Introduction
The term ‘bronchopulmonary dysplasia’ (BPD) was first used by Northway et al. in 1967 to describe a chronic form of injury to the lungs caused by barotrauma and oxygen injury in preterm infants requiring mechanical ventilation.[1] Despite significant advances in preterm infant care in the past few decades, including the development of surfactant as well as newer and gentler modes of ventilation, the prevalence of BPD continues to remain high. These new strategies have allowed the survival of very low birth weight infants and resulted in a change in the characteristics of BPD. Jobe coined the term “new BPD” in 1999 to describe the chronic lung disease in preterm infants at that time. This “new BPD” demonstrated much less airway damage and alveolar septal fibrosis when compared to “old BPD” which was characterized by dysmorphic microvasculature and alveolar simplification.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Bronchopulmonary dysplasia is a multifactorial pathology that is influenced by a variety of prenatal and postnatal factors affecting the mother and infant. The various prenatal risk factors that influence the development of BPD include[3]:
- Lack of antenatal steroids
- Maternal smoking
- Pregnancy-induced hypertension/preeclampsia
- Hypoxia
- Maternal infection, including chorioamnionitis
- Genetic susceptibility
- Congenital anomalies causing pulmonary hypoplasia
Similarly, various postnatal factors predispose premature infants to develop BPD including:
- Lung immaturity
- Poor nutrition
- Need for mechanical ventilation
- Oxygen injury
- Infection/sepsis
Epidemiology
The incidence of BPD varies significantly between different centers because of variation in perinatal practices, differences in management styles and lack of consistent definition of BPD. The highest observed rate of BPD is in infants born at a lower gestational age (GA) and lower birth weight.[4] The data from the neonatal research network reports the incidence of BPD in very low birth weight infants (birth weight less than 1500 grams) to be 40 to 68% depending on the definition of BPD used. This incidence was found to be inversely proportional to the GA of the infant[5] The other demographic risk factors associated with BPD include male sex, low birth weight, white race, impaired growth for GA and family history of asthma.[4]
Pathophysiology
Injury from mechanical ventilation and reactive oxygen species to premature lungs in the presence of antenatal factors predisposing the lungs to BPD form the basis of pathogenesis of BPD in preterm neonates. This myriad of events leads to an exaggerated inflammatory response with an increase in proinflammatory cytokines like interleukin(IL)-6, IL 8, tumor necrosis factor alpha etc along with growth factors (transforming growth factor ) and angiogenic factors (vascular endothelial growth factor, angiopoietin 2) which ultimately results in aberrant tissue repair and arrest in lung development. Dysregulated vascular and arrested alveolar development form the basis of the pathology seen in “new BPD.”[6]
Histopathology
Bronchopulmonary dysplasia occurs when lung development arrests in the late canalicular to saccular stages of lung development. The pathology in BPD characteristically demonstrates decreased septation and alveolar hypoplasia resulting in simplified large alveoli and reduced area available for gaseous exchange. There is also dysregulated vasculature with smooth muscle hyperplasia in pulmonary vessels and abnormal alveolar capillaries. Additionally, there is also the presence of increased interstitial fibroproliferation and alveolar septation.[7]
History and Physical
The clinical phenotype of infants with BPD is very variable. Depending on the severity of their disease they may or may not need respiratory support. Some may be tachypneic and depending on the degree of pulmonary edema may have signs of respiratory distress like retractions, rales and increased work of breathing.
Evaluation
Evaluation of BPD involves assessment of blood gas, chest x-ray and evaluating the nutritional status of the patient. An arterial blood gas may reveal hypoxia, hypercarbia or acidosis. These patients remain on continuous pulse oximetry to help target adequate oxygen saturation. Many centers also utilize transcutaneous carbon dioxide monitoring to evaluate the ventilation of the infant.
Chest radiographs may show decreased lung volumes, hyperinflation, areas of atelectasis, pulmonary edema, and pulmonary interstitial emphysema. High-resolution CT may demonstrate abnormalities not readily seen with routine chest radiography. Infants with moderate or severe BPD must be screened for pulmonary hypertension(PH) at 36 PMA using an echocardiogram. Some centers chose to screen all patients with BPD since the morbidity and mortality associated with the diagnosis of PH in BPD are quite high.
The diagnosis of BPD is made clinically based on the GA, postmenstrual age (PMA), oxygen exposure and oxygen requirement at 36 weeks PMA. In 2001, the National Institute of Child Health and Human Development (NICHD) workshop proposed the current definition where infants born at less than or equal to 32 weeks GA with 28 days of oxygen exposure get diagnosed with mild, moderate or severe BPD at 36 weeks PMA based on their respiratory support at that time.[8] Table 1 illustrates the definition used for diagnosing and classifying the severity of the disease.
