Introduction
The brain consists of the cerebrum, cerebellum, and brainstem. Taking up the majority of the brain space is the cerebrum. The cerebrum controls somatosensory, motor, language, cognitive thought, memory, emotions, hearing, and vision. The cerebrum is divided into the left and right hemispheres by a deep longitudinal fissure; the two hemispheres remain in contact and communication with one another by the corpus callosum. Each hemisphere further subdivides into a frontal, parietal, occipital, and temporal lobe. Each lobe carries out different functions.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The surface of the cerebrum is known as the cortex. It is about two-millimeter-thick and has many folds forming ridges (gyri) and grooves (sulci). A fissure is a deeper grove and is often used interchangeably with sulcus. The cerebrum is divided into a left and right hemisphere by a longitudinal fissure that goes by many different names: longitudinal fissure, cerebral fissure, median longitudinal fissure, interhemispheric fissure. Each cerebral hemisphere divides into four separate lobes by a central sulcus, parieto-occipital sulcus, and lateral fissure. The central sulcus runs posterior-medial to anterior-lateral and separates the frontal lobe from the parietal lobe. The parieto-occipital sulcus separates the parietal lobe from the occipital lobe. The lateral fissure (Sylvian fissure) is a laterally located horizontal fissure and separates the temporal lobe from the frontal and parietal lobe.
Frontal Lobe
The frontal lobe is anterior to the central sulcus and superior to the lateral fissure. The frontal lobe further divides into a superior, middle, and inferior frontal gyrus, primary motor cortex, and orbital area. These areas combine to controls our executive and motor functions. It controls judgment, problem-solving, planning, behavior, personality, speech, writing, speaking, concentration, self-awareness, and intelligence. The primary motor cortex is present in the precentral gyrus of the frontal lobe and is positioned immediately anterior to the central sulcus. The premotor cortex is anterior to the primary motor cortex. This area controls the contralateral body and extremity movement. The medial region controls the lower extremity. The superior-lateral region controls the upper extremity and hand. The lateral region controls the face. Certain body parts are more richly innervated thus does not proportionally represent the human body. In fact, the majority of the primary motor cortex is used to finely control the muscle of the hands, face, and lips, which is well represented by the homunculus model. Within the middle frontal gyrus is the frontal eye field area and is mostly responsible for the contralateral eye abduction and ipsilateral eye adduction. Broca's area is responsible for speech and is not present in both hemispheres. Instead, it is within the inferior frontal gyrus of the dominant hemisphere. The dominant hemisphere, in most individuals, is the left hemisphere. Therefore, Broca's area is most common in the left inferior frontal gyrus.[1]
Parietal Lobe
The parietal lobe is posterior to the central sulcus and anterior to the parieto-occipital sulcus. This lobe controls perception and sensation. The primary somatosensory cortex is in the postcentral gyrus and is positioned immediately posterior to the central sulcus. The primary somatosensory cortex controls the sense of touch, temperature, and pain of the contralateral body. Mirroring the primary motor cortex, the medial region senses the lower extremity, superior-lateral region sense the upper extremity and hand, and the lateral region senses the face. Similar to the primary motor area, the hands, face, and lips take up the majority of the somatosensory area and are also well presented by the homunculus model. Damage to the parietal lobe can present with a lack of these sensations as well as other symptoms depending on whether the dominant or nondominant hemisphere is farther damage. Damage to the dominant parietal lobe, usually the left hemisphere, present with agraphia, acalculia, finger agnosia, and left-right disorientation. The presentation of these symptoms is characteristic of Gerstmann Syndrome.[2] Damage to the nondominant parietal lobe, usually the right hemisphere, present with agnosia of the contralateral side of the world - this is also called hemispatial neglect syndrome.
