Introduction
Alveolar macrophages (AM), also known as dust cells, are a type of white blood cell (see Image. Lung histology 200x Magnification). The immune system is divided into the cellular and humoral components. Alveolar macrophages are the first line of defense against invading respiratory pathogens. They reside in pulmonary alveoli and the inter-alveolar septum near pneumocytes. The alveoli are the terminal respiratory system unit responsible for gaseous exchange. The alveoli are comprised of 3 different kinds of cells: (1) Type I pneumocytes build up the structure of the alveolar wall and aid in respiration. They do not replicate. (2) Type II pneumocytes secrete a lipoprotein called surfactant that prevents the collapse of the alveoli even after exhalation. (3) Alveolar macrophages produce various signaling chemicals that interact with other immune system cells to orchestrate a response that maintains immunologic and tissue homeostasis in the body [1]. Type II pneumocytes replete both types of pneumocytes and AMs, which in turn are vital to host defenses and tissue remodeling [2]
Structure
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure
All cell types of the mononuclear phagocyte system originate from the hematopoietic stem cells produced in bone marrow from the common myeloid progenitor. These myeloid cells further differentiate into myeloblasts, which give rise to monocytes. Monocytes travel in the bloodstream and mature in the organ's connective tissue to form macrophages [3]. Alveolar macrophages also can be present in the tissue from birth, independent of monocytes. Monocytes have a half-life of a day, whereas macrophages can live up to months or years in the tissue [4]. The size or shape of alveolar macrophages can vary among individuals depending on the phagocytic function and the living environment of the cell in the body. The cell membrane of alveolar macrophages can change its shape during mobilization or phagocytosis by activating the microtubule network. The movement of alveolar macrophages to the site of tissue injury in response to certain chemicals is known as chemotaxis [5]. Alveolar macrophages have a very distinct actin microfilament structure that aids in chemotaxis and endocytosis [6].
Function
Alveolar macrophages play an important role in scavenging microbes such as viruses, bacteria, fungi, inhaled environmental particles like coal, silica, asbestos, tissue debris, and cancer cells. Alveolar macrophages get activated by the interaction of toll-like receptors on the AM surface with the pathogen-associated molecular receptors on the microbial cell. The interplay between toll-like receptors and pathogen-associated molecular receptors transmits chemical signals that trigger the process of pathogen engulfment and the secretion of pro-inflammatory cytokines that enhance local immune response [7][8][7]. After phagocytosis, phagosomes are fused with lysosomes to form phagolysosomes and produce digestive enzymes that kill the pathogen. Certain bacteria, such as Mycobacterium Tuberculosis, can resist phagocytosis [9]. In such cases, alveolar macrophages prevent the infection from spreading to the other organs. Specific environmental particles like carbon and silica can be engulfed by macrophages in an attempt to keep them out of the bloodstream. Certain pro-inflammatory cytokines play an important part in tissue repair and fibrosis during an active inflammatory reaction.
Tissue Preparation
Resting macrophages are difficult to stain on hematoxylin and eosin preparations [10]. A practitioner can visualize them by injecting an experimental animal with very fine carbon particles. The engulfed carbon particles become visible as a dark, black-brown accumulation in the cytoplasm of the alveolar macrophages [10]. However, according to some studies, alveolar macrophages are more easily identifiable in pulmonary tissue sections than macrophages in other tissues of the body.
Histochemistry and Cytochemistry
Cells are differentiated from the surrounding tissue using a cluster of differentiation (CD) markers or the cell's surface molecules. There is no specific CD marker for alveolar macrophages. The cell recognition depends on the tissue in which macrophages must be detected, and the antibody can be tailored accordingly. CD11b and CD68 are associated with macrophages in the literature [11][12]. In 1 study, there is an increasing percentage of CD63, CD204, or CD206 positive cells found in the lungs of patients with chronic obstructive pulmonary disease compared to those in nonsmokers and smokers [13].
