Indications
Angiotensin-converting enzyme inhibitors (ACEIs) are the most commonly indicated medications in the treatment of cardiovascular and renal diseases, including heart failure, acute coronary syndrome, nephrotic syndrome, diabetes, and hypertension.[1]
Hypertension
Angiotensin-converting enzyme inhibitors effectively lower the mean arterial blood pressure as well as systolic and diastolic blood pressure both in hypertensive and normotensive subjects.[2][3] Angiotensin-converting enzyme inhibitors have been evaluated as antihypertensive drugs in multiple randomized controlled trials.[4] In 2014, the Eighth Joint National Commission (JNC8) published evidence-based guidelines for treating high blood pressure in adults, which recommended that ACE inhibitors are one of four drug classes recommended for initial therapy for adults with elevated blood pressure.[5] The other three classes of drugs are calcium channel blockers, thiazide diuretics, and angiotensin receptor blockers, which are useful as initial therapy for the general nonblack population. Only thiazide and calcium channel blockers are recommended as initial therapy for the general black population with elevated blood pressure.[6] Recent guidelines released by the American Heart Association/American College of Cardiology (AHA/ACC) and the European Society of Cardiology (ESC) also recommend ACE inhibitors as first-line antihypertensive therapy, especially in patients with diabetes mellitus and cardiovascular diseases.[7][8] Although ACE inhibitors are generally very effective antihypertensive drugs, they have been proven to be less effective in hypertensive Black race individuals than in whites in clinical practice.[9]
Heart Failure
Angiotensin-converting enzyme inhibitors (ACEIs) improve heart failure by decreasing afterload, preload, and systolic wall stress, which results in increased cardiac output without any increase in heart rate.[10][11] ACE inhibitors play an important role in promoting salt excretion by augmenting the renal blood flow and reducing aldosterone and antidiuretic hormone production. Apart from decreasing the afterload, ACEIs also reduce cardiac myocyte hypertrophy. Since the 1980s, several large, prospective, randomized, placebo-controlled trials have proved that treatment with ACE inhibitors reduces overall mortality, especially in patients with heart failure with reduced ejection fraction (0HFrEF).[12][13][14] These trials demonstrated that ACE inhibitors reduce mortality even in asymptomatic patients with left ventricular dysfunction.[15] Based on the above-mentioned evidence, ACE inhibitors are strongly recommended as first-choice therapy in patients with heart failure.[16][17]
Post Myocardial Infarction
Over the last few decades, several prospective, randomized trials have studied the effect of ACE inhibitors on mortality after myocardial infarction (MI).[18][19] The vast majority of these trials have shown a significant decrease in mortality and a slowing of the progression to congestive heart failure after MI in patients treated with ACE inhibitors.[20] The clinical practice guidelines in the contemporary era recommend that patients with left ventricular dysfunction or heart failure be treated with ACE inhibitors without delay after infarction. It is also recommended that all patients should be treated with ACE inhibitors initially, with a review of the need for continuation later based on left ventricular function assessment.[21]
Diabetes
The Renin-Angiotensin-Aldosterone system and increased glomerular capillary pressure have been reported to increase the progression of renal dysfunction due to diabetes mellitus related nephropathy.[22] A large, prospective, randomized, placebo-controlled has demonstrated that ACE inhibitors slow down the progression of nephropathy in patients with insulin-dependent diabetes mellitus and significantly reduce the combined endpoints of dialysis, transplantation, and death.[23] Current recommendations are using ACEi or ARB as first-line therapy for hypertension in patients with a history of diabetes. Also, the use of ACEi in diabetic hypertensive patients with no history of coronary heart disease has been shown to decrease the incidence of myocardial infarction and improve heart function.[24]
Nephrotic Syndrome or Proteinuria
Angiotensin-converting enzyme inhibitors have been reported to decrease glomerular capillary pressure by decreasing arterial pressure and selectively dilating efferent arterioles.[25] It has been shown that the use of ACE inhibitors prevents the progression of microalbuminuria to overt proteinuria.[26] Angiotensin-converting enzyme inhibition provides long-term protection against the development and progression of proteinuria and stabilizes renal function in previously untreated patients with impaired renal function.[26]
Chronic Kidney Disease
ACE inhibitors or ARBs are the first-line drugs in managing chronic kidney disease (CKD) patients. The use of ACEI or ARB has been proven to have a superior effect compared to placebo treatment on decreasing proteinuria and slowing kidney disease progression. The efficacy of ACEI and ARB is comparable.[27]
