Definition/Introduction
Heart dominance is described by the coronary artery branch giving off the posterior descending artery and supplying the inferior wall, characterized as left, right, or codominant. The posterior descending artery (PDA) is also known as the posterior interventricular artery because it runs along the posterior interventricular sulcus to the apex of the heart. It is at the apex where it meets the left anterior descending artery traveling along the heart's anterior surface. The posterior descending artery supplies the posterior third of the interventricular septum, including the posterior and inferior walls of the left ventricle. The vessel most commonly originates from either the right coronary artery (right dominant), left circumflex artery (left dominant), or both (codominant).
There have been physiologic variants described in case reports, such as an origin from the left anterior descending artery, referred to as "superdominant."[1][2][3] Estimates show that 70% to 80% of the population is right-heart dominant, with the posterior descending artery originating from the right coronary artery. Approximately 5% to 10% of the population is left-heart dominant, with the PDA originating from the left circumflex artery, and about 10% to 20% is codominant with the PDA supplied by both the left circumflex artery and right coronary artery.[4] Small branches from the dominant artery perfuse the atrioventricular node.[5] Theoretically, decreased perfusion to the atrioventricular node may result in dysfunction, adding further significance to the cardiac dominance of the patient (see Image. Coronary Arteries).
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
As with any coronary artery, the posterior descending artery is subject to possible stenosis or occlusion secondary to atheromatous plaque accumulation or thrombosis. The result of stenosis to the posterior descending artery would be decreased perfusion or even infarction of the posterior third of the interventricular septum, depending on the severity. Therefore, the location of the possible infarction or reduced perfusion depends on the individual's cardiac dominance. For example, a patient who is left-heart dominant and suffering from severe stenosis of the proximal left main coronary artery may suffer infarction of the posterior interventricular septum. However, this would not be true in a patient with codominant coronary circulation. A stenotic lesion to the proximal left main coronary artery would decrease perfusion to the posterior interventricular septum. However, it would still receive blood via the right coronary artery, reducing the risk of an infarct.
In right-dominant coronary circulation, the posterior descending artery is a collateral vessel to the basal left anterior descending artery through septal perforators.[6] This would mean that a patient with proximal left anterior descending coronary artery stenosis has the additional benefit of possibly receiving supply from the right coronary artery if he or she is right-heart dominant. This collateral circulation may be enough to bypass the blockage in the left anterior descending artery to provide enough oxygenated blood to allow the cardiac muscle to survive and recover.
Clinical Significance
Cardiac dominance is essential in cardiac surgery, particularly coronary artery bypass grafting. Cardiac dominance is determined through cardiac catheterization, which involves the insertion of a catheter into the ostium of the left main coronary artery and the right coronary artery and the injection of radiocontrast dye to allow visualization of coronary arteries. In coronary artery bypass grafting procedures, precise knowledge of patient-specific coronary anatomy is crucial because the surgeon must identify which vessels are suitable to receive the distal anastomosis of the venous graft. The posterior descending artery may be suitable for occlusion of the right or left coronary artery, depending on its patency. The venous conduit is then sutured into a portion of the right coronary artery distal to the occlusion.
Many studies have been conducted to determine the significance of cardiac dominance on patient outcomes and pathology. One study revealed that patients with left coronary dominance have a reduced prognosis in surgical myocardial revascularization. The exact reason remains undetermined, but speculation is that there is an association with collateral circulation seen in right heart-dominant patients that is absent in left heart-dominant subjects.[7]
Left-heart dominance was described to be a high-risk feature for percutaneous coronary intervention as well. Left-heart–dominant patients undergoing percutaneous coronary intervention have higher in-hospital mortality and are more likely to present with symptoms of heart failure, cardiogenic shock, or cardiac arrest.[8] Left-heart dominance in patients undergoing aortic valve replacement for severe aortic stenosis was also shown to be an independent risk factor. There appears to be an increased prevalence of left-heart dominance in patients undergoing aortic valve replacement, and the left main coronary artery is significantly shorter than those seen in right-heart–dominant patients; this may be evidence of a developmental relationship seen in left-heart–dominant patients between the left main coronary artery and aortic valve. In one study, patients with left dominant coronary circulation were determined to suffer a significantly higher rate of perioperative myocardial infarction compared to right heart dominant or codominant patients.[9]
These studies and trials highlight the significance of determining dominance in coronary artery anatomy in treating cardiac pathology. The increased risk seems to correlate with left- heart–dominant circulation. Still, more research must be done to determine if different strategies must be implemented to ensure better outcomes.
