Introduction
Colon polyps are protrusions occurring in the colon lumen most commonly sporadic or as part of other syndromes. Polyps are classified as diminutive if 5 mm in diameter or less, small if 6 to 9 mm, or large if they are 1 cm in diameter or more. Polyps can be depressed, flat, sessile or pedunculated. Few polyps arise from submucosa including lipomas, carcinoids or lymphoid aggregates. Most commonly, however, they result from the mucosa, and they can be adenomatous (tubular more than 80%, villous 5-15%, tubulovillous 5-15%), serrated (sessile or traditional), or non-neoplastic (hyperplastic and juvenile). Hyperplastic polyps are very common and have a very low malignant potential. They are encountered more in the distal colon. Juvenile polyps are benign hamartomas and are common in childhood. [1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Risk factors include advancing age, male gender, high-fat, low-fiber diet, tobacco use, and excess alcohol intake (more than eight drinks a week). Individuals with a family history of polyps, colorectal cancer, and intestinal polyposis carry a higher risk of developing colon polyps. Inflammatory bowel disease was found to be associated with decreased prevalence of polyps.[4]
Epidemiology
Colorectal polyps' incidence increases with age. They are more common in the western countries. With a prevalence of 30% in the people over the age 50 in the United States. However, 6% of children are affected, and the percentage goes up to 12% in children with lower gastrointestinal bleeding. Polyps are most prevalent in non-white men.[5][6]
Pathophysiology
The clinical significance of polyps arises from the fact that more than 95% of colon adenocarcinoma originate from polyps. Sessile serrated polyps are common, found more in the proximal colon, and have low malignant potential if there is no dysplasia, and significant malignant potential if they are dysplastic. Traditional serrated adenoma is uncommon, more often noted in the distal colon, with significant malignant potential. Non-neoplastic polyps include hyperplastic, juvenile polyps, hamartomas, and inflammatory pseudopolyps. Hyperplastic polyps are very common, found more in the distal colon, with very low malignant potential. Juvenile polyps are benign hamartomas and are not premalignant. They are common in childhood and more in the rectosigmoid. Polyps develop into cancer after inactivation of tumor suppressor genes as adenomatous polyposis coli (APC), or mismatch repair genes (MLH1). Genetics play a significant role; familial adenomatous polyposis (FAP) is autosomal dominant, and the majority of affected patients develop colorectal cancer (CRC) by age 40. Juvenile polyposis syndrome (JPS) is also autosomal dominant. Fifty to sixty percent of patients have a mutation in the SMAD4 or BMPR1A gene. By age 35, 20% of patients develop CRC. Other forms of inheritance exist as in MUTYH-associated polyposis (MAP) which is autosomal recessive caused by biallelic mutations in MUTYH gene.[7][8][9]
Histopathology
The three different polyps are villous, tubular and tubulovillous. Adenomatous polyps will gradually show dysplastic changes, which differentiates them from hyperplastic polyps. In general, colonic polyps are benign but those that develop high-grade dysplasia will become malignant with time.
History and Physical
Polyps are asymptomatic and usually found on screening colonoscopies for CRC. Patients may present with painless rectal bleeding of bright or dark red color, on wiping or with bowel movements mixed with stools or dripping. Other presentations include diarrhea, constipation, abdominal pain, mucus with stools, or with symptoms and signs of iron deficiency anemia secondary to chronic bleeding. A physical exam is usually normal, although rectal polyps may be palpated on digital rectal exam or if they are prolapsed. Fecal occult blood test (FOBT) by digital rectal exam (DRE) is not as effective as FOBT done on stool passed spontaneously.