Microscopy, Light
In a healthy lung, there are at least 2 types of macrophages: alveolar macrophages (AM) and interstitial macrophages (IM) [14]. They are functionally different and can be distinguished by localization within the lung and expression of CD11b and CD11c. After exposure to a pathogen, polarized alveolar macrophages are divided into M1 and M2 cells [4]. M1 cells produce pro-inflammatory mediators like TNF-alpha and IL-1beta. M2 cells further differentiate and dominantly produce allergic cytokines IL-4 and IL-13; these are involved in the pathological mechanism of asthma [4]. One study established the role of IL-17 in allergic asthma. IL-17 is produced by alveolar macrophages and causes airway remodeling in patients with asthma [15].
Microscopy, Electron
Under the electron microscope, alveolar macrophages contain all the vital cell organelles, such as a variable-shaped nucleus with nucleoli, ribosomes, Golgi bodies, mitochondria, and, most importantly, lysosomes. Lysosomes contain digestive enzymes that help break down engulfed material.
Pathophysiology
Alveolar macrophages play an important role in tuberculosis infections. Mycobacterium tuberculosis bacteria evolved mechanisms that resist phagocytosis of macrophages. Alveolar macrophages gather around M. Tuberculosis and join to form a multinucleated giant cell (also known as Langerhans giant cell), surrounded by T-cells. TNF-alpha and IFN-gamma are particularly important in forming granuloma [16][17]. Tuberculosis is 1 of the leading causes of mortality and morbidity in patients with HIV, especially in underdeveloped countries where HART is not widely available. The hallmark finding of non-caseating granulomas in some systemic diseases, such as sarcoidosis, forms by joining alveolar macrophages to wall off the infectious process. Alveolar macrophages also secrete vitamin D and cause hypercalcemia in sarcoidosis, clinical criteria that help diagnose [18][19]. Alveolar macrophages also engulf harmful environmental particles such as carbon, which has been specifically reported in coal mine workers and termed pneumoconiosis. Similarly, crystalline silica particles can deactivate alveolar macrophages' immunologic response, mimicking tuberculosis. For this reason, patients with a history of silica exposure should have periodic tuberculosis testing.
Clinical Significance
Alveolar macrophages are also found in higher numbers in the bronchoalveolar lavage collected from the lungs of patients who smoke and those with chronic obstructive pulmonary disease. The macrophage count obtained by lavage is 4 to 6 times greater in smokers than nonsmokers. Apart from this, alveolar macrophages are morphologically different and contain more harmful pigment and free radicals in smokers than in non-smokers.[13][20]. Emphysema is a chronic lung disease caused by the destruction of terminal airways by elastases secreted by neutrophils. Interestingly, alveolar macrophages secrete elastases too, therefore elastases also are high in the lavage of smokers.[21][22] In that aspect, the role of alveolar macrophages in emphysema can give more insight into the disease process and a new avenue for research. Alveolar macrophages are involved in interstitial pulmonary fibrosis, a condition in which fibrotic tissue replaces lung tissue. Fibroblasts are absent in healthy lung tissue but have been found in the bronchoalveolar lavage fluid of interstitial pulmonary fibrosis.
In some studies, fibroblasts are considered a subset of alveolar macrophages as they express the same monocyte surface markers, such as CD11b and CD14. Surfactants are phospholipids produced by pneumocytes that prevent the collapse of alveolar walls during expiration. Another function of alveolar macrophages is to remove excess surfactant and thus maintain homeostasis. Alveolar macrophages require stimulation from a signaling molecule known as granulocyte/macrophage-colony stimulating factor to clear excess surfactant. Pulmonary alveolar proteinosis (PAP) is a spectrum of autoimmune diseases in which antibodies are formed against granulocyte/macrophage-colony stimulating factor, halting the function of alveolar macrophages, thus building up excess surfactant. A hereditary form of PAP is a rare condition in children between the ages of 1 and 10 years, resulting from the mutation of granulocyte/macrophage-colony stimulating factor on alveolar macrophages [23]. In short, alveolar macrophages play an important role in the body's defense against pathogens and foreign bodies, walling off infections and repair.