Glomerular Disease and Post-transplant Glomerulonephritis\
The use of ACE inhibitors or ARB is the mainstay of treatment in patients with glomerular diseases. It slows down the decline in glomerular filtration rate (GFR) and proteinuria.[28] The use of renin-angiotensin-aldosterone inhibitors prolongs graft survival in patients with post-transplant glomerulonephritis.[29]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Angiotensin II causes direct vasoconstriction of precapillary arterioles and postcapillary venules, inhibits the reuptake of norepinephrine, stimulates the release of catecholamines from the adrenal medulla, reduces urinary excretion of sodium and water, stimulates synthesis and release of aldosterone, and stimulates hypertrophy of both vascular smooth muscle cells and cardiac myocytes.[30][31]
The exact mechanism of ACE inhibitors is not fully known. They interfere with the renin-angiotensin-aldosterone system, but their effect is not directly related to renin levels in the blood. As the name implies, ACE inhibitors block an angiotensin-converting enzyme that converts angiotensin I to angiotensin II. Decreased production of angiotensin II enhances natriuresis, lowers blood pressure, and prevents remodeling of smooth muscle and cardiac myocytes. Lowered arterial and venous pressure reduces preload and afterload. Also, the hypothesis is that ACE inhibitors interfere with the degradation of bradykinin, a peptide that causes vasodilation.[32]
Angiotensin-converting enzyme regulates the balance between the vasodilatory and natriuretic properties of bradykinin and the vasoconstrictive and salt-retentive properties of Angiotensin II. ACE inhibitors alter this balance by decreasing the formation of Angiotensin II and the degradation of bradykinin. ACE inhibitors also alter the formation and degradation of several other vasoactive substances, such as substance P, but the contribution of these compounds to the therapeutic or adverse effects of ACE inhibitors is uncertain.[33]
Administration
ACE inhibitors differ in their chemical structure, potency, bioavailability, plasma half-life, route of elimination, as well as their distribution and affinity for tissue-bound angiotensin-converting-enzyme.
Depending on the chemical structure, ACE inhibitors are classified into three groups.[34][35]
Sulfhydryl-containing ACE inhibitors
- Captopril – Hypertension therapy is 25 mg, either BID or TID, with a maximum of 450 mg. Heart failure therapy is 6.25 mg TID, with a maximum of 450 mg.
Dicarboxylic-containing ACE inhibitors: see table.
Phosphorus-containing ACE inhibitor.
- Fosinopril – Hypertension therapy dosing is 10 mg, increasing to a maximum dose of 80 mg. May split into two equal doses during the day to control blood pressure. Heart failure therapy is 5 to 10 mg daily to a maximum dose of 40 mg.
General Dosing Information
All of the ACE inhibitors are prescribed orally, except for enalapril, which can be given intravenously. Enalapril's IV dosage is initially 0.625 to 1.25 mg every 6 hours. Dosage titration up can be to 5 mg IV every 6 hours. Geriatric dosing should definitely initiate at the lower end of the adult dosing regimen.
There should be a dosage decrease in patients with heart failure, salt-depleted patients, and/or renal impairment.
Lisinopril and captopril are the only ACE inhibitors that do not have to be activated in the body to be effective. All the other ACE inhibitors are prodrugs and require activation. Most reach peak serum levels within 1 hour after ingestion. Since most of the activation occurs in the liver, a non-prodrug form is preferable in patients with underlying liver issues.[36]
Adverse Effects
About 1 to 10% will develop a dry, nonproductive paroxysmal cough, and there is no treatment for the cough.[37][38] Experimental studies have shown that using non-steroidal anti-inflammatory agents (NSAIDs) and intermediate-dose aspirin (500 mg) can help with ACE inhibitors induced cough.[39] ACE inhibitor-induced cough is reported more frequently among women than men.[40] The cough is usually dry, and it often requires cessation of therapy.
Angioedema is the most significant adverse effect of ACEi. It can affect any part of the body, including the intestine, but the most concerning is edema of the tongue, glottis, and/or larynx, causing airway obstruction.[41] Angioedema has a higher rate of incidence in the African-American population. When airway compromise is present, the treatment always secures the airway with an endotracheal tube that allows ventilation until the edema resolves. Multiple treatments have been tried, such as diphenhydramine, methylprednisolone, and epinephrine. Also, fresh frozen plasma and the newer agents, bradykinin blocking agents, have been tried. There are case reports that these bradykinin blocking agents might improve angioedema, but no literature exists proving that they are better than the other agents.[42] There is an ongoing phase III trial at this time.
