Introduction
In 1841, a British anatomist, Alfred Poland, discovered a rare congenital chest wall muscle deficiency that he later named Poland syndrome. Poland syndrome most frequently involves unilateral underdevelopment or absence of chest wall muscle present at birth with some associated hand/upper extremity anomalies on the same side (see Image. Poland Syndrome With Absence of Pectoralis Major Muscle). Rarely, it is found to have bilateral chest muscle deficiency involvement. Some even suggest an association with vascular, skeletal, and inner organ anomalies. There is extensive variation in the presentation of Poland syndrome, which can sometimes make it difficult to diagnose.[1][2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Controversy exists over the etiology of Poland syndrome. It mostly occurs sporadically. However, 3 other theories about the development of Poland syndrome include genetic, teratogenic, or vascular compromise during fetal development as possible etiologies. There has been documentation that distant family members developed Poland syndrome, supporting the theory that it may be genetically linked. Another theory is that Poland syndrome results from environmental or medication-induced teratogenic effects on a developing fetus. Researchers found a higher incidence in pregnant smokers compared to pregnant non-smokers during embryogenesis.[3]
Other studies indicate medication-induced abortions for unwanted pregnancies with failed interruption of pregnancy as an induction factor of Poland syndrome. Some suggest vascular compromise during fetal development. These usually present with hypoplasia of subclavian or axillary vessels in Poland syndrome, which supports the theory of a poor developing limb bud. This could be caused by many factors, such as amniotic bands, tumors, edema, or aberrant muscle during the sixth and seventh weeks of embryogenesis.[2]
Epidemiology
Poland syndrome incidence ranges from 1 in 10,000 to 100,000 in live births.[3] In general, males are affected 3 times more than females. Right-sided anomalies are usually twice as predominant as left-sided ones. Most Poland syndrome is found sporadically, with some occasional familial genetic descendants. Mild forms are also more common than severe ones, suggesting that many cases are missed or under-represented. These aspects can underestimate the incidence rate overall.[1]
Pathophysiology
Poland syndrome has a wide diversity of clinical presentations. The congenital deformity can extend to anomalies of the pectoral muscle, breast, nipple complex, axillary fold, soft tissue, ribs, and upper limbs.[4] The classic pattern is unilateral hypoplasia or aplasia of the sternocostal head of the pectoralis major muscle and an ipsilateral hypoplastic hand with simple syndactyly and short webbed fingers. It is sometimes accompanied by underdeveloped breast tissue on the pectoral muscle deficiency side in females.[5] When the absence of the breast in females is the leading feature of Poland syndrome, it is also known as "Amazone syndrome," described by Mühlbauer in 1977. It was suggested that the extremity bud damage and the proximity of the lacteal mound during embryogenesis results in the lack of development of breast tissue described in Amazone syndrome.[2][6]
Poland syndrome has also been occasionally associated with vascular, skeletal, and inner organ anomalies, including subclavian and axillary vascular system variances, scoliosis, sternal and rib abnormalities, and even dextrocardia.[7]
Symbrachydactyly, sometimes referred to as "atypical cleft hand," is a congenital limb abnormality describing hand malformations involving brachydactyly (short fingers), syndactyly (union of 2 or more fingers), and global hypoplasia of the hand. These can include transverse deficiency (congenital amputation), central deficiency (absence of 1 or more digits in which the central rays of the hand are affected), brachymetacarpia (shortened metacarpal bone and finger), brachyphalangism (shortened phalanges), hypodactyly (fewer than the normal number of fingers). All these anomalies describe different forms and severity of hand conditions that can present in patients with Poland syndrome.[8]
History and Physical
Typical Poland syndrome presentations are aesthetical complaints regarding chest asymmetry. Most patients are found to be asymptomatic.[9] Children usually present first with finger or hand anomalies as the chest wall asymmetry appears more obvious as they age. In rare instances, severe Poland syndrome cases can present with obvious scoliosis, rib, and sternum deformity, which causes cardiopulmonary symptoms such as shortness of breath or difficulty taking deep breaths.