Media
(Click Image to Enlarge)
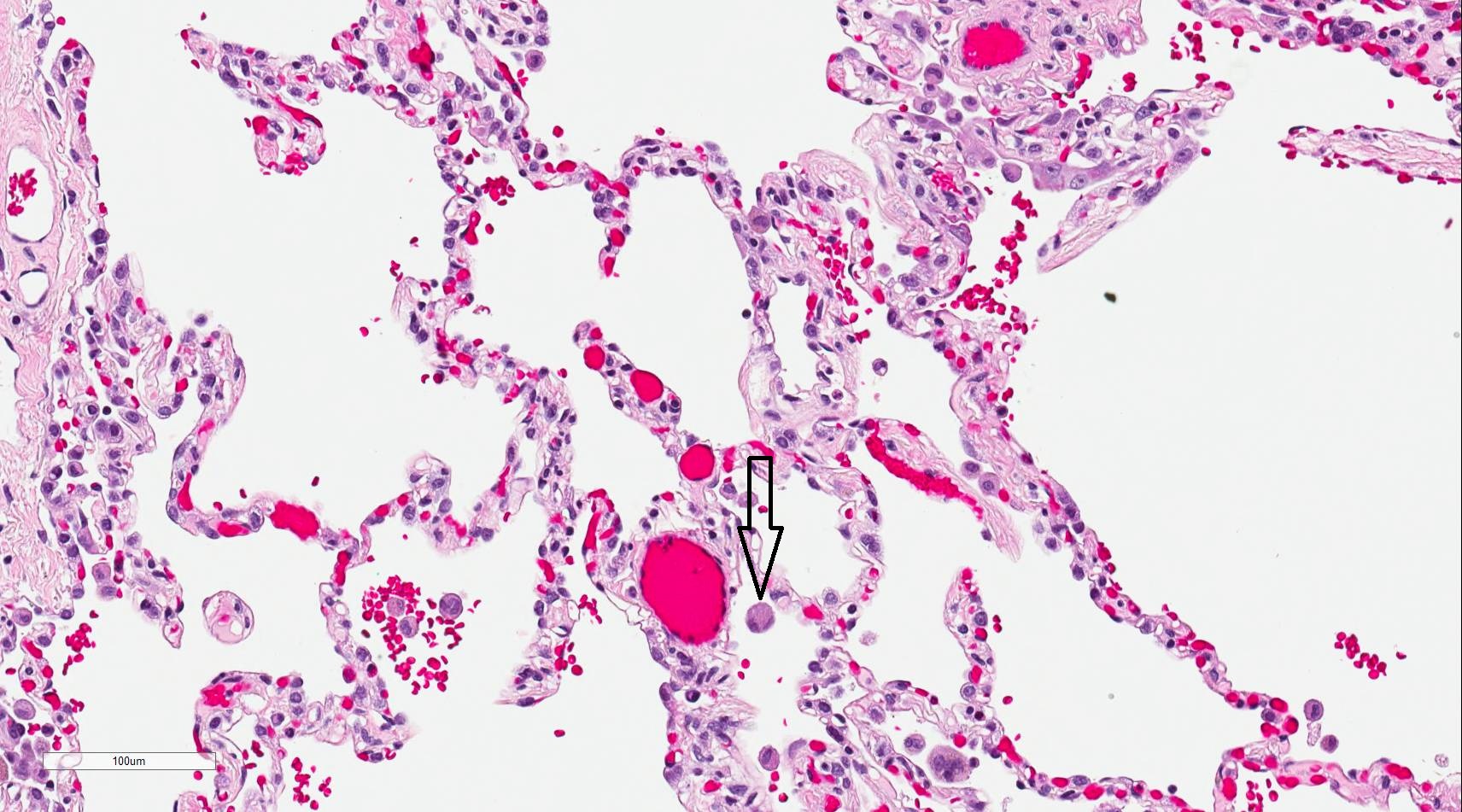
Lung Histology 200× Magnification
Contributed by D Lynch, MD
References
Lambrecht BN. Alveolar macrophage in the driver's seat. Immunity. 2006 Apr:24(4):366-8 [PubMed PMID: 16618595]
Level 3 (low-level) evidenceGuth AM, Janssen WJ, Bosio CM, Crouch EC, Henson PM, Dow SW. Lung environment determines unique phenotype of alveolar macrophages. American journal of physiology. Lung cellular and molecular physiology. 2009 Jun:296(6):L936-46. doi: 10.1152/ajplung.90625.2008. Epub 2009 Mar 20 [PubMed PMID: 19304907]
Level 3 (low-level) evidenceOrkin SH. Diversification of haematopoietic stem cells to specific lineages. Nature reviews. Genetics. 2000 Oct:1(1):57-64. doi: 10.1038/35049577. Epub [PubMed PMID: 11262875]
Level 3 (low-level) evidenceMartinez FO,Gordon S, The M1 and M2 paradigm of macrophage activation: time for reassessment. F1000prime reports. 2014; [PubMed PMID: 24669294]
Mantovani A, Sozzani S, Locati M, Allavena P, Sica A. Macrophage polarization: tumor-associated macrophages as a paradigm for polarized M2 mononuclear phagocytes. Trends in immunology. 2002 Nov:23(11):549-55 [PubMed PMID: 12401408]
Level 3 (low-level) evidenceHance KA, Tataria M, Ziporin SJ, Lee JK, Thompson RW. Monocyte chemotactic activity in human abdominal aortic aneurysms: role of elastin degradation peptides and the 67-kD cell surface elastin receptor. Journal of vascular surgery. 2002 Feb:35(2):254-61 [PubMed PMID: 11854722]
Chalifour A, Jeannin P, Gauchat JF, Blaecke A, Malissard M, N'Guyen T, Thieblemont N, Delneste Y. Direct bacterial protein PAMP recognition by human NK cells involves TLRs and triggers alpha-defensin production. Blood. 2004 Sep 15:104(6):1778-83 [PubMed PMID: 15166032]
Level 3 (low-level) evidenceGulati A,Kaur D,Krishna Prasad GVR,Mukhopadhaya A, PRR Function of Innate Immune Receptors in Recognition of Bacteria or Bacterial Ligands. Advances in experimental medicine and biology. 2018; [PubMed PMID: 30637703]