Media
(Click Image to Enlarge)
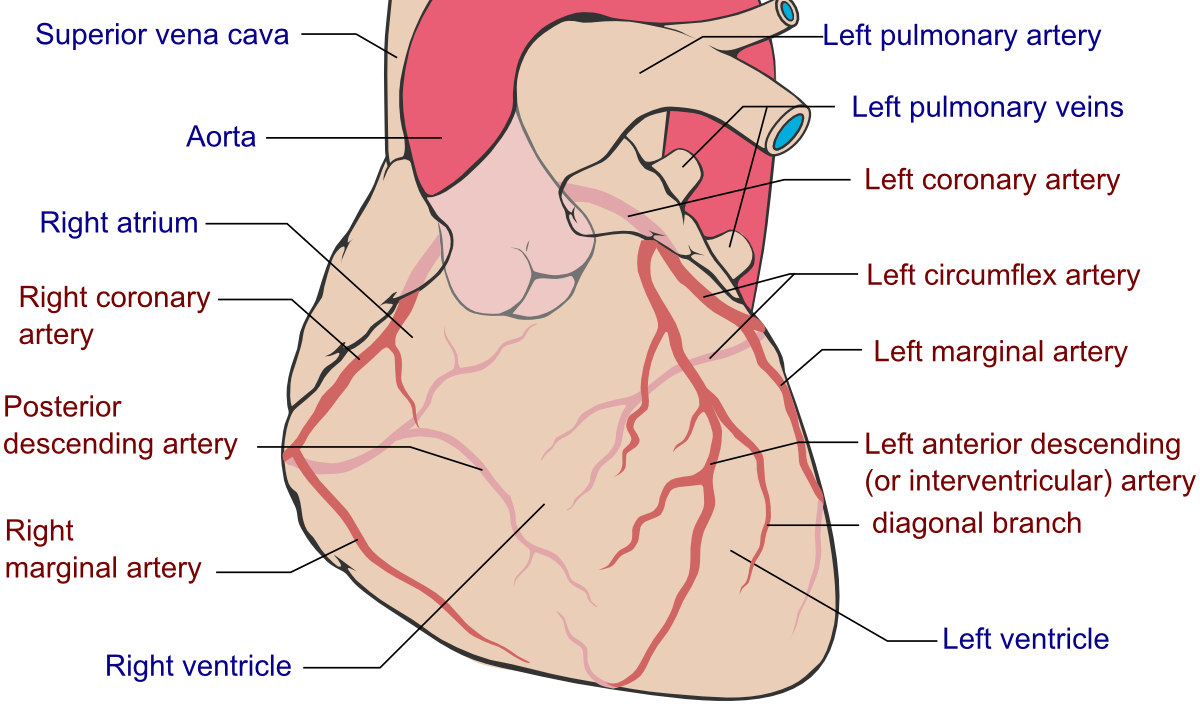
Coronary Arteries
Patrick J. Lynch, Fred the Oyster, Mikael H Häggström, Public Domain, via Wikimedia Commons.
References
John LC. Anomalous origin of the posterior descending artery from the left anterior descending coronary artery: cardiac surgeons beware. Heart (British Cardiac Society). 2002 Feb:87(2):161 [PubMed PMID: 11796560]
Level 3 (low-level) evidenceClark VL, Brymer JF, Lakier JB. Posterior descending artery origin from the left anterior descending: an unusual coronary artery variant. Catheterization and cardiovascular diagnosis. 1985:11(2):167-71 [PubMed PMID: 3872720]
Level 3 (low-level) evidenceShaikh SSA, Munde K, Patil V, Phutane M, Singla R, Khan Z, Bansal NO. "Superdominant" Left Anterior Descending Artery Continuing as Posterior Descending Artery: Extremely Rare Coronary Artery Anomaly. Cardiology research. 2018 Aug:9(4):253-257. doi: 10.14740/cr738w. Epub 2018 Aug 10 [PubMed PMID: 30116455]
Shriki JE, Shinbane JS, Rashid MA, Hindoyan A, Withey JG, DeFrance A, Cunningham M, Oliveira GR, Warren BH, Wilcox A. Identifying, characterizing, and classifying congenital anomalies of the coronary arteries. Radiographics : a review publication of the Radiological Society of North America, Inc. 2012 Mar-Apr:32(2):453-68. doi: 10.1148/rg.322115097. Epub [PubMed PMID: 22411942]
Villa AD, Sammut E, Nair A, Rajani R, Bonamini R, Chiribiri A. Coronary artery anomalies overview: The normal and the abnormal. World journal of radiology. 2016 Jun 28:8(6):537-55. doi: 10.4329/wjr.v8.i6.537. Epub [PubMed PMID: 27358682]
Level 3 (low-level) evidenceNishimura S, Ohshima S, Kato K, Daida H, Nishiyama S, Nakanishi S, Kondo K, Seki A, Yamaguchi H. [Coronary collaterals in patients with total obstruction of the proximal left anterior descending artery: their pathways and functional significance]. Journal of cardiography. 1985 Dec:15(4):969-79 [PubMed PMID: 3841911]
Omerbasic E, Hasanovic A, Omerbasic A, Pandur S. Prognostic value of anatomical dominance of coronary circulation in patients with surgical myocardial revascularization. Medical archives (Sarajevo, Bosnia and Herzegovina). 2015 Feb:69(1):6-9. doi: 10.5455/medarh.2015.69.6-9. Epub 2015 Feb 21 [PubMed PMID: 25870467]
Kuno T, Numasawa Y, Miyata H, Takahashi T, Sueyoshi K, Ohki T, Negishi K, Kawamura A, Kohsaka S, Fukuda K. Impact of coronary dominance on in-hospital outcomes after percutaneous coronary intervention in patients with acute coronary syndrome. PloS one. 2013:8(8):e72672. doi: 10.1371/journal.pone.0072672. Epub 2013 Aug 26 [PubMed PMID: 23991136]
Murphy ES, Rösch J, Rahimtoola SH. Frequency and significance of coronary arterial dominance in isolated aortic stenosis. The American journal of cardiology. 1977 Apr:39(4):505-9 [PubMed PMID: 848434]