Occipital Lobe
The occipital lobe is posterior to the parieto-occipital sulcus and superior to the tentorium cerebelli. This lobe interprets vision, distance, depth, color, and facial recognition. The occipital lobe receives its information from the contralateral vision field of both eyes (i.e., the left occipital lobe receives and interprets information from the right visual field from both the left and right eye).[3]
Temporal Lobe
The temporal lobe is inferior to the lateral fissure and further divides into a superior, middle, and inferior temporal gyrus. This lobe controls language comprehension, hearing, and memory. Wernicke's area is responsible for language comprehension, and it not found in both hemispheres. Similar to Broca's area, Wernicke's area is in the superior temporal gyrus of the dominant hemisphere, which is usually the left hemisphere. Therefore, the location of Wernicke's area is most commonly in the superior temporal gyrus. The primary auditory cortex is in the superior temporal gyrus and processes most auditory information from the contralateral ear and some from the ipsilateral ear. The temporal lobe communicates with the hippocampus and amygdala to form memories.[4]
Nerves that travel to and from the brain consist of dendrites, a cell body, axon, and axon terminal. Grey matter is commonly used interchangeably with the cortex. However, the grey matter implies that axons that are not myelinated appear grey. Grey matter can be found in deep structures, as well. Below the cortex sits white matter, which implies that axons are myelinated and appear white. White matter receives and send signals to and from the brain and allows for communication between different part of the brain quickly due to their myelinated axons. The grey matter of the cortex interprets signals received from different parts of the body and then sends out a response signal.
Embryology
The notochord sends signals and induces the overlying ectoderm to form the neural tube that will create the entire nervous system. By week four, the neural tube form into the forebrain (prosencephalon), midbrain (mesencephalon), and hindbrain (rhombencephalon). The forebrain develops into the telencephalon and diencephalon. The telencephalon develops into the cerebral hemispheres.[5]
Blood Supply and Lymphatics
The blood to the brain receives vascular supply by the left and right internal carotid arteries and the left and right vertebral arteries. The two vertebral arteries course posteriorly and combine to form the basilar artery. The internal carotid and basilar arteries join at the base of the brain, where they form an anastomosis called the circle of Willis. From the circle, an anterior, middle, and posterior cerebral artery branches off and supply different areas of each hemisphere. The internal carotid arteries supply blood to the anterior and middle arteries. The vertebral arteries supply blood to the posterior cerebral arteries.[6][7][8][9]
The anterior cerebral artery supplies the anteromedial surface of each hemisphere. The anteromedial surface of each hemisphere contains the motor and somatosensory region that controls the contralateral lower limb motor and senes. The middle cerebral artery delivers vascular supply to the lateral surface of each hemisphere. Important areas within the lateral surface are the motor and somatosensory region of the contralateral upper limb and face. Additionally, there are also Broca's area, Wernicke's area, dominant hemisphere, and nondominant hemispheres. The posterior cerebral artery supplies the posterior and inferior surfaces of each hemisphere. The posterior cerebral artery supplies the occipital lobe. Watershed regions are areas in the brain that sit between two cerebral arteries. These regions receive dual supply from distal branches of the cerebral arteries.
Vein drains the cortex and the deeper brain into a series of sinuses that eventually flows into the internal jugular veins. The venous system divides into a superficial and deep system. Draining the superficial surface of both hemispheres is the sagittal sinuses. The posterior region gets drained into the transverse sinuses. Deeper structures get drained into the great cerebral brain of Galen and straight sinus. These sinuses drain into the internal jugular veins and the right heart.[10][11]
Physiologic Variants
Holoprosencephaly
Failure of the forebrain to separate into the left and right hemisphere will result in holoprosencephaly. There are different degrees of severity of holoprosencephaly, from incomplete separation to no separation of the hemispheres. Moderate holoprosencephaly can present with cleft lip and palate. The severe form may present with cyclopia. Holoprosencephaly can be seen in trisomy 13 and can also be present in other chromosomal abnormality as well.[12]
Anencephaly
Failure of the rostral neural tube to form results in anencephaly, a congenital defect where the brain, scalp, and skull do not form. An infant with anencephaly is mostly stillborn, and those that do survive dies within hours or weeks.[13]
Lissencephaly
Lissencephaly is a disorder where the brain fails to form folds resulting in a lack of sulci and gyri.[14]
Surgical Considerations
Patients that have drug resistance epilepsy may benefit from surgical removal of the epileptogenic area — determining where the epileptogenic zone is the first important step. If the zone is in proximity to any the crucial area of the brain that is key to everyday life such Broca or Wernicke area, further consideration and planning is needed to determine if the zone is safe for resection.