Life-threatening anaphylactoid reactions have occurred in patients receiving Hymenoptera venom desensitization treatment and patients receiving dialysis with high-flux membranes. Treatment includes diphenhydramine, epinephrine, and blood pressure support with fluids and catecholamines.[43][44]
Angiotensin-converting enzyme inhibitors have been reported to cause a reversible decline in renal function. Those with heart failure who depend on the renin-angiotensin-aldosterone system may develop changes in renal function with the use of ACE inhibitors.[45] Also, about one-fifth of the patients with renal artery stenosis develop increases in blood urea nitrogen and creatinine.[46] Any patient who already has a renal insufficiency is susceptible to a worsening of renal function. The renal function requires monitoring during treatment for susceptible groups.[47]
As with any medication that lowers blood pressure, hypotension is an adverse reaction. Those at risk for this side effect: heart failure with systolic blood pressure below 100 mmHg, ischemic heart disease, cerebrovascular disease, hyponatremia, high dose diuretic therapy, renal dialysis, or severe volume and/or sodium depletion.[48]
ACE inhibitors may cause hyperkalemia. Those at risk for this side effect: prior history of renal impairment and/or diabetes, simultaneous use of potassium-sparing diuretics, and/or potassium supplements.[49] Treatment depends upon the potassium level, EKG changes, and whether the patient still has kidney function and produces urine.[47] There has been one report of increased sudden death in patients taking ACE inhibitors and co-trimoxazole simultaneously. The mechanism is believed to be hyperkalemia.[50]
Cholestatic jaundice or hepatitis is another rare but serious adverse effect that can progress to hepatic necrosis and sometimes death. The clinician needs to discontinue the drug, and the patient managed appropriately.[51]
Contraindications
ACE inhibitors are contraindicated in patients with a history of angioedema or hypersensitivity related to treatment with an ACE inhibitor and those with hereditary or idiopathic angioedema.[52]
These drugs should not be given to patients already taking a direct renin inhibitor such as aliskiren.
ACE inhibitors should not be given during pregnancy. They were Category D in pregnancy under the old FDA system because it is known to cause skull hypoplasia, anuria, hypotension, renal failure, lung hypoplasia, skeletal deformations, oligohydramnios, and death.[53]
The combination therapy of ACEi and ARBs does not reduce mortality in patients with heart failure compared to monotherapy. In fact, the combination therapy can worsen renal indices and cause life-threatening hyperkalemia.[54]
Monitoring
Renal function and electrolytes need to be checked regularly due to the effects of the drug on the renin-angiotensin-aldosterone system. For patients with increasing potassium, drop-in GFR, or increasing creatinine, the drug needs to be adjusted accordingly or discontinued.[55]
Toxicity
Excessive doses of ACE inhibitors are usually well-tolerated, but they can cause hypotension, drop-in GFR, and electrolyte derangements. In addition, since ACE inhibitors block aldosterone, they can cause hyperkalemia and hyponatremia.[56][57]
If the patient presents within 1 hour of ingestion and is awake and able to protect their airway, activated charcoal can be given. If they remain asymptomatic for 6 hours of observation, they can be considered medically stable for either discharge or referral to psychiatry.[58]