Level 3 (low-level) evidenceHaque MF, Boonhok R, Prammananan T, Chaiprasert A, Utaisincharoen P, Sattabongkot J, Palittapongarnpim P, Ponpuak M. Resistance to cellular autophagy by Mycobacterium tuberculosis Beijing strains. Innate immunity. 2015 Oct:21(7):746-58. doi: 10.1177/1753425915594245. Epub 2015 Jul 9 [PubMed PMID: 26160686]
Soufleris AJ, Pretlow TP, Bartolucci AA, Pitts AM, MacFadyen AJ, Boohaker EA, Pretlow TG 2nd. Cytologic characterization of pulmonary alveolar macrophages by enzyme histochemistry in plastic. The journal of histochemistry and cytochemistry : official journal of the Histochemistry Society. 1983 Dec:31(12):1412-8 [PubMed PMID: 6631003]
Inoue T, Plieth D, Venkov CD, Xu C, Neilson EG. Antibodies against macrophages that overlap in specificity with fibroblasts. Kidney international. 2005 Jun:67(6):2488-93 [PubMed PMID: 15882296]
Level 3 (low-level) evidenceLe Hir M,Kaissling B, Antibodies against macrophages that overlap in specificity with fibroblasts. Kidney international. 2005 Nov; [PubMed PMID: 16221249]
Level 3 (low-level) evidenceKunz LI, Lapperre TS, Snoeck-Stroband JB, Budulac SE, Timens W, van Wijngaarden S, Schrumpf JA, Rabe KF, Postma DS, Sterk PJ, Hiemstra PS, Groningen Leiden Universities Corticosteroids in Obstructive Lung Disease Study Group. Smoking status and anti-inflammatory macrophages in bronchoalveolar lavage and induced sputum in COPD. Respiratory research. 2011 Mar 22:12(1):34. doi: 10.1186/1465-9921-12-34. Epub 2011 Mar 22 [PubMed PMID: 21426578]
Level 2 (mid-level) evidenceUmemura N, Saio M, Suwa T, Kitoh Y, Bai J, Nonaka K, Ouyang GF, Okada M, Balazs M, Adany R, Shibata T, Takami T. Tumor-infiltrating myeloid-derived suppressor cells are pleiotropic-inflamed monocytes/macrophages that bear M1- and M2-type characteristics. Journal of leukocyte biology. 2008 May:83(5):1136-44. doi: 10.1189/jlb.0907611. Epub 2008 Feb 19 [PubMed PMID: 18285406]
Level 3 (low-level) evidencePeebles RS Jr, Aronica MA. Proinflammatory Pathways in the Pathogenesis of Asthma. Clinics in chest medicine. 2019 Mar:40(1):29-50. doi: 10.1016/j.ccm.2018.10.014. Epub [PubMed PMID: 30691715]
Ufimtseva E,Eremeeva N,Bayborodin S,Umpeleva T,Vakhrusheva D,Skornyakov S, Mycobacterium tuberculosis with different virulence reside within intact phagosomes and inhibit phagolysosomal biogenesis in alveolar macrophages of patients with pulmonary tuberculosis. Tuberculosis (Edinburgh, Scotland). 2019 Jan; [PubMed PMID: 30711161]