The examination begins by assessing the anterior chest wall for asymmetry. The presentation of chest wall tissue deficiency is highly variable. The pathognomonic finding is the absence of the sternocostal head of the pectoralis major muscle. Other structures that may be absent include ribs 2 to 5, latissimus dorsi, serratus anterior, and pectoralis minor. The presence or absence of the latissimus dorsi muscle is very important in surgical planning. The sternum and ribs may appear distorted or hypoplastic. The ipsilateral breast or nipple-areola complex may be absent or hypoplastic. The ipsilateral hand may have defects such as syndactyly, microdactyly, brachysyndactyly, or hypoplasia of the hand.
The patient may also have a variation of scoliosis and anterior chest wall defects such as pectus excavatum.[5] Visual inspection and palpation of the chest wall are important aspects of the physical evaluation that determine the muscle deficiencies and the bony deformities. Soft tissue on the affected side is usually thinner, with sometimes associated alopecia on the involved side.[10] The axilla and back should also be carefully examined and observed. Auscultation of the cardiopulmonary system is also a primordial part of the examination to rule out dextrocardia, a rare form of Poland syndrome that can be seen when the left side is involved.[11]
Evaluation
The only defining criterion in the diversity and variation of Poland syndrome is pectoral muscle deficiency.[12]
Treatment / Management
Surgical reconstruction varies based on the clinical presentation, age, gender, and severity of the deformity.[13] The most common procedure in women with Poland syndrome is mammary reconstruction with a silicone implant, usually performed after the age of 18. Many recommend a latissimus flap with a breast implant for severe forms of Poland syndrome in women. Syndactyly revision is usually performed in children in early childhood.[14] (B2)
In men, fat grafting is performed the most to compensate esthetically for muscle mass deficit. Autologous fat transfer is frequently used to correct chest wall asymmetry in mild to moderate deformity. In some cases, contralateral lipo-aspiration and rarely contralateral breast resection are considered in severe cases. More extensive chest wall reconstruction for PS includes autologous or alloplastic grafts. Muscle flap, either a pedicle or a free flap, can be used for chest wall reconstruction. Due to its proximity, the latissimus dorsi is usually considered a favorable option for muscle flaps. However, the contralateral side is another viable option when the muscle is aplastic ipsilaterally.[7][15][7](B3)
Bone graft or prosthesis can also be used to reconstruct the chest wall with or without a concomitant muscle flap.[16] Most breast and pectoral reconstructions now use single-step rather than a more extensive 2-step approach with tissue expanders. Recent studies even designed custom-made silicone implants with 3-dimensional computer aid design reconstruction.[17][18][19][20][21](B2)
Differential Diagnosis
The differential diagnoses for Poland syndrome include the following:
Staging
Most physicians use a classification system for Poland syndrome using grades I-III to qualify the different degrees of severity. The grading system is also referred to as Foucras classification.[19]
- Grade I: Mild chest deformity with pectoralis major hypoplasia and moderate breast hypoplasia; on examination, it illustrates slight chest wall asymmetry in men and breast asymmetry in women
- Grade II: Marked pectoralis major aplasia, hypoplasia, or other chest wall muscles, with possible rib deformity; it demonstrates a marked chest wall asymmetry in men and breast asymmetry in women
- Grade III: Full muscular and breast aplasia, including aplasia of other chest wall muscles with major bone and cartilage anomaly, including rib and sternal deformity; on physical exam, it presents as major chest wall asymmetry in men and women and breast asymmetry with aplasia in women
Prognosis
In a few research studies, some malignancies are associated with Poland syndrome, such as leukemia and carcinoma of the hypoplastic breast and other tumors. The relationship between congenital defects and tumors pushes to oncologic awareness.[16] The majority of children with Poland syndrome reach adulthood, and in general, it is considered to have a decent prognosis.