Similar things pertain to brain tumors. Determine the location and deciding it is safe to remove it.
Clinical Significance
One of the clinical significance of knowing different areas, functions, and arterial supplies of the cerebral hemispheres is knowing which area of the brain suffered damage in a stroke. The anterior cerebral artery supplies the motor and somatosensory of the contralateral lower limb. Therefore, anything affecting the normal flow of blood to the anterior cerebral artery will result in motor weakness and sensory loss in the contralateral lower limb. The middle cerebral artery supplies the motor and somatosensory of the contralateral face, lip, and upper limb. Therefore, anything affecting the normal flow of blood to the middle cerebral artery will result in motor weakness and sensory loss in the contralateral face, lip, and upper limb.[8] If the left middle cerebral artery is affected, Broca and Wernicke area (usually left hemisphere) can also be affected. An individual will present with difficulty speaking and understanding. The posterior cerebral artery supplies the occipital lobe of the contralateral visual field. Therefore, anything affecting the flow of blood to the posterior cerebral artery can present with contralateral hemianopia. Once a stroke is recognized, it is essential to determine whether the cause is ischemic or hemorrhage because management is different. Recognizing the signs and symptoms of a stroke is important because the longer a stroke goes untreated, the worse the prognosis and sequela.
Aneurysm of the cerebral arteries can affect blood flow and compress the cerebral hemispheres and present differently depending on which area is affected. The most common site of an aneurysm is the anterior cerebral and the anterior communicating artery. Aneurysm of the anterior cerebral artery can present with contralateral lower limb numbness and weakness, while aneurysm of the middle cerebral artery can present with contralateral facial and upper limb numbness and weakness. Most aneurysm, however, is clinically silent until rupture resulting in subarachnoid hemorrhage and present with a severe headache.
Other Issues
Any conditions that affect the cerebrum and its grey and white matter can alter its normal function. The hemispheres may develop primary brain tumors. Glioblastoma multiforme is a malignant primary brain tumor that is commonly found in the cerebral hemisphere and can cross the corpus callosum. Oligodendroglioma is another primary brain tumor that commonly affects the frontal lobe. Meningioma may compress adjacent cerebral structures. Multiple sclerosis is the autoimmune and demyelination of the brain and spinal cord. Most often affects white women in their 20s and 30s and present with scanning speech, intention tremor, and nystagmus. One of the tools used diagnosed multiple sclerosis is to visualize periventricular plaque on magnetic resonance imaging (MRI), which represents areas of demyelination of axons.
A neurodegenerative disorder that affects the cortices results in a decrease in cognitive abilities and memory. One of the most common etiologies of dementia in the elderly population is Alzheimer disease and results from widespread cortical atrophy. The second most common origin of dementia is vascular dementia, which is caused by multiple infarcts to cortical regions. Frontotemporal dementia is due to the generation of the frontal and temporal lobe and present with personality and behavioral changes. Lewy body dementia is dementia and hallucination due to Lewy bodies located in the cortex.