This definition still has many deficiencies and does not adequately predict respiratory outcomes; hence in 2016, the NICHD workshop on BPD proposed a revision of this definition. The suggested refinement suggests utilizing radiographic confirmation and accounts for the newer modes of non-invasive ventilation.[9] Although this new definition classifies BPD further, it does not address the primary limitation of utilizing the treatment modality as the primary factor defining the disease and its severity.[10]
Treatment / Management
The global aim in the management of infants with BPD is to support them while lung growth occurs, limit further injury to the lungs, optimize lung function and detect complications associated with BPD. The various measures employed in the care of these infants are-
- Nutrition: Infants with BPD need an increased amount of energy to promote lung growth and repair. Their nutritional need maybe up to 140 to 150 Kcal/Kg/day and protein intake from 3.5 to 4 g/kg/day.[11] Breast milk is preferable to formula. Commercial milk fortifiers can be used to fortify the mother’s milk or donor breast milk to higher calories.[12] Intramuscular supplementation of vitamin A started within a few days of birth and administered three times a week for 4 weeks has been shown to decrease the risk of BPD by 7%.[13]
- Fluid restriction: Based on the severity of their lung disease, infants are restricted to a total fluid volume of 120 to 150 ml/kg/day. Restriction of fluid intake allows for improved pulmonary function by preventing pulmonary edema and improving gas exchange. Although frequently followed, there is insufficient data to support this practice.[14]
- Minimize ventilator-associated lung injury: Non-invasive ventilation is the preferred mode of ventilation wherever feasible. If mechanical ventilation is necessary, care should be taken to limit barotrauma and volutrauma. Early extubation has been shown to lower the rates of BPD.[15]
- Minimize oxygen associated injury: Exposure to hyperoxia is one of the most critical factors in the pathogenesis of BPD. There is significant controversy regarding SpO target ranges. One approach attempts to target SpO of 88-94% with a lower alarm limit of 88% and a higher alarm limit of 96%.[16]
- Pharmacological interventions: (A1)
- Corticosteroids: Systemic corticosteroids have been used in BPD to improve lung function, reduce inflammation and reduce the need for mechanical ventilation. However, concerns about long term neurodevelopmental outcomes have led to recommendations to restrict their use to infants with severe BPD who remain ventilator dependent with high oxygen needs.[17][18] Despite many clinical trials, it is unclear as to which corticosteroid provides the most benefit and at the optimal dose. Notwithstanding the variable evidence, low dose dexamethasone and hydrocortisone continue to be used in practice in the treatment of BPD.[19] The current data does not demonstrate support for the routine use of inhaled corticosteroids to prevent BPD.[20]
- Diuretics: Thiazides and loop diuretics are the most commonly used diuretics in the setting to improve short term pulmonary mechanics of BPD. These agents are most commonly used in infants who are ventilator dependent with increasing requirement of positive end-expiratory pressure despite fluid restriction. A systemic review of available literature does not show any improvement in long term clinical outcome in infants with established or developing BPD.[21]
- Bronchodilators:- administration of beta-2 agonists can decrease airway resistance and improve compliance. However, their routine use is not recommended in BPD as it has not been shown to improve long term outcomes. Their use should be restricted to manage acute episodes of bronchoconstriction in older infants who remain ventilator dependent.[22] (A1)
Differential Diagnosis
- Pulmonary atelectasis
- Pneumonia
- Pulmonary hypertension
- Tracheomalacia
- Pulmonary interstitial emphysema
Prognosis
BPD is a chronic illness that persists beyond discharge from the hospital and into adulthood. Infants with BPD have a 50% chance of readmission to the hospital during their first year of life. They have an increased risk of developing reactive airway disease, asthma, emphysema, and RSV bronchiolitis. BPD also affects their growth and neurodevelopmental outcome. VLBW infants with BPD are more likely to have delays in fine and gross motor skills, and language.[23]
Infants with BPD are at high risk for cardiopulmonary sequelae like pulmonary hypertension (PH), cor pulmonale, and systemic hypertension. A recent meta-analysis reported an accumulative estimated prevalence of PH in BPD to be 20% and can be as high as 40% in severe BPD. A newer, prospective study showed that BPD-associated pulmonary hypertension (BPD-PH) affects at least 8 to 25% of extremely low birth weight (birth weight less than 1000g) infants. Retrospective studies demonstrate a 2-year morbidity rate of 26 to 47% in patients with BPD-PH.[24]
Complications
BPD is one of the most prevalent morbidities associated with prematurity and carries associations with the following complications-
- Systemic hypertension
- Poor neurodevelopmental outcome
- Pulmonary Hypertension
- Left ventricular hypertrophy and left ventricular dysfunction
Deterrence and Patient Education
Bronchopulmonary dysplasia (BPD) is a severe disease that affects babies who are born early and need to be in the NICU. It causes breathing problems in babies and occurs because their lungs are not well developed and ready to do the work of breathing. These babies often need to have a breathing tube and are connected to a breathing machine to help them breathe. They may need several medications during their hospital stay to help with this lung disease. Some babies may also require home oxygen and may need to return to the hospital if they develop respiratory infections. Babies with BPD also need more energy and may require extra nutrition.