For those with hypotension, fluids should be the first line of therapy. There is no antidote for ACE inhibitor poisoning. Naloxone has been used in captopril overdoses in the past with some success and can be a choice if intravenous fluids are not successful. Also, vasopressors are an option for the treatment of hypotension.[59]
Enhancing Healthcare Team Outcomes
ACE inhibitors are one of the most widely used drugs for hypertension and heart failure, but their popularity does not mean they do not require the management of an interprofessional team. Besides nephrologists and cardiologists, these drugs are widely prescribed by nurse practitioners and primary care providers. While ACE inhibitors are relatively safe, a pharmacist should examine the patient's medication record to verify dosing and check for drug-drug interactions. Nursing can provide patient counsel, monitor for interactions and adverse events, and report any issues to the prescriber. It is important to monitor renal function and levels of electrolytes regularly.[60] Because many ACE inhibitors are currently available, it is important to keep up with the guidelines and recommendations, and the pharmacist can help the prescriber in this area.[61] An interprofessional team approach will optimize ACE inhibitor therapy resulting in improved patient outcomes. [Level 5]
Media
(Click Image to Enlarge)
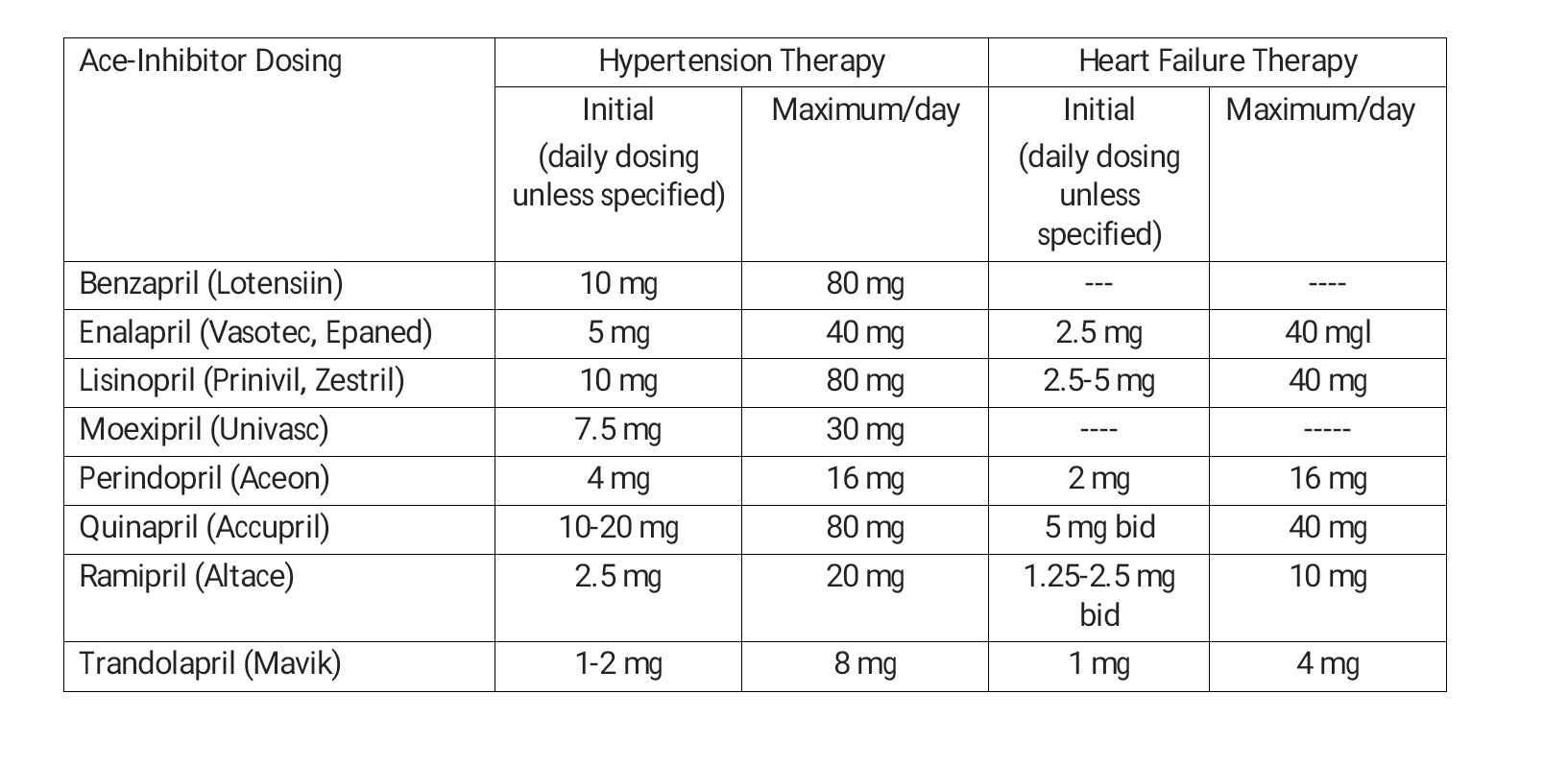
Dicarboxyl-containing ACE inhibitors and doses Contributed by Linda L Herman
References
Nasution SA. The use of ACE inhibitor in cardiovascular disease. Acta medica Indonesiana. 2006 Jan-Mar:38(1):60-4 [PubMed PMID: 16479034]
Vidt DG, Bravo EL, Fouad FM. Drug therapy. Captopril. The New England journal of medicine. 1982 Jan 28:306(4):214-9 [PubMed PMID: 7033784]
Level 3 (low-level) evidenceTodd PA, Heel RC. Enalapril. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in hypertension and congestive heart failure. Drugs. 1986 Mar:31(3):198-248 [PubMed PMID: 3011386]
Messerli FH, Bangalore S, Bavishi C, Rimoldi SF. Angiotensin-Converting Enzyme Inhibitors in Hypertension: To Use or Not to Use? Journal of the American College of Cardiology. 2018 Apr 3:71(13):1474-1482. doi: 10.1016/j.jacc.2018.01.058. Epub [PubMed PMID: 29598869]
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014 Feb 5:311(5):507-20. doi: 10.1001/jama.2013.284427. Epub [PubMed PMID: 24352797]
Level 1 (high-level) evidencePage MR. The JNC 8 hypertension guidelines: an in-depth guide. The American journal of managed care. 2014 Jan:20(1 Spec No.):E8 [PubMed PMID: 25618230]
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2018 May 15:71(19):e127-e248. doi: 10.1016/j.jacc.2017.11.006. Epub 2017 Nov 13 [PubMed PMID: 29146535]
Level 3 (low-level) evidenceWilliams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I, ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. European heart journal. 2018 Sep 1:39(33):3021-3104. doi: 10.1093/eurheartj/ehy339. Epub [PubMed PMID: 30165516]
Veterans Administration Co-Operative Study Group on Antihypertensive Agents. Racial differences in response to low-dose captopril are abolished by the addition of hydrochlorothiazide. British journal of clinical pharmacology. 1982:14 Suppl 2(Suppl 2):97S-101S [PubMed PMID: 6753911]
