
Introduction
The spinal cord relies on 3 main arteries for vascular supply. The anterior spinal artery supplies the anterior two-thirds, and the 2 posterolateral spinal arteries supply the posterior third of the spinal cord.
The anterior spinal artery originates from the 2 vertebral arteries at the level of the foramen magnum. It is supplied by anterior segmental medullary vessels from the aorta, the biggest of which is the artery of Adamkiewicz also referred to as the arteria radicularis magna or the great anterior radiculomedullary artery.
The anatomic course of the artery of Adamkiewicz can be traced starting from the descending aorta. Here, approximately 8 to 10 segmental (either intercostal or lumbar) arteries branch off and split into anterior and posterior branches. The posterior branch then divides into 3: the radiculomedullary artery, the muscular branch, and the dorsal somatic branch. The radiculomedullary artery then splits into the main anterior and smaller posterior radiculomedullary arteries, and the largest anterior radiculomedullary artery is named the artery of Adamkiewicz. The artery of Adamkiewicz then passes through the intervertebral foramen and enters the spinal canal adjacent to the exiting spinal nerve (usually ventral or slightly rostrolateral to the dorsal root ganglion/ventral ramus. It then travels with the ventral root to the ventral (anterior) surface of the spinal cord, ascends, makes a classic “hairpin” arch, then directs toward and joins the anterior spinal artery. [1][2][3][4]
The artery of Adamkiewicz typically arises from the left side of the aorta between T8 and L2 (usually T9 to T12, although the artery of Adamkiewicz is found above T8 in about 15% of people), and has been documented as having a diameter anywhere from 0.6 to 1.8 mm. Variants include the artery of Adamkiewicz arising from the right side of the aorta or level outside of T8 through L2, differences in the angle of how the artery of Adamkiewicz joins the anterior spinal artery, and the presence of more than one artery of Adamkiewicz. Of note, collateral circulation is possible if the artery of Adamkiewicz has progressive occlusion; collaterals usually arise from the muscular branch or other intercostal or lumbar arteries.[3][5]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The artery of Adamkiewicz is significant in that it is the only major arterial supply supplying the anterior spinal artery along the lower thoracic, lumbar, and sacral segments of the spinal cord. Injury to this artery can cause neurologic damage manifesting as fecal and urinary incontinence, and impaired motor function, although the sensory function is usually preserved.
Blood Supply and Lymphatics
The artery of Adamkiewicz arises from the descending aorta.[1][2]
Surgical Considerations
The location of the artery of Adamkiewicz is very important for many surgical procedures since lack of flow to this vessel can cause ischemia to the spinal cord (discussed in the Clinical Significance section). Several surgical subspecialties must consider its location, including vascular surgery (thoracoabdominal aortic aneurysm repair), orthopedics (thoracolumbar spine surgery), neurosurgery (resection of intramedullary tumors), as well as urology and pediatric surgery (retroperitoneal dissections).[5]
Anatomical evaluation of the artery of Adamkiewicz is often performed preoperatively via computerized tomographic or magnetic resonance angiography to avoid neurological complications, and there are several documented cases of change in surgical approach if the artery of Adamkiewicz and planned approach are on the same side. Care must be taken to distinguish the artery of Adamkiewicz from the anterior radiculomedullary vein, which is very similar in shape and may follow a very close course to the artery of Adamkiewicz. To avoid confusing the 2, it is imperative to trace the artery from the aorta (termed the “continuity technique”). Of note, preoperative imaging may be difficult in patients with bony abnormalities (scoliosis, osteophytes, narrowing of intervertebral foramen), or patients with extensive arterial disease.[3][6][7]
Clinical Significance
Anterior cord syndrome (also called anterior spinal artery syndrome) most commonly occurs due to an interrupted supply of the anterior spinal artery or the Artery of Adamkiewicz (its major supplier), which has a less efficient supply compared to the 2 posterolateral spinal arteries. This commonly is caused by atherosclerotic disease, trauma (surgical instrumentation or direct injury by a disc or bone fragment), hypotension (for example, from blood loss in open surgery like bowel resection), vasculitic disorders. Anterior cord syndrome can also be caused by muscular disorders including spinal muscular atrophy and multiple sclerosis, as well as infectious causes including poliomyelitis and West Nile virus.