Complications
Complications of Poland syndrome patients are not commonly heard of as most patients are asymptomatic. Young children who present with few musculoskeletal dysfunctions are corrected at such an early age that they are usually not considered a true complication.[25]
Surgical treatment options for Poland syndrome come with their own expected surgical complications. Autologous fat transfer can sometimes postoperatively get complicated with fat necrosis that can be corrected after surgical drainage. Another long-term complication from fat grafting is liponecrotic cysts formation, which has benign characteristics on breast imaging.[17] Breast reconstruction complications, in general, include infection, bleeding, and poor healing of scars. Flap surgery complications involve the possible risk of loss of flap tissue, either complete or partial, and possible loss of sensation at the flap donor and reconstruction site.[26] Chest wall implants can sometimes postoperatively develop a seroma, infection, displacement, rupture, or capsule formation.[27]
Deterrence and Patient Education
The low incidence and unusual presentation of this syndrome, which presents at a young age in children, makes it sometimes difficult to diagnose and explain to distressed parents. Therefore, it is a crucial aspect of patient education and awareness, as this chest wall abnormality is usually confused and unrecognized for asymmetry by family members until perceived by their pediatricians during physical exams.
Enhancing Healthcare Team Outcomes
Poland Syndrome is an unfortunate congenital muscle deficiency that affects young children with disfiguring outcomes. It is a mental and physical disturbance that can affect patients over their entire lifespan if not treated accordingly. The goal of these patients is to use integrated care with different evidence-based approaches and planning to address their aesthetic concerns with plastic reconstruction and their psychological disorders with psychotherapy support. An interprofessional approach that provides a synergistic and integrated team dedicated to patient care can help achieve the best possible outcomes for Poland syndrome patients.[28]
The role of early cosmetic reconstruction and mental health support at a young age cannot be undermined. Suppose the patient is to be discharged home after surgical reconstruction. In that case, consultation should be made with a social worker, physical therapist, and community mental health therapist who can monitor the patient's progress, evaluate for proper recovery, and make referrals as needed. An integrated collaboration of different medical teams sharing decision-making, action plan, and communication is important for a successful long-term outcome.[6][28][6]
Media
(Click Image to Enlarge)
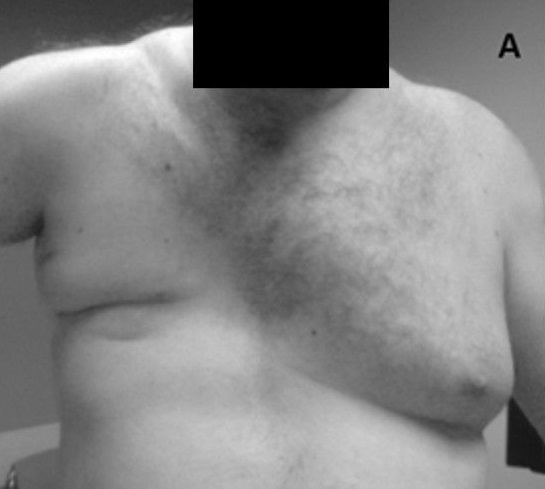
Poland Syndrome With Absence of Pectoralis Major Muscle
KJ Lizarraga and AAF De Salles, Public Domain, via Wikimedia Commons
References
Romanini MV, Calevo MG, Puliti A, Vaccari C, Valle M, Senes F, Torre M. Poland syndrome: A proposed classification system and perspectives on diagnosis and treatment. Seminars in pediatric surgery. 2018 Jun:27(3):189-199. doi: 10.1053/j.sempedsurg.2018.05.007. Epub 2018 Jun 8 [PubMed PMID: 30078491]
