Introduction
The nervous system is a complex network that enables an organism to interact with its surroundings. Sensory components that detect environmental stimuli and motor components that provide skeletal, cardiac, and smooth muscle control and control of glandular secretions are coordinated in a system to compel appropriate motor responses to the stimuli or sensory inputs that have been received, stored, and processed.
The nervous system comprises vast neural networks; signaling within these circuits enables thinking, language, feeling, learning, memory, and all functions and sensations. It is well-established that through the plasticity of existing cells, our nervous systems can adapt to situations not previously encountered. Still, it also has been shown that neural stem cells (NSCs) are plastic and involved in creating new connections in adaptation and response to injury. NSCs play a fundamental role in development and the ability to respond to stimuli in the environment and injury.[1][2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The nervous system can be divided into the peripheral and central (CNS). The brain is divided into four main parts: (1) the brain stem, consisting of the medulla, pons, and midbrain; (2) the cerebellum; (3) the diencephalon, with the thalamus and hypothalamus; and (4) the cerebral hemispheres, comprised of the cerebral cortex, basal ganglia, white matter, hippocampi, and amygdalae. See Images. Peripheral and Central Nervous Systems and Schematic Diagram of the Major CNS.
Cranial nerves III—XII arise from the brainstem and provide sensory innervation to the head and neck, with some function extension into the region of the trapezius muscle through the spinal accessory nerve. The medulla is a rostral continuation of the spinal cord and contains autonomic centers that control vital functions and systems involved in breathing and the maintenance of appropriate blood pressure. These centers also regulate diaphragmatic and pharyngeal reflexes. The pons are located between the medulla and midbrain and contribute to maintaining posture, balance, and breathing. The pons carry information from the cerebrum to the cerebellum through the corticopontocerebellar tract. The midbrain is the most rostral portion of the brainstem. It is involved in ocular movement and visual and auditory relay pathways via the lateral and medial geniculate nuclei, respectively.
The cerebellum lies in the posterior fossa and coordinates head and eye movements, movement planning and execution, and posture maintenance. In addition to its well-established role in motor function, the cerebellum is a critical component of many cognitive and sensory-motor processes, including auditory pathways involved in functions such as speech recognition.
The thalamus and hypothalamus are located between the cerebral hemispheres and the brain stem. The thalamus is a major processing region for sensory information going to the cerebral cortex and motor information traveling in the opposite direction toward the brainstem and spinal cord. The hypothalamus controls pituitary gland secretions by secreting hormones into the hypophysial portal blood that either stimulate or inhibit the release of anterior pituitary hormones. Cell bodies located in the hypothalamus also control the secretions of the posterior pituitary, which include antidiuretic hormone and oxytocin.
The basal ganglia or basal nuclei include the putamen, caudate, globus pallidus, ventral striatum, ventral pallidum, substantia nigra, and subthalamic nucleus. These nuclei receive input from nearly the entire neocortex and then project through basal ganglia-thalamocortical circuits to a relatively small part of the frontal lobe to aid in movement regulation. The hippocampus is primarily involved with memory, and the amygdala processes emotional information that affects the autonomic system through the hypothalamus and hormone secretion. The cerebral cortex is largely involved in perception and higher motor function through the processing of sensory information and integrating motor functions. The cortex contains primary, secondary, and tertiary sensory and motor areas. Cortical function centers around its ability to integrate diverse signals and provide direction in response.
The spinal cord is the caudal extension of the CNS. The spinal cord, as is the spinal column, is segmented and projects 31 pairs of spinal nerves (with afferent and efferent components). There are 8 cervical spinal nerves, 12 pairs of thoracic nerves, 5 pairs of lumbar nerves, 5 pairs of sacral nerves, and 1 pair of coccygeal nerves. The afferent nerves comprise the sensory nerves and carry information from the skin, joints, muscles, and visceral organs. In contrast, the efferent nerves comprise the somatic and autonomic motor nerves and innervate skeletal, cardiac, and smooth muscle, as well as glandular tissue and secretory cells. The spinal cord transmits signals between the periphery and the rest of the CNS through ascending and descending pathways. Due to unequal growth during development, the spinal cord is shorter than the spinal column, with the cell bodies of the spinal nerves ending around the level of L1/L2 at the conus medullaris. The cauda equina, which consists of spinal nerves L2 through C1, continues caudally in the lumbar cistern ( subarachnoid space) as the spinal nerves leave the spinal column at their respective levels. This subarachnoid space devoid of the spinal cord enables the safe performance of lumbar punctures, typically between the L3 and L4 or L4 and L5 vertebral bodies.