This syndrome affects the anterior two-thirds of the spinal cord, which includes the majority of the anterior and lateral white matter funiculi, the central gray matter, the bilateral lateral and anterior horns, and the bases of the posterior horns. This results in bilateral loss of motor function (flaccid paralysis at the level of the lesion and spastic paralysis below the lesion) from loss of the corticospinal tract and anterior horn, bilateral loss of pain, and temperature one level below the lesion from loss of the spinothalamic tract, and sexual dysfunction and urinary and fecal incontinence from loss of descending autonomic tracts. Sensations of touch, vibration, and proprioception remain intact since the posterior white matter columns are spared. Motor recovery occurs in less than half of patients with anterior cord syndrome, and treatment is generally supportive and focuses on addressing the underlying cause. Successful recovery involves enrolling patients in physical therapy, occupational therapy, and mental health support.[8][9][10]
Subarachnoid hemorrhage, which typically occurs intracranially, can also originate from the spine (less than 1% of all cases). Etiologies include arteriovenous malformations and fistulae, as well as isolated spinal artery aneurysms. Spinal subarachnoid hemorrhage should be on the differential diagnosis of patients who present with sudden-onset back pain, myelopathy, and radiculopathy.[11]
Other Issues
Transforaminal epidural steroid injections are commonly used to treat radicular pain, and there have been case reports of spinal cord infarction and acute paraplegia following this procedure. Typically, a posterior approach with a subpedicular technique is utilized. The needle tip is placed in the “safe triangle” in the superior aspect of the neural foramen, where it is immediately superior and lateral to the targeted nerve, which decreases the chance of traumatic injury to the nerve. While this method avoids injury to the nerve root, disruption of blood supply to the anterior spinal cord can occur with this procedure in the thoracic or upper lumbar spine if the needle tip is in the vicinity of the AKA, or other anterior medullary arteries. Case reports have suggested that acute paraplegia was due to direct needle injury, induced vasospasm, or embolization. Thus, it has been proposed that when epidural injections are performed at L3 and above, the needle should be placed in the inferior foramen instead.[4][12]
Media
(Click Image to Enlarge)
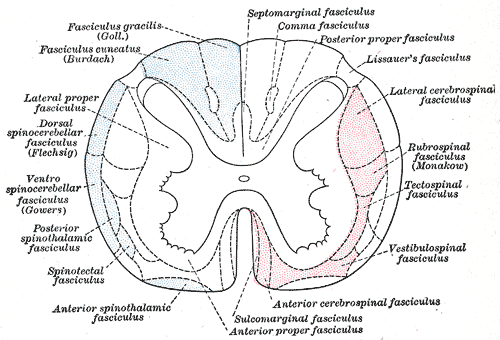
Nerve Fasciculi, Neurology. The illustration depicts the principal fasciculi of the spinal cord.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
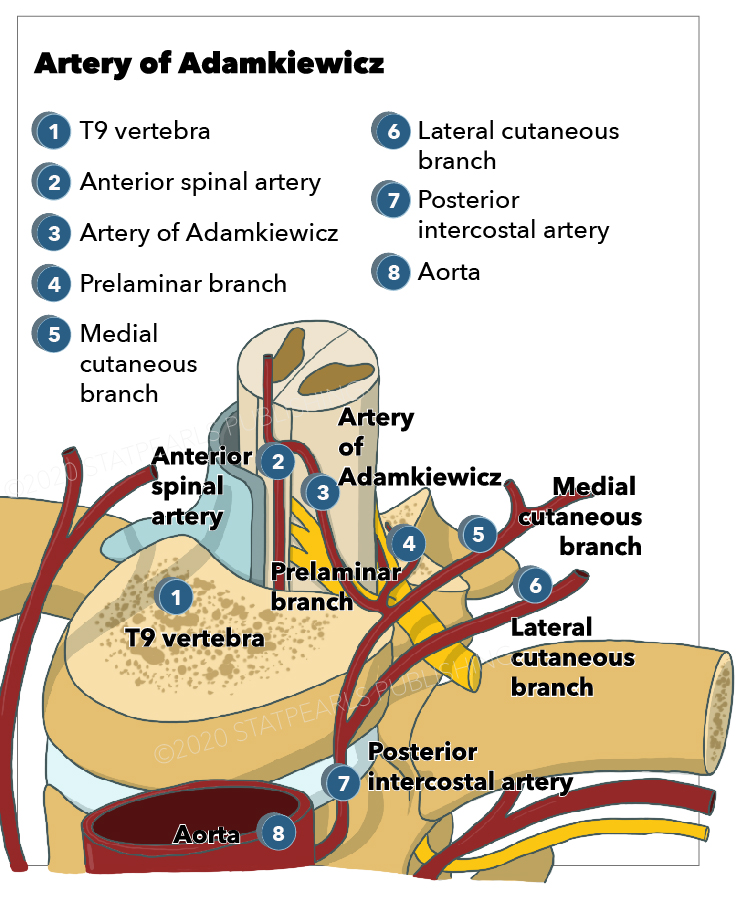
Anterior spinal artery, Artery of Adamkiewicz, Posterior intercostal artery, Lateral cutaneous branch StatPearls Illustration
References
N'da HA, Chenin L, Capel C, Havet E, Le Gars D, Peltier J. Microsurgical anatomy of the Adamkiewicz artery-anterior spinal artery junction. Surgical and radiologic anatomy : SRA. 2016 Jul:38(5):563-7. doi: 10.1007/s00276-015-1596-3. Epub 2015 Dec 1 [PubMed PMID: 26627692]