Babies who have BPD may develop other problems such as:
- Increased blood pressure
- Eye and ear problems
- Development problems
- Heart problems.
While in the NICU the doctors must be vigilant for these problems. Even after discharge, the baby may require followup for with doctors and developmental specialists.
Enhancing Healthcare Team Outcomes
Optimizing care of infants with BPD requires an interprofessional team approach that includes a neonatologist, nurses, pediatric pulmonologist, respiratory therapist, nutritionist, physical and occupational therapists, social worker and child life specialist. Training of the parent prior to discharge is critical. At the time of transition from hospital to home, adequate discharge planning is essential with setting up follow appointments and making sure parents have all the supplies necessary for taking care of their child.
Media
(Click Image to Enlarge)
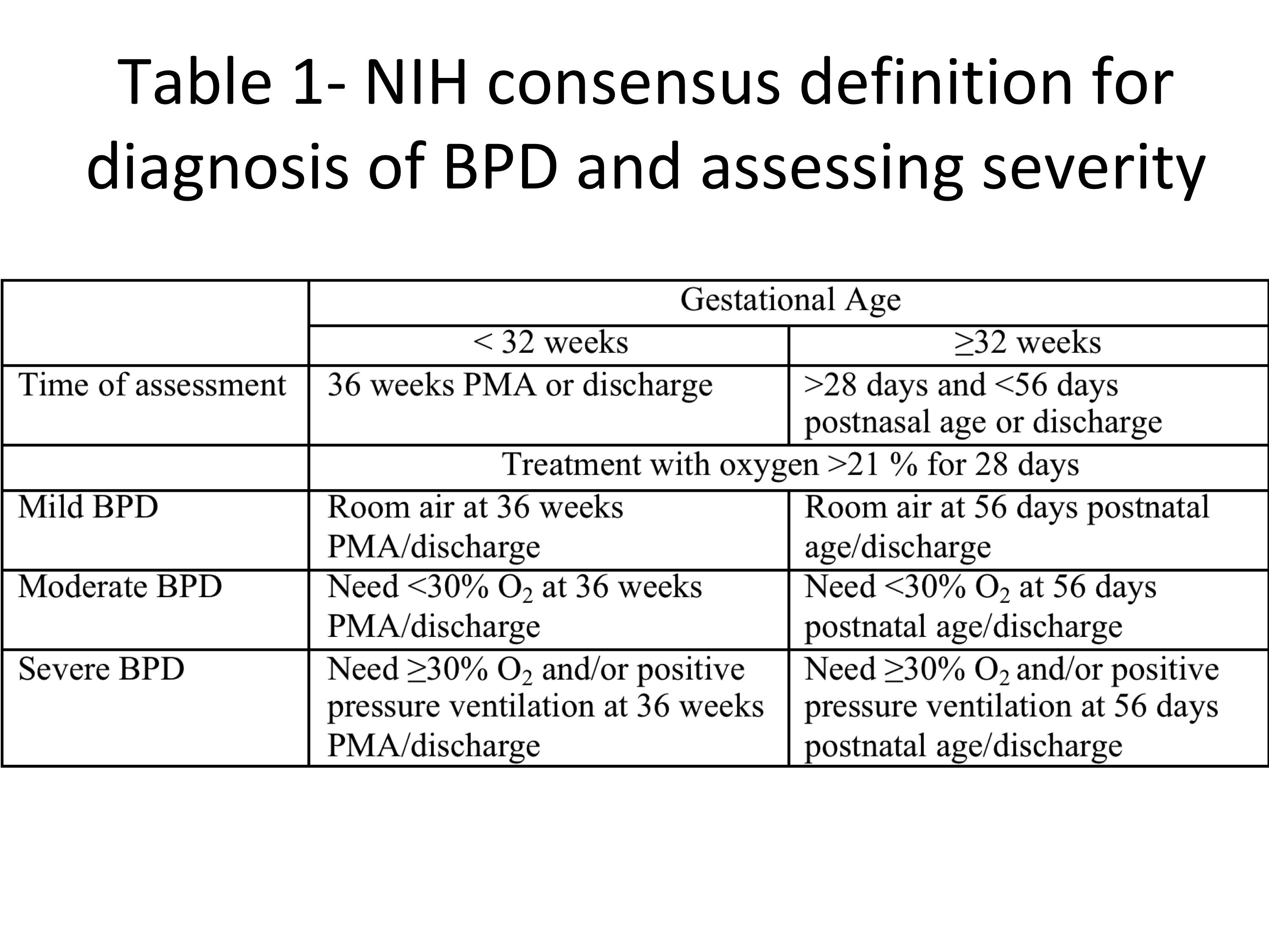
Definition of BPD "Contributed by Mitali Sahni, MD"
References
Northway WH Jr, Rosan RC, Porter DY. Pulmonary disease following respirator therapy of hyaline-membrane disease. Bronchopulmonary dysplasia. The New England journal of medicine. 1967 Feb 16:276(7):357-68 [PubMed PMID: 5334613]
Level 2 (mid-level) evidenceJobe AJ. The new BPD: an arrest of lung development. Pediatric research. 1999 Dec:46(6):641-3 [PubMed PMID: 10590017]
Level 3 (low-level) evidenceBalany J, Bhandari V. Understanding the Impact of Infection, Inflammation, and Their Persistence in the Pathogenesis of Bronchopulmonary Dysplasia. Frontiers in medicine. 2015:2():90. doi: 10.3389/fmed.2015.00090. Epub 2015 Dec 21 [PubMed PMID: 26734611]
Level 3 (low-level) evidenceJensen EA, Schmidt B. Epidemiology of bronchopulmonary dysplasia. Birth defects research. Part A, Clinical and molecular teratology. 2014 Mar:100(3):145-57. doi: 10.1002/bdra.23235. Epub 2014 Mar 17 [PubMed PMID: 24639412]
Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, Hale EC, Newman NS, Schibler K, Carlo WA, Kennedy KA, Poindexter BB, Finer NN, Ehrenkranz RA, Duara S, Sánchez PJ, O'Shea TM, Goldberg RN, Van Meurs KP, Faix RG, Phelps DL, Frantz ID 3rd, Watterberg KL, Saha S, Das A, Higgins RD, Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010 Sep:126(3):443-56. doi: 10.1542/peds.2009-2959. Epub 2010 Aug 23 [PubMed PMID: 20732945]