Impulse transmission throughout the nervous system is conducted via neurons employing synaptic connections. Consequently, both electrical and chemical components are involved in signal transmission. A variety of neurotransmitters are used in various synapses, neuroeffector, and neuromuscular junctions; examples include acetylcholine, norepinephrine, dopamine, serotonin, glutamate, gamma-aminobutyric acid, neuropeptides, hormones, and even nitric oxide. Ion concentrations also play a significant role in impulse generation and conduction. It is of consequent importance that healthy ion balances be maintained by using active transport. The heavy use of Na+/K+-ATPase accounts for the neural demand for glucose. It has also been shown that calcium is necessary for excitation at neuromuscular junctions and ganglionic synapses and that magnesium inhibits excitability.[3][4][5][6][7][8][9][10][11][12][13]
Embryology
The formation of the nervous system begins with the process called neurulation, which follows gastrulation and results in the development of the neural tube. During week 3 of development, the notochord secretes signaling factors to induce the transformation of the overlying ectoderm to neuroectoderm and the formation of the neural plate. The neural tube is formed through folding and closing the neural folds. In the formation of the spinal cord, the basal plate, largely expressing Sonic hedgehog, induces the differentiation of motor areas ventrally, and the alar plate, primarily expressing bone morphogenic proteins and Wnt factors, induces sensory area formation dorsally. It should be noted that these signaling factors induce appropriate development along a concentration gradient with the involvement of modulating factors and other signaling factors unmentioned here; the plates and their effects are not segregated.
The cranial parts of the CNS are formed from the prosencephalon, mesencephalon, and rhombencephalon (cranial to caudal) present during week 4 of development. In week 5, the prosencephalon develops into the telencephalon and diencephalon, and the rhombencephalon becomes the metencephalon and myelencephalon. The telencephalon ultimately becomes the cerebral hemispheres and basal nuclei; the diencephalon develops into the thalamus, hypothalamus, and retinas; the mesencephalon gives rise to the midbrain, including superior and inferior colliculi; the metencephalon becomes the pons and cerebellum; the myelencephalon forms the medulla.[14]
Nerves
Some of the largest nerves in the body include the sciatic nerve, the femoral nerve, the obturator nerve, the median nerve, the ulnar nerve, the radial nerve, and the musculocutaneous nerve. The sciatic nerve is the largest in the body and is divided into tibial and fibular parts, the distal extensions of which become the tibial and common fibular (peroneal) nerves. The common fibular nerve splits into the deep and superficial fibular nerves. The sciatic nerve innervates the posterior compartment of the thigh. The tibial nerve innervates the posterior compartment of the leg. The fibular nerves innervate the anterior and lateral compartments of the leg. The brachial plexus derives from the nerves of the upper limb. The median nerve primarily innervates the lateral portion of the antebrachium and hand, and the ulnar nerve innervates the medial portion. The radial nerve and its branches innervate the posterior of the entire arm and hand. The musculocutaneous nerve innervates the elbow flexors and provides sensory innervation to the lateral antebrachium.
Surgical Considerations
The specialty involved in the surgery of pathologies involving the CNS is neurosurgery.