Level 3 (low-level) evidenceMühlbauer W, Wangerin K. [Embryology and etiology of the Poland and Amazone syndromes]. Handchirurgie. 1977:9(3):147-52 [PubMed PMID: 204553]
Slezak R, Sasiadek M. [Poland's syndrome]. Polski merkuriusz lekarski : organ Polskiego Towarzystwa Lekarskiego. 2000 Aug:9(50):568-71 [PubMed PMID: 11081328]
Level 3 (low-level) evidenceRomanini MV,Torre M,Santi P,Dova L,Valle M,Martinoli C,Baldelli I, Proposal of the TBN Classification of Thoracic Anomalies and Treatment Algorithm for Poland Syndrome. Plastic and reconstructive surgery. 2016 Jul; [PubMed PMID: 27348639]
Al-Qattan MM. Classification of hand anomalies in Poland's syndrome. British journal of plastic surgery. 2001 Mar:54(2):132-6 [PubMed PMID: 11207123]
Majdak-Paredes EJ, Shafighi M, Fatah F. Integrated algorithm for reconstruction of complex forms of Poland syndrome: 20-year outcomes. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2015 Oct:68(10):1386-94. doi: 10.1016/j.bjps.2015.05.015. Epub 2015 May 28 [PubMed PMID: 26159469]
Beer GM, Kompatscher P, Hergan K. Poland's syndrome and vascular malformations. British journal of plastic surgery. 1996 Oct:49(7):482-4 [PubMed PMID: 8983554]
Level 3 (low-level) evidenceGoodell PB,Bauer AS,Sierra FJ,James MA, Symbrachydactyly. Hand (New York, N.Y.). 2016 Sep; [PubMed PMID: 27698626]
Gui L, Shen S, Mei W. Anaesthesia for chest wall reconstruction in a patient with Poland syndrome: CARE-compliant case report and literature review. BMC anesthesiology. 2018 May 24:18(1):57. doi: 10.1186/s12871-018-0518-4. Epub 2018 May 24 [PubMed PMID: 29793431]
Level 3 (low-level) evidenceAl Faleh K, Al Saadi M, Khalid-Bantuas S. Poland's Syndrome with Absent Limb Anomalies. Journal of clinical neonatology. 2014 Jan:3(1):44-6. doi: 10.4103/2249-4847.128735. Epub [PubMed PMID: 24741541]
Level 3 (low-level) evidenceLacorte D, Marsella M, Guerrini P. A case of Poland Syndrome associated with dextroposition. Italian journal of pediatrics. 2010 Feb 20:36():21. doi: 10.1186/1824-7288-36-21. Epub 2010 Feb 20 [PubMed PMID: 20170539]
Level 3 (low-level) evidenceBaas M,Burger EB,Sneiders D,Galjaard RH,Hovius SER,van Nieuwenhoven CA, Controversies in Poland Syndrome: Alternative Diagnoses in Patients With Congenital Pectoral Muscle Deficiency. The Journal of hand surgery. 2018 Feb; [PubMed PMID: 29033291]
Fijałkowska M, Antoszewski B. Surgical treatment of patients with Poland's syndrome--own experience. Polski przeglad chirurgiczny. 2011 Dec:83(12):662-7. doi: 10.2478/v10035-011-0106-5. Epub [PubMed PMID: 22343203]
Level 2 (mid-level) evidenceBraun TL, Trost JG, Pederson WC. Syndactyly Release. Seminars in plastic surgery. 2016 Nov:30(4):162-170 [PubMed PMID: 27895538]
Freitas Rda S, o Tolazzi AR, Martins VD, Knop BA, Graf RM, Cruz GA. Poland's syndrome: different clinical presentations and surgical reconstructions in 18 cases. Aesthetic plastic surgery. 2007 Mar-Apr:31(2):140-6 [PubMed PMID: 17093886]
