Introduction
Right bundle branch block (RBBB) is an electrocardiogram finding that occurs when the physiologic electrical conduction system of the heart, specifically in the His-Purkinje system, is altered or interrupted resulting in a widened QRS and electrocardiographic vector changes. The bundle of His divides in the interventricular septum into the right and left bundle branches. Initially, the right bundle branch off of the bundle of His travels down the interventricular septum near the endocardium. It then dives deeper into the muscular layer before re-emerging near the endocardium again. The right bundle branch receives most of its blood supply from the anterior descending coronary artery. It also receives collateral circulation from the right or left circumflex coronary arteries, depending on the dominance of the heart.[1]
Right bundle branch block is associated with structural changes from stretch or ischemia to the myocardium.[2] It can also occur iatrogenically from certain common cardiac procedures, such as right heart catheterization.[3] Although there is no significant association with cardiovascular risk factors, the presence of a right bundle branch block is a predictor of mortality in myocardial infarction, heart failure, and certain heart blocks. In asymptomatic patients, isolated right bundle branch block typically does not need further evaluation.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Due to the anatomy of the right bundle branch, damage typically occurs at 3 different locations. The proximal right bundle nearest the endocardium is the most common location to be affected. The distal right bundle is typically only injured when the moderator band is transected during surgery. The terminal right bundle is injured during ventriculotomy or transatrial resection.[5]
A right bundle branch block is typically caused by disease processes that change the myocardium of the right bundle branch, for example, structural changes, trauma, and infiltrative processes. Rarely, hyperkalemia can alter the conduction physiology by slowing electrical impulse conduction through cardiac tissue, causing a right bundle branch block.[6] Infections such as myocarditis or myocardial infarction can cause direct cellular damage to the right bundle branch.[2] Increased right intraventricular pressure, either acutely by pulmonary embolism or chronically as in cor pulmonale, can stretch the right bundle branch causing a bundle branch block.[7] RBBB can also be induced iatrogenically from right heart catheterizations and by ethanol ablation for a septal reduction in hypertrophic cardiomyopathy.[3][8] Idiopathic fibrosis and calcification of the conduction system, called Lenegre’s disease or Lev’s disease, is a less common cause of right bundle branch block but most commonly occurs in the elderly.[9][10] In patients with underlying heart disease causing degeneration of the conduction pathway, a tachycardia dependent bundle branch block can occur. This happens when the heart rate reaches an elevated rate and becomes uncoupled from the refractory period, thus blocking the next electrical stimuli down the right bundle branch.[11]
Epidemiology
Right bundle branch block is generally a slowly progressive degenerative disease of the myocardium. The incidence of right bundle branch block typically increases with age, with up to 11.3% of people by age 80. There is no significant association with cardiac disease, ischemic heart disease or cardiac risk factors.[12]
Pathophysiology
When the right bundle branch is interrupted, electrical stimuli from the atrioventricular (AV) node conducts to the bundle of His and down the left bundle branch. The left ventricle depolarizes first while the right ventricle polarized later, causing the characteristic ECG findings.[13]
History and Physical