Clinical Significance
Many neurological conditions affect the CNS. They range dramatically in scope, impact, and nature of the effect. Some conditions can lead to progressively impaired movement, such as in Parkinson disease. Huntington chorea and hemiballismus cause excessive movement, among other symptoms. The demyelination in multiple sclerosis can cause acute attacks and, over time, chronic degradation of function. Others may impact cognition, such as the various dementias. Epilepsy can cause uncontrolled excitation. Headaches often impair the daily function of patients. Traumatic injuries can cause plegia or paresis and may result in any number of deficits depending on the location and extent of the lesion.[15]
Media
(Click Image to Enlarge)
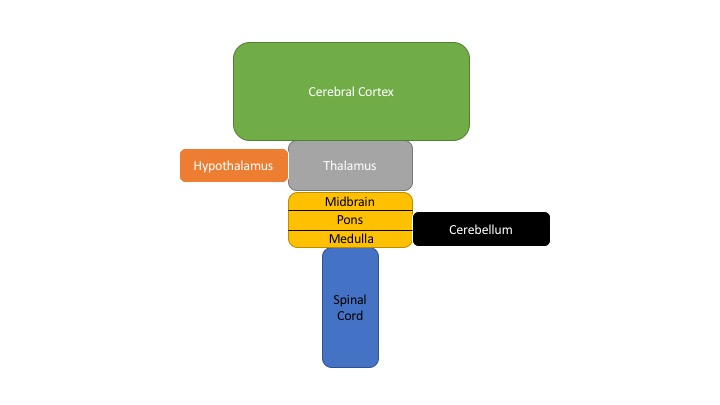
Schematic Diagram of the Major CNS Components
Contributed by P Ludwig
(Click Image to Enlarge)
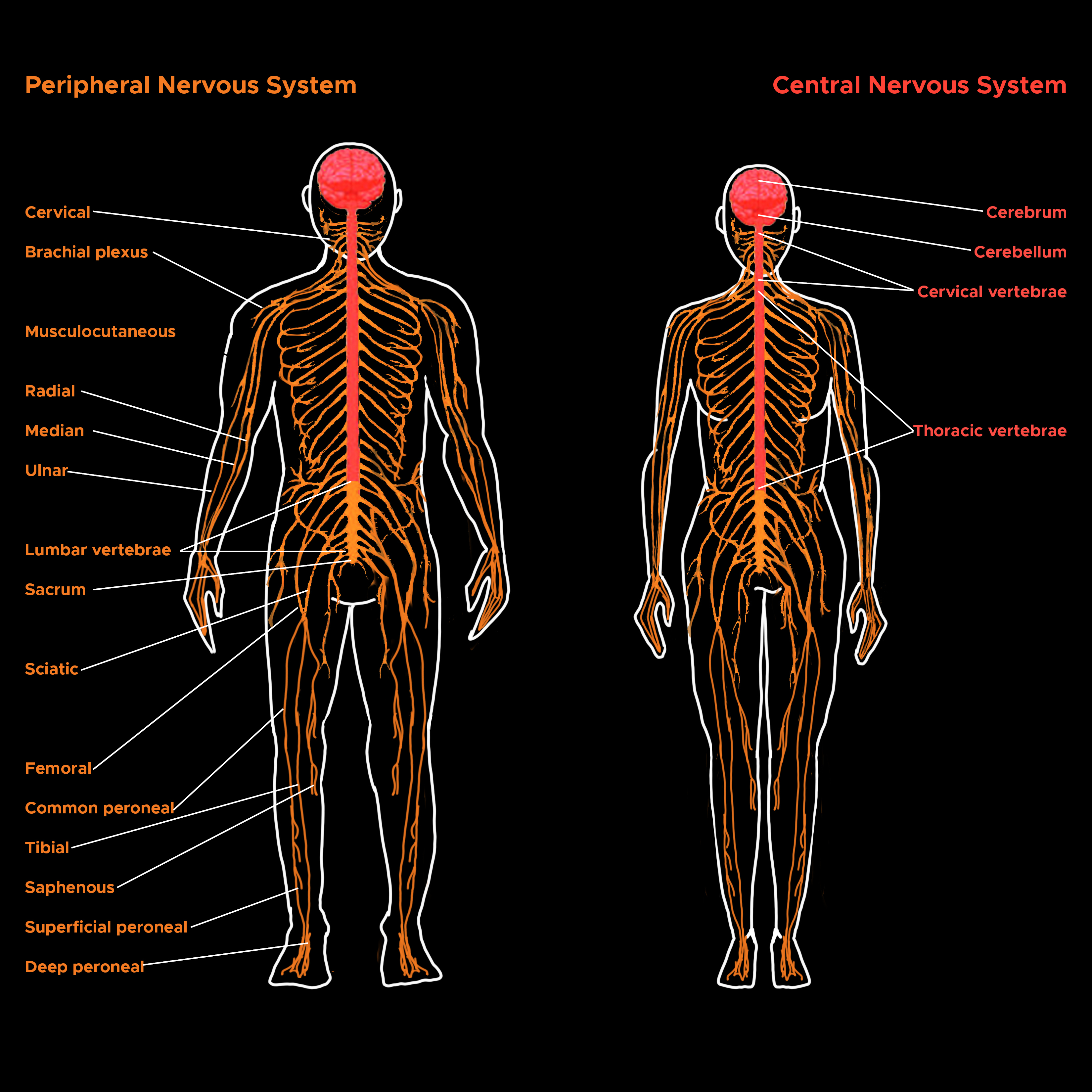
Peripheral and Central Nervous Systems. Illustration of the peripheral and central nervous systems: brain, spinal cord, and nerves.
