 35326016]
Lin L, Xu M, Mo E, Huang S, Qi X, Gu S, Sun W, Su Q, Li J, Zhao YE. Accuracy of Newer Generation IOL Power Calculation Formulas in Eyes With High Axial Myopia. Journal of refractive surgery (Thorofare, N.J. : 1995). 2021 Nov:37(11):754-758. doi: 10.3928/1081597X-20210712-08. Epub 2021 Nov 1 [PubMed PMID: 34756144]
Level 2 (mid-level) evidenceIida Y, Shimizu K, Shoji N. Development of a New Method for Calculating Intraocular Lens Power after Myopic Laser In Situ Keratomileusis by Combining the Anterior-Posterior Ratio of the Corneal Radius of the Curvature with the Double-K Method. Journal of clinical medicine. 2022 Jan 20:11(3):. doi: 10.3390/jcm11030522. Epub 2022 Jan 20 [PubMed PMID: 35159971]
Diener R, Treder M, Lauermann JL, Eter N, Alnawaiseh M. Optimizing intraocular lens power calculation using adjusted conventional keratometry for cataract surgery combined with Descemet membrane endothelial keratoplasty. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2022 Sep:260(9):3087-3093. doi: 10.1007/s00417-022-05598-6. Epub 2022 Mar 8 [PubMed PMID: 35258717]
Hou Y, Liu L, Wang G, Xie J, Wang Y. Different lens power calculation formulas for the prediction of refractive outcome after phacoemulsification with silicone oil removal. BMC ophthalmology. 2022 Feb 13:22(1):74. doi: 10.1186/s12886-022-02304-2. Epub 2022 Feb 13 [PubMed PMID: 35151281]
Kanclerz P, Grzybowski A. Accuracy of Intraocular Lens Power Calculation in Eyes Filled with Silicone Oil. Seminars in ophthalmology. 2019:34(5):392-397. doi: 10.1080/08820538.2019.1636097. Epub 2019 Jul 1 [PubMed PMID: 31257972]
Dong J, Yao J, Chang S, Kanclerz P, Khoramnia R, Wang X. Comparison Study of the Two Biometers Based on Swept-Source Optical Coherence Tomography Technology. Diagnostics (Basel, Switzerland). 2022 Feb 26:12(3):. doi: 10.3390/diagnostics12030598. Epub 2022 Feb 26 [PubMed PMID: 35328151]
Khan MA, Burden J, Dinsmore J, Lockwood AJ. Making cataract surgery possible in patients with ankylosing spondylitis: A new positioning technique. American journal of ophthalmology case reports. 2022 Mar:25():101246. doi: 10.1016/j.ajoc.2021.101246. Epub 2021 Dec 22 [PubMed PMID: 35005297]
Level 3 (low-level) evidencePark SSE, Wilkinson S, Mamalis N. Dealing with floppy iris syndrome. Current opinion in ophthalmology. 2022 Jan 1:33(1):3-8. doi: 10.1097/ICU.0000000000000815. Epub [PubMed PMID: 34711714]
Level 3 (low-level) evidenceTobaiqy M, Aalam W, Banji D, Al Haleem ENA. Intraoperative Floppy Iris Syndrome Induced by Tamsulosin: The Risk and Preventive Strategies. Middle East African journal of ophthalmology. 2021 Jan-Mar:28(1):51-56. doi: 10.4103/meajo.MEAJO_561_20. Epub 2021 Apr 30 [PubMed PMID: 34321822]
Lenhart PD, Lambert SR. Current management of infantile cataracts. Survey of ophthalmology. 2022 Sep-Oct:67(5):1476-1505. doi: 10.1016/j.survophthal.2022.03.005. Epub 2022 Mar 17 [PubMed PMID: 35307324]
Level 3 (low-level) evidenceChattannavar G, Badakere A, Mohamed A, Kekunnaya R. Visual outcomes and complications in infantile cataract surgery: a real - world scenario. BMJ open ophthalmology. 2022:7(1):e000744. doi: 10.1136/bmjophth-2021-000744. Epub 2022 Mar 8 [PubMed PMID: 35342821]
Sadlak N, Fiorello MG, Cabral HJ, Subramanian ML, Desai MA, Lee HJ. Poor Correlation of Provider and Patient Satisfaction with Anesthesia in Ophthalmic Surgeries: A Secondary Analysis of a Clinical Trial. Clinical ophthalmology (Auckland, N.Z.). 2022:16():677-683. doi: 10.2147/OPTH.S351010. Epub 2022 Mar 6 [PubMed PMID: 35282171]
Micieli JA, Arshinoff SA. Cataract surgery. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2011 Oct 4:183(14):1621. doi: 10.1503/cmaj.110549. Epub 2011 Aug 8 [PubMed PMID: 21825045]