Introduction
Amniotic band syndrome (ABS) comprises various congenital anomalies, which include disruption, deformation, and malformations of organs that were intended to develop normally (see Image. Amniotic Band Syndrome).[1] ABS should be called a sequence rather than a syndrome because the pattern of anomalies in ABS is related to an insult that can result from multiple etiologies. In contrast, a syndrome refers to patterns of congenital anomalies that are known to result from a single etiology (eg, Turner syndrome is due to an XO chromosomal anomaly). Likewise, ABS has many names: amnion rupture sequence, ADAM complex (amniotic deformities/adhesions/mutilations), amniotic band disruption complex, congenital constricting bands, terminal transverse defects, and Streeter anomaly.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
There is no known clear etiology of ABS. However, it is thought that rupture of amnion early in pregnancy results in the development of multiple loose strands (amniotic bands) that adhere to or entangle the fetus.[1][3] Constriction of otherwise normally developing organs results in constriction rings, some severe cases leading to vascular disruption and could potentially result in amputation of the involved anatomic structure. Adherence, even without constriction, can have adverse mechanical effects that result in malformation or deformation. The cause of the rupture of amnion is unknown in most cases.
However, in some cases, iatrogenic invasive procedures like chorionic villus sampling can lead to ABS-like clinical presentation. The aforementioned etiological reasoning does not explain all ABS findings, as in some cases, the affected anatomic structures are internal visceral organs and have histologically intact amniotic lining. In these cases, disruption of fetal blood flow unrelated to bands is thought to be the primary cause. This vascular insult could result from misoprostol exposure in the first trimester and or chorionic villus sampling before 10 weeks of gestation. For a few cases, neither the amniotic band nor vascular disruption is thought to result from a genetic mutation. Almost all ABS cases in twins have been seen in monozygotic twins, suggesting a genetic correlation.[4]
Epidemiology
The estimated incidence of ABS ranges between 1 in 1000 to 1 in 15000 live births and 1 in 70 stillbirths.[5] Both male and female newborns are equally affected. There is no known inheritance pattern. Almost all cases are sporadic, but few examples of familial ABS have been reported, primarily with monozygotic twin gestation.
Pathophysiology
Although not completely understood, as the embryo grows between the amnion and the chorion, the amnion eventually obliterates the extracolonic space. The incomplete obliteration of the extracolonic space may render the amnion fragile and susceptible to rupture. The ruptured amnion could attach itself to body parts, leading to clinical features of ABS. Theories of defective germ plasma and vascular disruption have been proposed to explain the pathophysiology, especially in internal organ cases.
History and Physical
Clinical presentation can be classified into 4 major categories:
- Constrictive rings
- Limb defects
- Neural or spine defects
- Craniofacial defects
Constriction rings and limb or digital amputation are the most common findings, present in at least 80 percent of cases. The amniotic bands may be present, confined to the skin or soft tissue, and extend deep into the tissue. If constriction results in amputation in utero, then the amputated part is usually resorbed and not visible following birth. Limb defects include constriction ring of an extremity with swelling of the distal part, absence of distal portions of 1 or more fingers and toes, especially the central digits, contractures, or fractures. Lower extremities are affected more commonly than the upper, and the thumb is usually spared due to the protection of the palm in utero. While atypical, craniofacial abnormalities, such as encephalocele, facial clefts, and cleft lip/cleft palate, may be present. Spinal defects and scoliosis have also been known to occur with ABS.
Evaluation
Due to the extensive clinical presentation and heterogeneous etiology, diagnosing ABS could be challenging, especially prenatally. If constriction, amputation, or deformation of major anatomic structures are present, ABS can be suspected prenatally as early as the first trimester. Distal limb edema can help make a diagnosis of ABS prenatally. In very few cases, a strand of amniotic fibrous tissue could be seen attached to tissues and restricting the free movement of the fetus in utero. Postnatally, ABS should be suspected in newborns with visible constrictions, amputations, non-midline, and unusually located craniofacial or body wall defects. Investigating the fresh fetal membranes and placenta is important in cases where amniotic bands are absent in newborns.
Treatment / Management
There are no set guidelines for the management of ABS when diagnosed prenatally. Regardless of the therapeutic approach chosen, all patients should receive counseling about fetal abnormalities detected and the possibility of other hidden abnormalities. For chromosomal microarray, amniocentesis indicates if the results affect pregnancy decision-making. Consulting with concerned subspecialists is ideally recommended. In cases of lethal anomalies, post-natal palliative care should also be a topic of discussion. The in-utero intervention of amniotic band lysis can potentially slow the progression of constriction effects and restore normal flow to the downstream structures. There is a hypothesis that fetal limb recovery is more likely after fetal intervention than postnatal recovery because of the plasticity of tissue healing during fetal life. Although fetoscopic intervention may restore blood flow and save the limb, plastic surgery may still be necessary after birth. However, the efficacy of this intervention is unknown, as there are no set criteria for the selection of candidates and a lack of clinical studies.[6] There are no standard guidelines for the management of pregnancy complicated with fetal ABS. Follow-up, ultrasound, and intervention are individually tailored and depend on the severity of ABS complications.[7] Postnatal management includes a thorough physical exam and, if needed, imaging studies to clearly describe the extent of ABS. Relief of constriction rings postnatally may help salvage some limb function by relieving venous pressure. Vascular comprise diagnosed postnatally may require urgent surgical intervention.(B2)
Differential Diagnosis
Differential diagnosis of amniotic bands divides into 2 main groups.
- Uterus and placental anomalies:
- Synechiae and septa—Uterine synechiae are intrauterine adhesions typically resulting from a previous intrauterine surgical site or infection. Uterine septa are congenital malformations. Synechiae and septa do not restrict fetal movement and are not associated with fetal anomalies like ABS.