Level 1 (high-level) evidenceGavras H, Faxon DP, Berkoben J, Brunner HR, Ryan TJ. Angiotensin converting enzyme inhibition in patients with congestive heart failure. Circulation. 1978 Nov:58(5):770-6 [PubMed PMID: 699246]
Dzau VJ, Colucci WS, Williams GH, Curfman G, Meggs L, Hollenberg NK. Sustained effectiveness of converting-enzyme inhibition in patients with severe congestive heart failure. The New England journal of medicine. 1980 Jun 19:302(25):1373-9 [PubMed PMID: 6246425]
CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The New England journal of medicine. 1987 Jun 4:316(23):1429-35 [PubMed PMID: 2883575]
Level 1 (high-level) evidenceSOLVD Investigators, Yusuf S, Pitt B, Davis CE, Hood WB, Cohn JN. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The New England journal of medicine. 1991 Aug 1:325(5):293-302 [PubMed PMID: 2057034]
Level 1 (high-level) evidence. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators. Lancet (London, England). 1993 Oct 2:342(8875):821-8 [PubMed PMID: 8104270]
Level 1 (high-level) evidencePfeffer MA, Braunwald E, Moyé LA, Basta L, Brown EJ Jr, Cuddy TE, Davis BR, Geltman EM, Goldman S, Flaker GC. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. The New England journal of medicine. 1992 Sep 3:327(10):669-77 [PubMed PMID: 1386652]
Level 1 (high-level) evidenceYancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Colvin MM, Drazner MH, Filippatos GS, Fonarow GC, Givertz MM, Hollenberg SM, Lindenfeld J, Masoudi FA, McBride PE, Peterson PN, Stevenson LW, Westlake C. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017 Aug 8:136(6):e137-e161. doi: 10.1161/CIR.0000000000000509. Epub 2017 Apr 28 [PubMed PMID: 28455343]
Level 3 (low-level) evidencePonikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European heart journal. 2016 Jul 14:37(27):2129-2200. doi: 10.1093/eurheartj/ehw128. Epub 2016 May 20 [PubMed PMID: 27206819]
Swedberg K, Held P, Kjekshus J, Rasmussen K, Rydén L, Wedel H. Effects of the early administration of enalapril on mortality in patients with acute myocardial infarction. Results of the Cooperative New Scandinavian Enalapril Survival Study II (CONSENSUS II). The New England journal of medicine. 1992 Sep 3:327(10):678-84 [PubMed PMID: 1495520]
Level 1 (high-level) evidenceAmbrosioni E, Borghi C, Magnani B. The effect of the angiotensin-converting-enzyme inhibitor zofenopril on mortality and morbidity after anterior myocardial infarction. The Survival of Myocardial Infarction Long-Term Evaluation (SMILE) Study Investigators. The New England journal of medicine. 1995 Jan 12:332(2):80-5 [PubMed PMID: 7990904]
Level 1 (high-level) evidencePfeffer MA. Left ventricular remodeling after acute myocardial infarction. Annual review of medicine. 1995:46():455-66 [PubMed PMID: 7598478]
O'Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX, Anderson JL, Jacobs AK, Halperin JL, Albert NM, Brindis RG, Creager MA, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Kushner FG, Ohman EM, Stevenson WG, Yancy CW, American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Jan 29:127(4):e362-425. doi: 10.1161/CIR.0b013e3182742cf6. Epub 2012 Dec 17 [PubMed PMID: 23247304]
Level 3 (low-level) evidenceIchikawa I, Brenner BM. Glomerular actions of angiotensin II. The American journal of medicine. 1984 May 31:76(5B):43-9 [PubMed PMID: 6203406]
Level 3 (low-level) evidenceLewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. The New England journal of medicine. 1993 Nov 11:329(20):1456-62 [PubMed PMID: 8413456]