Media
(Click Image to Enlarge)
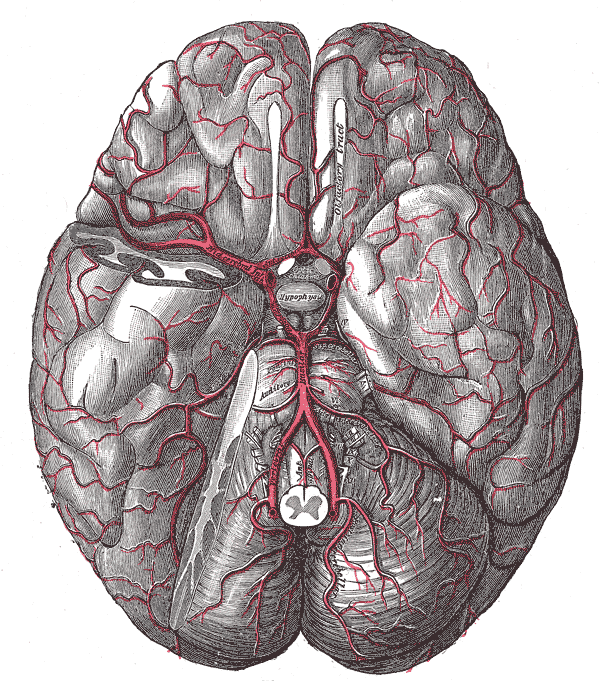
The arteries of the base of the brain
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
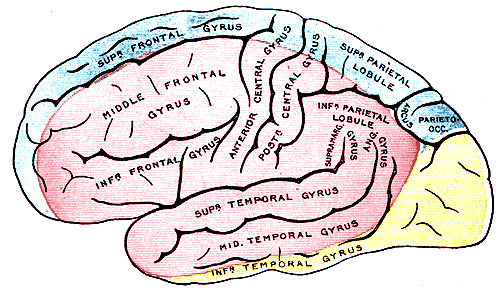
Outer Surface of the Cerebral Hemisphere. The outer surface of the cerebral hemisphere shows areas supplied by cerebral arteries. The blue areas are supplied by the anterior cerebral artery, the pink areas by the middle cerebral artery, and the yellow areas by the posterior cerebral artery.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
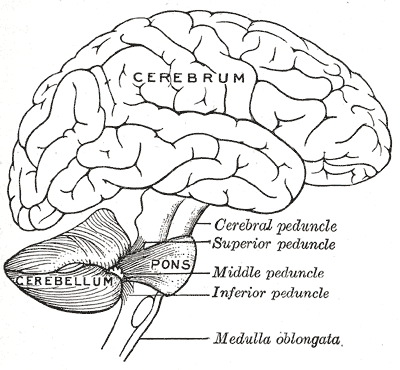
Brain, Encephalon, Connections of the several parts of the brain, Cerebrum, Cerebellum, Pons, Cerebral; Superior; Middle; Inferior Peduncle, Medulla oblongata
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
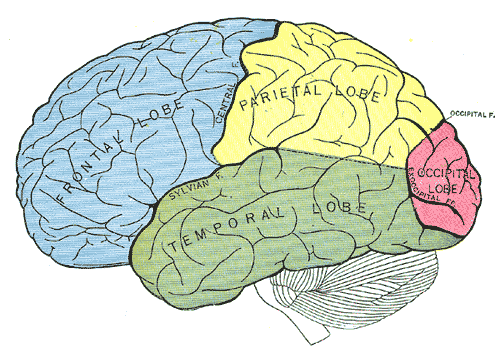
Principal fissures and lobes of the cerebrum viewed laterally, Frontal Lobe, Parietal Lobe, Temporal Lobe, Occipital Lobe
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
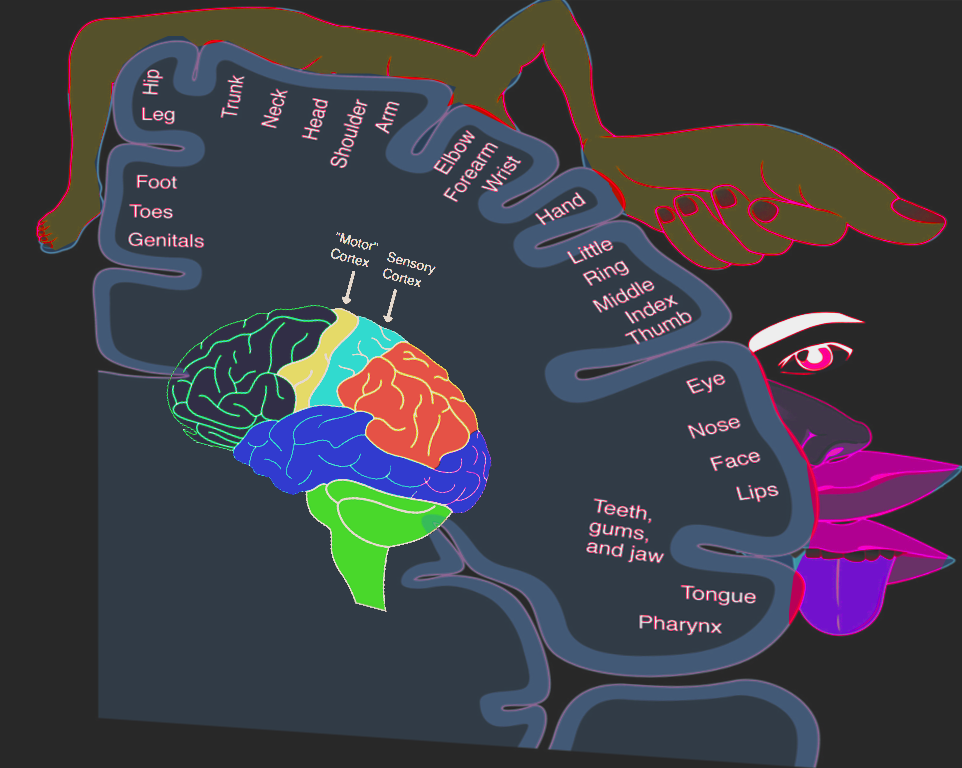
Homonculus: sensory & motor Image courtesy S. Bhimji MD
References
Stinnett TJ, Reddy V, Zabel MK. Neuroanatomy, Broca Area. StatPearls. 2023 Jan:(): [PubMed PMID: 30252352]
Altabakhi IW, Liang JW. Gerstmann Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 30137813]
Rehman A, Al Khalili Y. Neuroanatomy, Occipital Lobe. StatPearls. 2023 Jan:(): [PubMed PMID: 31335040]
Javed K, Reddy V, M Das J, Wroten M. Neuroanatomy, Wernicke Area. StatPearls. 2023 Jan:(): [PubMed PMID: 30422593]
Elshazzly M, Lopez MJ, Reddy V, Caban O. Embryology, Central Nervous System. StatPearls. 2023 Jan:(): [PubMed PMID: 30252280]