Level 3 (low-level) evidenceFokin AA, Robicsek F. Poland's syndrome revisited. The Annals of thoracic surgery. 2002 Dec:74(6):2218-25 [PubMed PMID: 12643435]
Pinsolle V, Chichery A, Grolleau JL, Chavoin JP. Autologous fat injection in Poland's syndrome. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2008 Jul:61(7):784-91. doi: 10.1016/j.bjps.2007.11.033. Epub 2008 Feb 21 [PubMed PMID: 18178141]
Baratte A, Bodin F, Del Pin D, Wilk A, Bruant C. [Poland's syndrome in women: Therapeutic indications according to the grade. Apropos of 11 cases and review of the literature]. Annales de chirurgie plastique et esthetique. 2011 Feb:56(1):33-42. doi: 10.1016/j.anplas.2010.10.016. Epub 2011 Feb 2 [PubMed PMID: 21292378]
Level 2 (mid-level) evidenceFekih M, Mansouri-Hattab N, Bergaoui D, Chaieb A, Fikry T, Khairi H. [Correction of breast Poland's anomalies. About eight cases and literature review]. Annales de chirurgie plastique et esthetique. 2010 Jun:55(3):211-8. doi: 10.1016/j.anplas.2009.06.003. Epub 2009 Oct 29 [PubMed PMID: 19879029]
Level 3 (low-level) evidenceChavoin JP, Taizou M, Moreno B, Leyx P, Grolleau JL, Chaput B. Correcting Poland Syndrome with a Custom-Made Silicone Implant: Contribution of Three-Dimensional Computer-Aided Design Reconstruction. Plastic and reconstructive surgery. 2018 Aug:142(2):109e-119e. doi: 10.1097/PRS.0000000000004605. Epub [PubMed PMID: 30045173]
Hodgkinson DJ. Chest wall implants: their use for pectus excavatum, pectoralis muscle tears, Poland's syndrome, and muscular insufficiency. Aesthetic plastic surgery. 1997 Jan-Feb:21(1):7-15 [PubMed PMID: 9204161]
Level 3 (low-level) evidenceJansari M, Karkhanis V, Joshi JM. Unilateral hyperlucent lung: Always think ACROSS. Lung India : official organ of Indian Chest Society. 2013 Oct:30(4):368-9. doi: 10.4103/0970-2113.120629. Epub [PubMed PMID: 24339504]
Losken A, Fishman I, Denson DD, Moyer HR, Carlson GW. An objective evaluation of breast symmetry and shape differences using 3-dimensional images. Annals of plastic surgery. 2005 Dec:55(6):571-5 [PubMed PMID: 16327452]
Caouette-Laberge L, Borsuk D. Congenital anomalies of the breast. Seminars in plastic surgery. 2013 Feb:27(1):36-41. doi: 10.1055/s-0033-1343995. Epub [PubMed PMID: 24872738]
Sunitha VC, Narayanan S, Nair PP, Prakash ML. Left-sided Poland's syndrome in a girl with rare associations like spina bifida and diaphragmatic hernia. BMJ case reports. 2013 Sep 20:2013():. doi: 10.1136/bcr-2013-200930. Epub 2013 Sep 20 [PubMed PMID: 24057335]
Level 3 (low-level) evidenceUrschel HC Jr. Poland syndrome. Seminars in thoracic and cardiovascular surgery. 2009 Spring:21(1):89-94. doi: 10.1053/j.semtcvs.2009.03.004. Epub [PubMed PMID: 19632568]
Scheflan M, Kalisman M. Complications of breast reconstruction. Clinics in plastic surgery. 1984 Apr:11(2):343-50 [PubMed PMID: 6233063]
Baldelli I, Santi P, Dova L, Cardoni G, Ciliberti R, Franchelli S, Merlo DF, Romanini MV. Body Image Disorders and Surgical Timing in Patients Affected by Poland Syndrome: Data Analysis of 58 Case Studies. Plastic and reconstructive surgery. 2016 Apr:137(4):1273-1282. doi: 10.1097/PRS.0000000000002018. Epub [PubMed PMID: 27018681]
Level 3 (low-level) evidence