Right bundle branch block is usually asymptomatic and is typically found incidentally on ECG. The ECG finding itself does not cause any signs or symptoms. On physical examination, the patient may have a split second heart sound.[14]
Evaluation
The characteristic ECG findings for right bundle branch block are as follows:
- QRS duration is greater than or equal to 120 milliseconds
- In lead V1 and V2, there is an RSR` in leads V1 and V2
- In Leads 1 and V6, the S wave is of greater duration than the R wave, or the S wave is greater than 40 milliseconds
- In Leads V5 and V6, there is a normal R wave peak time
- In Lead V1, the R wave peak time is greater than 50 milliseconds
T waves tend to be discordant to the terminal QRS vector. This results in inverted T waves in the right precordial leads and upright T waves in the left precordial leads.[15]
Treatment / Management
Generally, the isolated presence of a right bundle branch block is asymptomatic and does not require further evaluation or treatment. In the setting of heart failure with a low ventricular ejection fraction in combination with a right bundle branch block, cardiac resynchronization therapy is indicated.[16](B2)
Differential Diagnosis
The differential diagnosis for right bundle branch block includes incomplete left bundle branch block, ventricular tachycardia, and Brugada syndrome. Incomplete right bundle branch block has similar electrocardiographic features with a QRS duration of 100 to 119 milliseconds. Ventricular tachycardia or an accelerated idioventricular rhythm can have a similar appearance to a right bundle branch block if the dominant pacemaker originates from the ventricles. Brugada syndrome has an ECG similar to that of a right bundle branch block.[17]
In patients who have a pacemaker in place and have a QRS complex with right bundle branch block morphology, evaluation needs to be performed for right ventricular lead perforation or accidental left ventricular lead placement.[18]
Prognosis
In patients without significant heart disease, right bundle branch block does not have any additional risk. In patients with cardiovascular disease, right bundle branch block is an independent risk factor for all-cause mortality. The presence of a right bundle branch block before acute myocardial infarction, during an acute MI and post-MI, are all associated with higher mortality rates. In heart failure, the presence of a right bundle branch block has also been associated with increased mortality.[19]
Pearls and Other Issues
In myocardial infarction, the presence of a left bundle branch block alters the conduction system in such a way that makes the ST segments of the electrocardiogram difficult to interpret. The presence of a right bundle branch block does not affect the ST segments in the same way that a left bundle branch block does, and thus does not interfere with the diagnosis of myocardial infarction.[20]
In patients with a left bundle branch block, special care needs to be taken when undergoing a right heart catheterization as there is an increased risk of complete heart block due to the increased risk of iatrogenically induced RBBB.[3]
Enhancing Healthcare Team Outcomes
ECGS are regularly done in clinical practice and sometimes the primary care provider, nurse practitioner and the internist may come across a patient with a RBBB. In isolation and in an asymptomatic patient, RBBB is benign. However, the patient should be referred to a cardiologist to ensure that he or she has no heart disease. In patients wih CHF and RBBB, cardiac resynchronization therapy is indicated.[16] The outlook after treatment is fair but without treatment, most patients have a poro quality of life and a shortened life span.
Media
(Click Image to Enlarge)
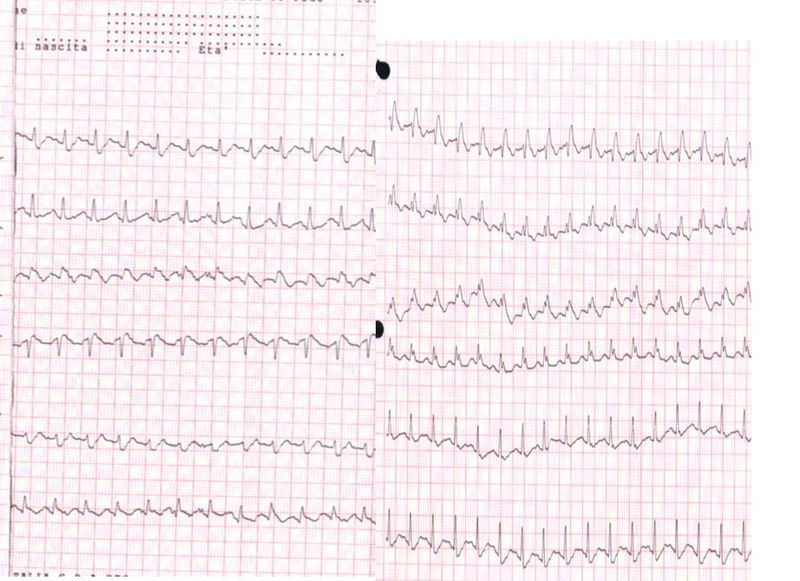
Electrocardiogram, Pulmonary Embolism. The ECG of a patient with pulmonary embolism showed sinus tachycardia of approximately 150 bpm and a right bundle branch block.