Konan LM, Reddy V, Mesfin FB. Neuroanatomy, Cerebral Blood Supply. StatPearls. 2023 Jan:(): [PubMed PMID: 30335330]
Avci E, Fossett D, Aslan M, Attar A, Egemen N. Branches of the anterior cerebral artery near the anterior communicating artery complex: an anatomic study and surgical perspective. Neurologia medico-chirurgica. 2003 Jul:43(7):329-33; discussion 333 [PubMed PMID: 12924591]
Level 3 (low-level) evidenceNavarro-Orozco D, Sánchez-Manso JC. Neuroanatomy, Middle Cerebral Artery. StatPearls. 2023 Jan:(): [PubMed PMID: 30252258]
Javed K, Reddy V, M Das J. Neuroanatomy, Posterior Cerebral Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 30860709]
Uddin MA, Haq TU, Rafique MZ. Cerebral venous system anatomy. JPMA. The Journal of the Pakistan Medical Association. 2006 Nov:56(11):516-9 [PubMed PMID: 17183980]
Kiliç T, Akakin A. Anatomy of cerebral veins and sinuses. Frontiers of neurology and neuroscience. 2008:23():4-15 [PubMed PMID: 18004050]
Dubourg C, Bendavid C, Pasquier L, Henry C, Odent S, David V. Holoprosencephaly. Orphanet journal of rare diseases. 2007 Feb 2:2():8 [PubMed PMID: 17274816]
Level 3 (low-level) evidenceGole RA, Meshram PM, Hattangdi SS. Anencephaly and its associated malformations. Journal of clinical and diagnostic research : JCDR. 2014 Sep:8(9):AC07-9. doi: 10.7860/JCDR/2014/10402.4885. Epub 2014 Sep 20 [PubMed PMID: 25386414]
Mochida GH. Genetics and biology of microcephaly and lissencephaly. Seminars in pediatric neurology. 2009 Sep:16(3):120-6. doi: 10.1016/j.spen.2009.07.001. Epub [PubMed PMID: 19778709]
Level 3 (low-level) evidence