Level 1 (high-level) evidenceZhang Y, Ding X, Hua B, Liu Q, Chen H, Zhao XQ, Li W, Li H. Real-world use of ACEI/ARB in diabetic hypertensive patients before the initial diagnosis of obstructive coronary artery disease: patient characteristics and long-term follow-up outcome. Journal of translational medicine. 2020 Apr 1:18(1):150. doi: 10.1186/s12967-020-02314-y. Epub 2020 Apr 1 [PubMed PMID: 32238168]
Anderson S, Rennke HG, Brenner BM. Therapeutic advantage of converting enzyme inhibitors in arresting progressive renal disease associated with systemic hypertension in the rat. The Journal of clinical investigation. 1986 Jun:77(6):1993-2000 [PubMed PMID: 3011863]
Level 3 (low-level) evidenceRavid M, Lang R, Rachmani R, Lishner M. Long-term renoprotective effect of angiotensin-converting enzyme inhibition in non-insulin-dependent diabetes mellitus. A 7-year follow-up study. Archives of internal medicine. 1996 Feb 12:156(3):286-9 [PubMed PMID: 8572838]
Level 1 (high-level) evidenceSilvariño R, Rios P, Baldovinos G, Chichet MA, Perg N, Sola L, Saona G, De Souza N, Lamadrid V, Gadola L. Is Chronic Kidney Disease Progression Influenced by the Type of Renin-Angiotensin-System Blocker Used? Nephron. 2019:143(2):100-107. doi: 10.1159/000500925. Epub 2019 Jun 14 [PubMed PMID: 31203280]
Rigat B, Hubert C, Alhenc-Gelas F, Cambien F, Corvol P, Soubrier F. An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. The Journal of clinical investigation. 1990 Oct:86(4):1343-6 [PubMed PMID: 1976655]
Pazik J, Ostrowska J, Lewandowski Z, Mróz A, Perkowska-Ptasińska A, Baczkowska T, Durlik M. Renin-Angiotensin-Aldosterone system inhibitors and statins prolong graft survival in post-transplant glomerulonephritis. Annals of transplantation. 2008:13(4):41-5 [PubMed PMID: 19034222]
FOLKOW B, JOHANSSON B, MELLANDER S. The comparative effects of angiotensin and noradrenaline on consecutive vascular sections. Acta physiologica Scandinavica. 1961 Oct:53():99-104 [PubMed PMID: 13893844]
Level 2 (mid-level) evidenceBell L, Madri JA. Influence of the angiotensin system on endothelial and smooth muscle cell migration. The American journal of pathology. 1990 Jul:137(1):7-12 [PubMed PMID: 2164777]
Level 3 (low-level) evidenceTimmermans PB, Wong PC, Chiu AT, Herblin WF, Benfield P, Carini DJ, Lee RJ, Wexler RR, Saye JA, Smith RD. Angiotensin II receptors and angiotensin II receptor antagonists. Pharmacological reviews. 1993 Jun:45(2):205-51 [PubMed PMID: 8372104]
Level 3 (low-level) evidenceCascieri MA, Bull HG, Mumford RA, Patchett AA, Thornberry NA, Liang T. Carboxyl-terminal tripeptidyl hydrolysis of substance P by purified rabbit lung angiotensin-converting enzyme and the potentiation of substance P activity in vivo by captopril and MK-422. Molecular pharmacology. 1984 Mar:25(2):287-93 [PubMed PMID: 6199659]
Level 3 (low-level) evidenceSpyroulias GA, Galanis AS, Pairas G, Manessi-Zoupa E, Cordopatis P. Structural features of angiotensin-I converting enzyme catalytic sites: conformational studies in solution, homology models and comparison with other zinc metallopeptidases. Current topics in medicinal chemistry. 2004:4(4):403-29 [PubMed PMID: 14965309]
Regulski M, Regulska K, Stanisz BJ, Murias M, Gieremek P, Wzgarda A, Niznik B. Chemistry and pharmacology of Angiotensin-converting enzyme inhibitors. Current pharmaceutical design. 2015:21(13):1764-75 [PubMed PMID: 25388457]