Morty RE. Recent advances in the pathogenesis of BPD. Seminars in perinatology. 2018 Nov:42(7):404-412. doi: 10.1053/j.semperi.2018.09.001. Epub 2018 Oct 2 [PubMed PMID: 30384986]
Level 3 (low-level) evidenceCoalson JJ. Pathology of new bronchopulmonary dysplasia. Seminars in neonatology : SN. 2003 Feb:8(1):73-81 [PubMed PMID: 12667832]
Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, Wrage LA, Poole K, National Institutes of Child Health and Human Development Neonatal Research Network. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics. 2005 Dec:116(6):1353-60 [PubMed PMID: 16322158]
Level 3 (low-level) evidenceHiggins RD, Jobe AH, Koso-Thomas M, Bancalari E, Viscardi RM, Hartert TV, Ryan RM, Kallapur SG, Steinhorn RH, Konduri GG, Davis SD, Thebaud B, Clyman RI, Collaco JM, Martin CR, Woods JC, Finer NN, Raju TNK. Bronchopulmonary Dysplasia: Executive Summary of a Workshop. The Journal of pediatrics. 2018 Jun:197():300-308. doi: 10.1016/j.jpeds.2018.01.043. Epub 2018 Mar 16 [PubMed PMID: 29551318]
Ibrahim J, Bhandari V. The definition of bronchopulmonary dysplasia: an evolving dilemma. Pediatric research. 2018 Nov:84(5):586-588. doi: 10.1038/s41390-018-0167-9. Epub 2018 Sep 4 [PubMed PMID: 30188504]
Arigliani M, Spinelli AM, Liguoro I, Cogo P. Nutrition and Lung Growth. Nutrients. 2018 Jul 18:10(7):. doi: 10.3390/nu10070919. Epub 2018 Jul 18 [PubMed PMID: 30021997]
Kim LY, McGrath-Morrow SA, Collaco JM. Impact of breast milk on respiratory outcomes in infants with bronchopulmonary dysplasia. Pediatric pulmonology. 2019 Mar:54(3):313-318. doi: 10.1002/ppul.24228. Epub 2019 Jan 4 [PubMed PMID: 30609293]
Ambalavanan N, Wu TJ, Tyson JE, Kennedy KA, Roane C, Carlo WA. A comparison of three vitamin A dosing regimens in extremely-low-birth-weight infants. The Journal of pediatrics. 2003 Jun:142(6):656-61 [PubMed PMID: 12838194]
Level 1 (high-level) evidencePasha AB, Chen XQ, Zhou GP. Bronchopulmonary dysplasia: Pathogenesis and treatment. Experimental and therapeutic medicine. 2018 Dec:16(6):4315-4321. doi: 10.3892/etm.2018.6780. Epub 2018 Sep 19 [PubMed PMID: 30542380]
Bhandari V. The potential of non-invasive ventilation to decrease BPD. Seminars in perinatology. 2013 Apr:37(2):108-14. doi: 10.1053/j.semperi.2013.01.007. Epub [PubMed PMID: 23582965]
Dumpa V, Bhandari V. Surfactant, steroids and non-invasive ventilation in the prevention of BPD. Seminars in perinatology. 2018 Nov:42(7):444-452. doi: 10.1053/j.semperi.2018.09.006. Epub 2018 Oct 2 [PubMed PMID: 30343941]