Guziński M, Bryl M, Ziemińska K, Wolny K, Sąsiadek M, Garcarek JS. Detection of the Adamkiewicz artery in computed tomography of the thorax and abdomen. Advances in clinical and experimental medicine : official organ Wroclaw Medical University. 2017 Jan-Feb:26(1):31-37. doi: 10.17219/acem/62788. Epub [PubMed PMID: 28397429]
Level 3 (low-level) evidenceYoshioka K, Niinuma H, Ehara S, Nakajima T, Nakamura M, Kawazoe K. MR angiography and CT angiography of the artery of Adamkiewicz: state of the art. Radiographics : a review publication of the Radiological Society of North America, Inc. 2006 Oct:26 Suppl 1():S63-73 [PubMed PMID: 17050520]
Murthy NS, Maus TP, Behrns CL. Intraforaminal location of the great anterior radiculomedullary artery (artery of Adamkiewicz): a retrospective review. Pain medicine (Malden, Mass.). 2010 Dec:11(12):1756-64. doi: 10.1111/j.1526-4637.2010.00948.x. Epub 2010 Sep 7 [PubMed PMID: 21134118]
Level 2 (mid-level) evidenceCharles YP, Barbe B, Beaujeux R, Boujan F, Steib JP. Relevance of the anatomical location of the Adamkiewicz artery in spine surgery. Surgical and radiologic anatomy : SRA. 2011 Jan:33(1):3-9. doi: 10.1007/s00276-010-0654-0. Epub 2010 Jun 30 [PubMed PMID: 20589376]
Amato ACM, Parga Filho JR, Stolf NAG. Predictors of Adamkiewicz artery and anterior spinal artery detection through computerized tomographic angiography. SAGE open medicine. 2017:5():2050312117711599. doi: 10.1177/2050312117711599. Epub 2017 Jun 2 [PubMed PMID: 28616230]
Tanaka H, Ogino H, Minatoya K, Matsui Y, Higami T, Okabayashi H, Saiki Y, Aomi S, Shiiya N, Sawa Y, Okita Y, Sueda T, Akashi H, Kuniyoshi Y, Katsumata T, Japanese Study of Spinal Cord Protection in Descending and Thoracoabdominal Aortic Repair investigators. The impact of preoperative identification of the Adamkiewicz artery on descending and thoracoabdominal aortic repair. The Journal of thoracic and cardiovascular surgery. 2016 Jan:151(1):122-8. doi: 10.1016/j.jtcvs.2015.07.079. Epub 2015 Jul 29 [PubMed PMID: 26344681]
Klakeel M, Thompson J, Srinivasan R, McDonald F. Anterior spinal cord syndrome of unknown etiology. Proceedings (Baylor University. Medical Center). 2015 Jan:28(1):85-7 [PubMed PMID: 25552812]
Level 3 (low-level) evidenceYadav N, Pendharkar H, Kulkarni GB. Spinal Cord Infarction: Clinical and Radiological Features. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2018 Oct:27(10):2810-2821. doi: 10.1016/j.jstrokecerebrovasdis.2018.06.008. Epub 2018 Aug 6 [PubMed PMID: 30093205]
Bican O, Minagar A, Pruitt AA. The spinal cord: a review of functional neuroanatomy. Neurologic clinics. 2013 Feb:31(1):1-18. doi: 10.1016/j.ncl.2012.09.009. Epub [PubMed PMID: 23186894]
Aljuboori Z, Sharma M, Simpson J, Altstadt T. Surgical Management of Ruptured Isolated Aneurysm of Artery of Adamkiewicz: Interesting Report and Overview of Literature. World neurosurgery. 2018 Mar:111():36-40. doi: 10.1016/j.wneu.2017.11.179. Epub 2017 Dec 9 [PubMed PMID: 29229349]
Level 3 (low-level) evidenceKroszczynski AC, Kohan K, Kurowski M, Olson TR, Downie SA. Intraforaminal location of thoracolumbar anterior medullary arteries. Pain medicine (Malden, Mass.). 2013 Jun:14(6):808-12. doi: 10.1111/pme.12056. Epub 2013 Feb 25 [PubMed PMID: 23438301]