Williams B. Drug discovery in renin-angiotensin system intervention: past and future. Therapeutic advances in cardiovascular disease. 2016 Jun:10(3):118-25. doi: 10.1177/1753944716642680. Epub 2016 Apr 27 [PubMed PMID: 27126389]
Level 3 (low-level) evidencePinargote P, Guillen D, Guarderas JC. ACE inhibitors: upper respiratory symptoms. BMJ case reports. 2014 Jul 17:2014():. doi: 10.1136/bcr-2014-205462. Epub 2014 Jul 17 [PubMed PMID: 25035451]
Level 3 (low-level) evidenceIsraili ZH, Hall WD. Cough and angioneurotic edema associated with angiotensin-converting enzyme inhibitor therapy. A review of the literature and pathophysiology. Annals of internal medicine. 1992 Aug 1:117(3):234-42 [PubMed PMID: 1616218]
Tenenbaum A, Grossman E, Shemesh J, Fisman EZ, Nosrati I, Motro M. Intermediate but not low doses of aspirin can suppress angiotensin-converting enzyme inhibitor-induced cough. American journal of hypertension. 2000 Jul:13(7):776-82 [PubMed PMID: 10933569]
Os I, Bratland B, Dahlöf B, Gisholt K, Syvertsen JO, Tretli S. Female sex as an important determinant of lisinopril-induced cough. Lancet (London, England). 1992 Feb 8:339(8789):372 [PubMed PMID: 1346451]
Level 3 (low-level) evidenceSlater EE, Merrill DD, Guess HA, Roylance PJ, Cooper WD, Inman WH, Ewan PW. Clinical profile of angioedema associated with angiotensin converting-enzyme inhibition. JAMA. 1988 Aug 19:260(7):967-70 [PubMed PMID: 2840522]
Korzeniowska K, Cielewiczi A, Pawlaczyk M, Motowidlo K, Andrys-Wawrzyniak I, Jablecka A. ANGIOEDEMA AFTER ANGIOTENSIN-CONVERTING ENZYME INHIBITORS. Acta poloniae pharmaceutica. 2017 May:74(3):983-986 [PubMed PMID: 29513968]
Tunon-de-Lara JM, Villanueva P, Marcos M, Taytard A. ACE inhibitors and anaphylactoid reactions during venom immunotherapy. Lancet (London, England). 1992 Oct 10:340(8824):908 [PubMed PMID: 1357311]
Level 3 (low-level) evidenceRousaud Baron F, Garcia JM, Camps EM, Cubells TD, Comamala MR. ACE inhibitors and anaphylactoid reactions to high-flux membrane dialysis (AN69): clinical aspects. Nephron. 1992:60(4):487 [PubMed PMID: 1584327]
Level 3 (low-level) evidenceMurphy BF, Whitworth JA, Kincaid-Smith P. Renal insufficiency with combinations of angiotensin converting enzyme inhibitors and diuretics. British medical journal (Clinical research ed.). 1984 Mar 17:288(6420):844-5 [PubMed PMID: 6322905]
Level 3 (low-level) evidenceKhosla S, Ahmed A, Siddiqui M, Trivedi A, Benatar D, Salem Y, Elbzour M, Vidyarthi V, Lubell D. Safety of angiotensin-converting enzyme inhibitors in patients with bilateral renal artery stenosis following successful renal artery stent revascularization. American journal of therapeutics. 2006 Jul-Aug:13(4):306-8 [PubMed PMID: 16858164]
Level 2 (mid-level) evidenceRosano GMC, Tamargo J, Kjeldsen KP, Lainscak M, Agewall S, Anker SD, Ceconi C, Coats AJS, Drexel H, Filippatos G, Kaski JC, Lund L, Niessner A, Ponikowski P, Savarese G, Schmidt TA, Seferovic P, Wassmann S, Walther T, Lewis BS. Expert consensus document on the management of hyperkalaemia in patients with cardiovascular disease treated with renin angiotensin aldosterone system inhibitors: coordinated by the Working Group on Cardiovascular Pharmacotherapy of the European Society of Cardiology. European heart journal. Cardiovascular pharmacotherapy. 2018 Jul 1:4(3):180-188. doi: 10.1093/ehjcvp/pvy015. Epub [PubMed PMID: 29726985]