- Residual gestational sac - A residual gestational sac left after the death of the fetus in case of twin pregnancy.
- Circumvallate placenta - Circumvallate placenta refers to a placenta with an unusually small chorionic plate but with the growth of extracranial placental tissue, which also does not restrict fetal movement and does not cause ABS.
2. Limb Amputations - there are other causes of congenital absence of limbs:
- Syndromes and teratogens—Numerous syndromes have associated congenital limb anomalies. An example is absent thumb and radius syndrome. Some of the limb anomalies could also be due to teratogenic substances.
Prognosis
The prognosis of a newborn affected by ABS depends on the extent of the defects, from minor cosmetic defects to the lethal involvement of vital organs.
Complications
ABS carries correlations with miscarriages, preterm, and stillbirths.
Deterrence and Patient Education
ABS is a highly variable spectrum of anomalies affecting various anatomical structures during fetal life.[8] Etiology is multifactorial with multiple proposed mechanisms; the most widely accepted theories include amniotic band attachment, vascular disruption, and rare genetic mutation. There are 4 main categories of anatomical defects – constriction rings, limb defects, spine/neural defects, and craniofacial defects. It is diagnosable prenatally. The extent of ABS and severity of the defect dictates the care of pregnant mothers, as there are no clear published guidelines. In-utero lysis of amniotic bands can salvage limb function, but no patient selection guidelines exist. Postnatal treatment involves the release of constricting rings, if possible, to save the distal limb. ABS can also lead to lethal deformation of vital internal organs in rare cases.
Enhancing Healthcare Team Outcomes
Management of ABS begins with early fetal diagnosis and collaboration between obstetrics, neonatal-perinatal specialists, and maternal-fetal medicine specialists; this may help achieve the best outcome for individual patients. Management of newborns affected by ABS requires careful examination and interprofessional team involvement. There is a lack of strong evidence for any particular approach. Consult with a pediatric general surgeon, orthopedic surgeon, or craniofacial surgeon may be needed depending on the anatomical structure involved. Nurses monitoring these infants must constantly monitor for pulses, warmth, and cyanosis and report any deviation from normal to the attending physician and specialists on the team. Specialized neonatal inpatient nurses should assist the clinician in educating the parents about the patient's care. While extremity constriction may be easy to visualize, if the bands involve the chest, abdomen, or neck, one may require imaging studies, which would include a radiologist.
Lastly, parents should receive counseling from the nursing and clinical interprofessional team that most ABS cases are sporadic with no known re-occurrence risk unless in cases of familial ABS. In instances of cosmetic deformity, psychological counseling may also be necessary for the patients or their families. ABS requires an interprofessional team approach, including physicians, specialists, specialty-trained nurses, and counselors, collaborating across disciplines to achieve optimal patient results.
Media
(Click Image to Enlarge)
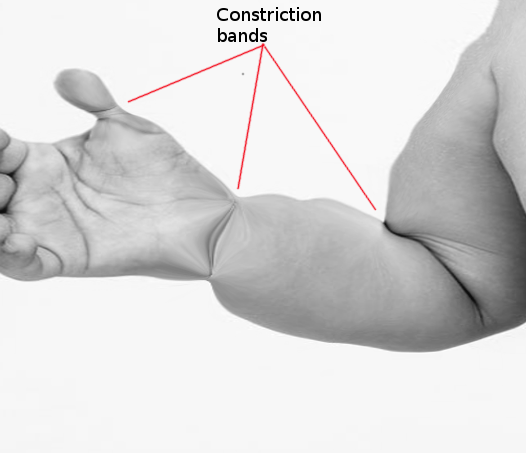
Amniotic Band Syndrome
Contributed by O Chaigasame, MD
References
Seeds JW, Cefalo RC, Herbert WN. Amniotic band syndrome. American journal of obstetrics and gynecology. 1982 Oct 1:144(3):243-8 [PubMed PMID: 7124837]
Singh AP, Gorla SR. Amniotic Band Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 31424867]
Daya M, Makakole M. Congenital vascular anomalies in amniotic band syndrome of the limbs. Journal of pediatric surgery. 2011 Mar:46(3):507-13. doi: 10.1016/j.jpedsurg.2010.09.006. Epub [PubMed PMID: 21376201]
Koskimies E, Syvänen J, Nietosvaara Y, Mäkitie O, Pakkasjärvi N. Congenital constriction band syndrome with limb defects. Journal of pediatric orthopedics. 2015 Jan:35(1):100-3. doi: 10.1097/BPO.0000000000000206. Epub [PubMed PMID: 24787313]
Kalousek DK, Bamforth S. Amnion rupture sequence in previable fetuses. American journal of medical genetics. 1988 Sep:31(1):63-73 [PubMed PMID: 3223500]
Javadian P, Shamshirsaz AA, Haeri S, Ruano R, Ramin SM, Cass D, Olutoye OO, Belfort MA. Perinatal outcome after fetoscopic release of amniotic bands: a single-center experience and review of the literature. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2013 Oct:42(4):449-55. doi: 10.1002/uog.12510. Epub [PubMed PMID: 23671033]
Level 3 (low-level) evidenceGueneuc A, Chalouhi GE, Borali D, Mediouni I, Stirnemann J, Ville Y. Fetoscopic Release of Amniotic Bands Causing Limb Constriction: Case Series and Review of the Literature. Fetal diagnosis and therapy. 2019:46(4):246-256. doi: 10.1159/000495505. Epub 2019 Feb 6 [PubMed PMID: 30726851]
Level 2 (mid-level) evidenceBrown DL, Felker RE, Emerson DS. Intrauterine shelves in pregnancy: sonographic observations. AJR. American journal of roentgenology. 1989 Oct:153(4):821-4 [PubMed PMID: 2672739]