Committee on Fetus and Newborn. Postnatal corticosteroids to treat or prevent chronic lung disease in preterm infants. Pediatrics. 2002 Feb:109(2):330-8 [PubMed PMID: 11826218]
Baud O, Maury L, Lebail F, Ramful D, El Moussawi F, Nicaise C, Zupan-Simunek V, Coursol A, Beuchée A, Bolot P, Andrini P, Mohamed D, Alberti C, PREMILOC trial study group. Effect of early low-dose hydrocortisone on survival without bronchopulmonary dysplasia in extremely preterm infants (PREMILOC): a double-blind, placebo-controlled, multicentre, randomised trial. Lancet (London, England). 2016 Apr 30:387(10030):1827-36. doi: 10.1016/S0140-6736(16)00202-6. Epub 2016 Feb 23 [PubMed PMID: 26916176]
Level 1 (high-level) evidenceDoyle LW, Davis PG, Morley CJ, McPhee A, Carlin JB, DART Study Investigators. Low-dose dexamethasone facilitates extubation among chronically ventilator-dependent infants: a multicenter, international, randomized, controlled trial. Pediatrics. 2006 Jan:117(1):75-83 [PubMed PMID: 16396863]
Level 1 (high-level) evidenceShah VS, Ohlsson A, Halliday HL, Dunn M. Early administration of inhaled corticosteroids for preventing chronic lung disease in very low birth weight preterm neonates. The Cochrane database of systematic reviews. 2017 Jan 4:1(1):CD001969. doi: 10.1002/14651858.CD001969.pub4. Epub 2017 Jan 4 [PubMed PMID: 28052185]
Level 1 (high-level) evidenceStewart A, Brion LP, Ambrosio-Perez I. Diuretics acting on the distal renal tubule for preterm infants with (or developing) chronic lung disease. The Cochrane database of systematic reviews. 2011 Sep 7:2011(9):CD001817. doi: 10.1002/14651858.CD001817.pub2. Epub 2011 Sep 7 [PubMed PMID: 21901679]
Level 1 (high-level) evidenceSosulski R, Abbasi S, Bhutani VK, Fox WW. Physiologic effects of terbutaline on pulmonary function of infants with bronchopulmonary dysplasia. Pediatric pulmonology. 1986 Sep-Oct:2(5):269-73 [PubMed PMID: 3774383]
Anderson PJ, Doyle LW. Neurodevelopmental outcome of bronchopulmonary dysplasia. Seminars in perinatology. 2006 Aug:30(4):227-32 [PubMed PMID: 16860163]
Bhandari A, Bhandari V. Pitfalls, problems, and progress in bronchopulmonary dysplasia. Pediatrics. 2009 Jun:123(6):1562-73. doi: 10.1542/peds.2008-1962. Epub [PubMed PMID: 19482769]
Level 3 (low-level) evidence