Walter Serra, Giuseppe De Iaco, Claudio Reverberi, Tiziano Gherli, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
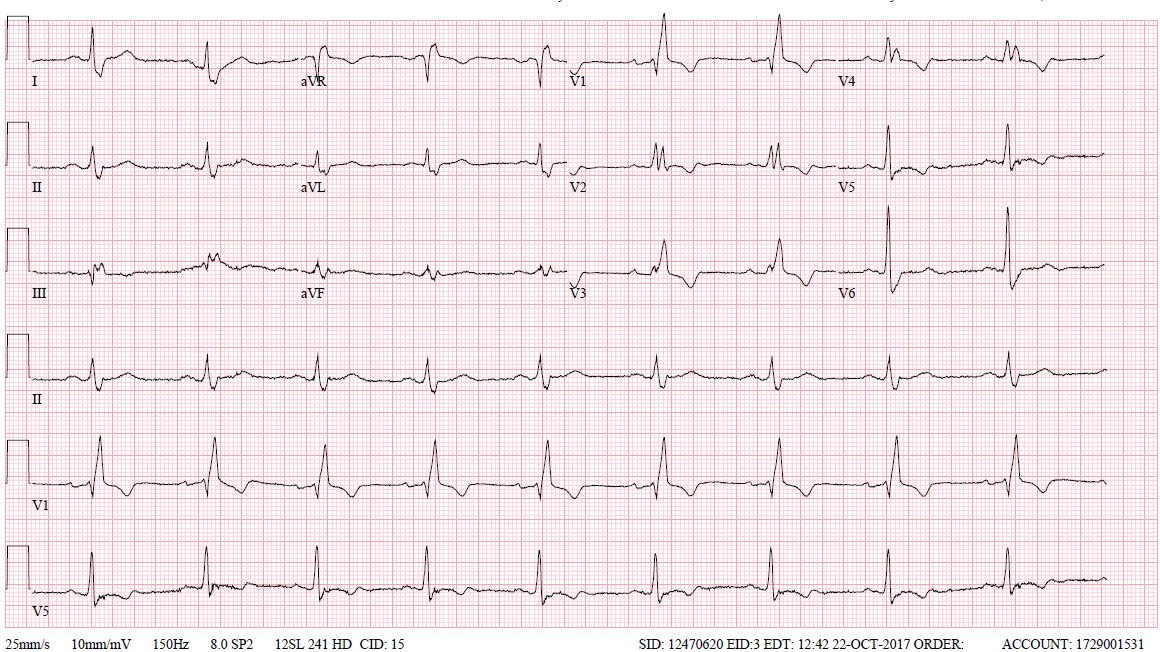
First degree Av block with Right Bundle Branch Block Contributed by Dhaval Desai, MD
References
Tusscher KH, Panfilov AV. Modelling of the ventricular conduction system. Progress in biophysics and molecular biology. 2008 Jan-Apr:96(1-3):152-70 [PubMed PMID: 17910889]
Level 3 (low-level) evidenceSarda L, Colin P, Boccara F, Daou D, Lebtahi R, Faraggi M, Nguyen C, Cohen A, Slama MS, Steg PG, Le Guludec D. Myocarditis in patients with clinical presentation of myocardial infarction and normal coronary angiograms. Journal of the American College of Cardiology. 2001 Mar 1:37(3):786-92 [PubMed PMID: 11693753]
Patil AR. Risk of right bundle-branch block and complete heart block during pulmonary artery catheterization. Critical care medicine. 1990 Jan:18(1):122-3 [PubMed PMID: 2293963]
Level 3 (low-level) evidenceA clinical and follow-up study of right and left bundle branch block., Rotman M,Triebwasser JH,, Circulation, 1975 Mar [PubMed PMID: 1132086]
Horowitz LN, Alexander JA, Edmunds LH Jr. Postoperative right bundle branch block: identification of three levels of block. Circulation. 1980 Aug:62(2):319-28 [PubMed PMID: 7397974]
Ohmae M, Rabkin SW. Hyperkalemia-induced bundle branch block and complete heart block. Clinical cardiology. 1981 Jan:4(1):43-6 [PubMed PMID: 7226590]
Level 3 (low-level) evidenceStein PD, Matta F, Sabra MJ, Treadaway B, Vijapura C, Warren R, Joshi P, Sadiq M, Kofoed JT, Hughes P, Chabala SD, Keyes DC, Kakish E, Hughes MJ. Relation of electrocardiographic changes in pulmonary embolism to right ventricular enlargement. The American journal of cardiology. 2013 Dec 15:112(12):1958-61. doi: 10.1016/j.amjcard.2013.08.030. Epub 2013 Sep 25 [PubMed PMID: 24075285]
Level 2 (mid-level) evidenceAgarwal S,Tuzcu EM,Desai MY,Smedira N,Lever HM,Lytle BW,Kapadia SR, Updated meta-analysis of septal alcohol ablation versus myectomy for hypertrophic cardiomyopathy. Journal of the American College of Cardiology. 2010 Feb 23 [PubMed PMID: 20170823]
Level 1 (high-level) evidenceLENEGRE J. ETIOLOGY AND PATHOLOGY OF BILATERAL BUNDLE BRANCH BLOCK IN RELATION TO COMPLETE HEART BLOCK. Progress in cardiovascular diseases. 1964 Mar:6():409-44 [PubMed PMID: 14153648]
LEV M. ANATOMIC BASIS FOR ATRIOVENTRICULAR BLOCK. The American journal of medicine. 1964 Nov:37():742-8 [PubMed PMID: 14237429]
Denes P, Wu D, Dhingra RC, Amat-y-leon F, Wyndham C, Rosen KM. Eectrophysiological observations in pateints with rate dependent bundle branch block. Circulation. 1975 Feb:51(2):244-50 [PubMed PMID: 1112004]
Eriksson P,Hansson PO,Eriksson H,Dellborg M, Bundle-branch block in a general male population: the study of men born 1913. Circulation. 1998 Dec 1 [PubMed PMID: 9832497]