Gutierrez MG, Master SS, Singh SB, Taylor GA, Colombo MI, Deretic V. Autophagy is a defense mechanism inhibiting BCG and Mycobacterium tuberculosis survival in infected macrophages. Cell. 2004 Dec 17:119(6):753-66 [PubMed PMID: 15607973]
Level 3 (low-level) evidenceMohan A, Malur A, McPeek M, Barna BP, Schnapp LM, Thomassen MJ, Gharib SA. Transcriptional survey of alveolar macrophages in a murine model of chronic granulomatous inflammation reveals common themes with human sarcoidosis. American journal of physiology. Lung cellular and molecular physiology. 2018 Apr 1:314(4):L617-L625. doi: 10.1152/ajplung.00289.2017. Epub 2017 Dec 6 [PubMed PMID: 29212802]
Level 3 (low-level) evidenceMortaz E, Masjedi MR, Abedini A, Matroodi S, Kiani A, Soroush D, Adcock IM. Common features of tuberculosis and sarcoidosis. International journal of mycobacteriology. 2016 Dec:5 Suppl 1():S240-S241. doi: 10.1016/j.ijmyco.2016.09.031. Epub 2016 Nov 9 [PubMed PMID: 28043581]
Koyama S,Sato E,Haniuda M,Numanami H,Nagai S,Izumi T, Decreased level of vascular endothelial growth factor in bronchoalveolar lavage fluid of normal smokers and patients with pulmonary fibrosis. American journal of respiratory and critical care medicine. 2002 Aug 1; [PubMed PMID: 12153975]
Lee KH, Jeong J, Koo YJ, Jang AH, Lee CH, Yoo CG. Exogenous neutrophil elastase enters bronchial epithelial cells and suppresses cigarette smoke extract-induced heme oxygenase-1 by cleaving sirtuin 1. The Journal of biological chemistry. 2017 Jul 14:292(28):11970-11979. doi: 10.1074/jbc.M116.771089. Epub 2017 Jun 6 [PubMed PMID: 28588027]
Lee KH, Lee J, Jeong J, Woo J, Lee CH, Yoo CG. Cigarette smoke extract enhances neutrophil elastase-induced IL-8 production via proteinase-activated receptor-2 upregulation in human bronchial epithelial cells. Experimental & molecular medicine. 2018 Jul 6:50(7):1-9. doi: 10.1038/s12276-018-0114-1. Epub 2018 Jul 6 [PubMed PMID: 29980681]
Mlika M, Basit H, Kaul P. Alveolar Proteinosis (Archived). StatPearls. 2024 Jan:(): [PubMed PMID: 30725900]