Contributed by C Rowe
References
Galli R, Gritti A, Bonfanti L, Vescovi AL. Neural stem cells: an overview. Circulation research. 2003 Apr 4:92(6):598-608 [PubMed PMID: 12676811]
Level 3 (low-level) evidenceKennea NL, Mehmet H. Neural stem cells. The Journal of pathology. 2002 Jul:197(4):536-50 [PubMed PMID: 12115869]
Henn FA, Haljamäe H, Hamberger A. Glial cell function: active control of extracellular K + concentration. Brain research. 1972 Aug 25:43(2):437-43 [PubMed PMID: 4262289]
Level 3 (low-level) evidenceKatz B, Miledi R. A study of synaptic transmission in the absence of nerve impulses. The Journal of physiology. 1967 Sep:192(2):407-36 [PubMed PMID: 4383089]
Level 3 (low-level) evidenceSiegel JH, Relkin EM. Antagonistic effects of perilymphatic calcium and magnesium on the activity of single cochlear afferent neurons. Hearing research. 1987:28(2-3):131-47 [PubMed PMID: 3654385]
Level 3 (low-level) evidencePhelps EA, LeDoux JE. Contributions of the amygdala to emotion processing: from animal models to human behavior. Neuron. 2005 Oct 20:48(2):175-87 [PubMed PMID: 16242399]
Level 3 (low-level) evidenceScoville WB, Milner B. Loss of recent memory after bilateral hippocampal lesions. 1957. The Journal of neuropsychiatry and clinical neurosciences. 2000 Winter:12(1):103-13 [PubMed PMID: 10678523]
Alexander GE, DeLong MR, Strick PL. Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annual review of neuroscience. 1986:9():357-81 [PubMed PMID: 3085570]
Level 3 (low-level) evidenceMcLachlan NM, Wilson SJ. The Contribution of Brainstem and Cerebellar Pathways to Auditory Recognition. Frontiers in psychology. 2017:8():265. doi: 10.3389/fpsyg.2017.00265. Epub 2017 Mar 20 [PubMed PMID: 28373850]
Tziridis K, Dicke PW, Thier P. Pontine reference frames for the sensory guidance of movement. Cerebral cortex (New York, N.Y. : 1991). 2012 Feb:22(2):345-62. doi: 10.1093/cercor/bhr109. Epub 2011 Jun 13 [PubMed PMID: 21670098]
Level 3 (low-level) evidenceBrain peptides as neurotransmitters., Snyder SH,, Science (New York, N.Y.), 1980 Aug 29 [PubMed PMID: 6157191]
Level 3 (low-level) evidenceBult H, Boeckxstaens GE, Pelckmans PA, Jordaens FH, Van Maercke YM, Herman AG. Nitric oxide as an inhibitory non-adrenergic non-cholinergic neurotransmitter. Nature. 1990 May 24:345(6273):346-7 [PubMed PMID: 1971425]
Level 3 (low-level) evidenceHarvey AM, Macintosh FC. Calcium and synaptic transmission in a sympathetic ganglion. The Journal of physiology. 1940 Jan 15:97(3):408-16 [PubMed PMID: 16995173]
Imitola J, Raddassi K, Park KI, Mueller FJ, Nieto M, Teng YD, Frenkel D, Li J, Sidman RL, Walsh CA, Snyder EY, Khoury SJ. Directed migration of neural stem cells to sites of CNS injury by the stromal cell-derived factor 1alpha/CXC chemokine receptor 4 pathway. Proceedings of the National Academy of Sciences of the United States of America. 2004 Dec 28:101(52):18117-22 [PubMed PMID: 15608062]
Level 3 (low-level) evidenceZola-Morgan S, Squire LR, Amaral DG. Human amnesia and the medial temporal region: enduring memory impairment following a bilateral lesion limited to field CA1 of the hippocampus. The Journal of neuroscience : the official journal of the Society for Neuroscience. 1986 Oct:6(10):2950-67 [PubMed PMID: 3760943]
Level 3 (low-level) evidence