Arnsdorf MF. The cellular basis of cardiac arrhythmias. A matrical perspective. Annals of the New York Academy of Sciences. 1990:601():263-80 [PubMed PMID: 2221691]
Level 3 (low-level) evidenceLEATHAM A. Splitting of the first and second heart sounds. Lancet (London, England). 1954 Sep 25:267(6839):607-14 [PubMed PMID: 13202450]
Surawicz B, Childers R, Deal BJ, Gettes LS, Bailey JJ, Gorgels A, Hancock EW, Josephson M, Kligfield P, Kors JA, Macfarlane P, Mason JW, Mirvis DM, Okin P, Pahlm O, Rautaharju PM, van Herpen G, Wagner GS, Wellens H, American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology, American College of Cardiology Foundation, Heart Rhythm Society. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. Journal of the American College of Cardiology. 2009 Mar 17:53(11):976-81. doi: 10.1016/j.jacc.2008.12.013. Epub [PubMed PMID: 19281930]
Bilchick KC, Kamath S, DiMarco JP, Stukenborg GJ. Bundle-branch block morphology and other predictors of outcome after cardiac resynchronization therapy in Medicare patients. Circulation. 2010 Nov 16:122(20):2022-30. doi: 10.1161/CIRCULATIONAHA.110.956011. Epub 2010 Nov 1 [PubMed PMID: 21041691]
Level 2 (mid-level) evidenceThe Brugada syndrome: clinical, electrophysiologic and genetic aspects., Gussak I,Antzelevitch C,Bjerregaard P,Towbin JA,Chaitman BR,, Journal of the American College of Cardiology, 1999 Jan [PubMed PMID: 9935001]
Okmen E, Erdinler I, Oguz E, Akyol A, Turek O, Cam N, Ulufer T. An electrocardiographic algorithm for determining the location of pacemaker electrode in patients with right bundle branch block configuration during permanent ventricular pacing. Angiology. 2006 Oct-Nov:57(5):623-30 [PubMed PMID: 17067986]
Zhang ZM, Rautaharju PM, Soliman EZ, Manson JE, Cain ME, Martin LW, Bavry AA, Mehta L, Vitolins M, Prineas RJ. Mortality risk associated with bundle branch blocks and related repolarization abnormalities (from the Women's Health Initiative [WHI]). The American journal of cardiology. 2012 Nov 15:110(10):1489-95. doi: 10.1016/j.amjcard.2012.06.060. Epub 2012 Aug 2 [PubMed PMID: 22858187]
Level 2 (mid-level) evidenceWagner GS, Macfarlane P, Wellens H, Josephson M, Gorgels A, Mirvis DM, Pahlm O, Surawicz B, Kligfield P, Childers R, Gettes LS, Bailey JJ, Deal BJ, Gorgels A, Hancock EW, Kors JA, Mason JW, Okin P, Rautaharju PM, van Herpen G, American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology, American College of Cardiology Foundation, Heart Rhythm Society. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part VI: acute ischemia/infarction: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. Journal of the American College of Cardiology. 2009 Mar 17:53(11):1003-11. doi: 10.1016/j.jacc.2008.12.016. Epub [PubMed PMID: 19281933]