Level 3 (low-level) evidenceHodsman GP, Isles CG, Murray GD, Usherwood TP, Webb DJ, Robertson JI. Factors related to first dose hypotensive effect of captopril: prediction and treatment. British medical journal (Clinical research ed.). 1983 Mar 12:286(6368):832-4 [PubMed PMID: 6403103]
Level 3 (low-level) evidenceBurnakis TG, Mioduch HJ. Combined therapy with captopril and potassium supplementation. A potential for hyperkalemia. Archives of internal medicine. 1984 Dec:144(12):2371-2 [PubMed PMID: 6391404]
Perazella MA. Hyperkalemia and trimethoprim-sulfamethoxazole: a new problem emerges 25 years later. Connecticut medicine. 1997 Aug:61(8):451-8 [PubMed PMID: 9309892]
Level 3 (low-level) evidenceRahmat J, Gelfand RL, Gelfand MC, Winchester JF, Schreiner GE, Zimmerman HJ. Captopril-associated cholestatic jaundice. Annals of internal medicine. 1985 Jan:102(1):56-8 [PubMed PMID: 3881069]
Level 3 (low-level) evidenceBrown NJ, Ray WA, Snowden M, Griffin MR. Black Americans have an increased rate of angiotensin converting enzyme inhibitor-associated angioedema. Clinical pharmacology and therapeutics. 1996 Jul:60(1):8-13 [PubMed PMID: 8689816]
Level 2 (mid-level) evidenceQuan A. Fetopathy associated with exposure to angiotensin converting enzyme inhibitors and angiotensin receptor antagonists. Early human development. 2006 Jan:82(1):23-8 [PubMed PMID: 16427219]
Kuenzli A, Bucher HC, Anand I, Arutiunov G, Kum LC, McKelvie R, Afzal R, White M, Nordmann AJ. Meta-analysis of combined therapy with angiotensin receptor antagonists versus ACE inhibitors alone in patients with heart failure. PloS one. 2010 Apr 1:5(4):e9946. doi: 10.1371/journal.pone.0009946. Epub 2010 Apr 1 [PubMed PMID: 20376345]
Level 1 (high-level) evidenceLucas C, Christie GA, Waring WS. Rapid onset of haemodynamic effects after angiotensin converting enzyme-inhibitor overdose: implications for initial patient triage. Emergency medicine journal : EMJ. 2006 Nov:23(11):854-7 [PubMed PMID: 17057137]
Level 2 (mid-level) evidenceSorodoc V, Sorodoc L, Lionte C, Gazzi E, Jaba IM, Mungiu OC. [Intentional poisoning with ACE inhibitors. Emergeny Hospital Iaşi]. Revista medico-chirurgicala a Societatii de Medici si Naturalisti din Iasi. 2010 Apr-Jun:114(2):359-62 [PubMed PMID: 20700967]
Level 2 (mid-level) evidenceVarughese A, Taylor AA, Nelson EB. Consequences of angiotensin-converting enzyme inhibitor overdose. American journal of hypertension. 1989 May:2(5 Pt 1):355-7 [PubMed PMID: 2541742]
Level 3 (low-level) evidenceJackson T, Corke C, Agar J. Enalapril overdose treated with angiotensin infusion. Lancet (London, England). 1993 Mar 13:341(8846):703 [PubMed PMID: 8095618]
Level 3 (low-level) evidenceLip GY, Ferner RE. Poisoning with anti-hypertensive drugs: angiotensin converting enzyme inhibitors. Journal of human hypertension. 1995 Sep:9(9):711-5 [PubMed PMID: 8551483]
Brown NJ, Vaughan DE. Angiotensin-converting enzyme inhibitors. Circulation. 1998 Apr 14:97(14):1411-20 [PubMed PMID: 9577953]
Pongpanich P, Pitakpaiboonkul P, Takkavatakarn K, Praditpornsilpa K, Eiam-Ong S, Susantitaphong P. The benefits of angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers combined with calcium channel blockers on metabolic, renal, and cardiovascular outcomes in hypertensive patients: a meta-analysis. International urology and nephrology. 2018 Dec:50(12):2261-2278. doi: 10.1007/s11255-018-1991-x. Epub 2018 Oct 15 [PubMed PMID: 30324578]
Level 1 (high-level) evidence