Evaluation
Initial testing includes CBC to check for anemia found in chronic bleeding and BMP to check for electrolyte disorders as with hypersecretory adenomas. Guaiac (gFOBT) uses a chemical indicator with color change in the presence of blood and immunochemical (iFOBT or fecal immunochemical test []) uses antibodies against human hemoglobin. Stool DNA test is more sensitive but less specific than fecal immunochemical test (FIT).[10][11][12]
The gold standard test for polyps detection is colonoscopy, where polypectomy is done, and management is based on pathology results. This is however not a faultless screening test, as it has increased miss rate with low colon prep quality, smaller polyp, right-sided colon polyps, and less experience of the endoscopist. Patients found to have more than ten colorectal adenomas should be tested for MUTYH and APC. A newer way of screening is computed tomographic colonography (CTC) which requires excellent bowel preparation and is less sensitive with flat polyps. Other ways to diagnose are with double-contrast barium enemas and colon capsule endoscopies. Further research is still needed for enhanced optical technologies which may be used to differentiate between neoplastic and non-neoplastic colonic polyps, and they include narrowed spectrum endoscopy narrow-band imaging [NBI], confocal laser endomicroscopy [CLE], Fujinon intelligent chromoendoscopy [FICE] and image-enhanced endoscopy [i-scan].
Treatment / Management
Colonic polypectomy is done during colonoscopy for diagnostic and therapeutic purposes using snare polypectomy with electrocautery for pedunculated polyps, or mucosal resection for sessile polyps. Total colectomy with ileorectal anastomosis or proctocolectomy ileal pouch anal anastomosis is done for prophylactic reasons for Familial Adenomatous Polyposis (FAP) and MUTYH-associated polyposis (MAP). They may also be done with persistent bleeding or when there are too many polyps. Guidelines for CRC screening recommend a colonoscopy starting at age 50 for the general population, earlier for at-risk patients, and to stop screening if life expectancy is less than ten years. Risk factors for colon cancer include polyp pathology (adenomatous, serrated, with high-grade dysplasia, with more than 25% villous histology), polyp more than 1 cm in diameter, polyps located in the proximal colon and the number of polyps more than three. Hence, a follow-up colonoscopy is recommended to be done in 10 years if no polyps or distal small hyperplastic polyps are found; in five years if there are small sessile serrated polyps with no dysplasia; in three years if they are large sessile serrated polyp(s) or with dysplasia or traditional serrated adenoma. Other guidelines include screening in five to ten years if one or two small tubular adenomas are seen; in three years if there are three to ten adenomas; in less than three years if there are more than ten adenomas; and in three years if at least one adenoma is ten mm in diameter or more. Alternatively, also screen in three years if one or more adenomas show villous features of any or with high-grade dysplasia. Colectomy is recommended in cases of resected polyps with high-risk features of malignancy (lower third of the submucosa invasion, indeterminate or positive resection margins, margin less than 1 mm, lymphovascular invasion, or poor differentiation) as there is a high incidence of lymph node metastasis.[13][14](B2)
Differential Diagnosis
- Pseudopolyps
- Juvenile polyposis
- Hyperplastic polyposis
- Familial polyposis coli
- Turcot syndrome
- Cowden syndrome
- Peutz jegher syndrome
Complications
- Bleeding
- Diarrhea
- Bowel obstruction
- Cancer
Pearls and Other Issues
Recommendations that may decrease the incidence of colon polyps include low-fat, high fiber diet, decreased alcohol intake, and smoking cessation. No benefit was noted to decrease rates of CRC with the use of multivitamins, folate, calcium, statins, azathioprine or 6-mercaptopurine. Some studies found benefit using NSAID's and calcium in patients with FAP and MAP, where they may decrease the incidence and recurrence of polyps.
Enhancing Healthcare Team Outcomes
Because there is a potential risk of malignancy, all patients should be educated about polyps and follow up. Patients with a family history of polyps may benefit from screening colonoscopy. Those with hereditary nonpolyposis colon cancer should undergo screening colonoscopy every 1-2 years. In addition, these patients are also at risk for cancers in the ovary and uterus. [15][16](Level V)
Outcomes
When colonic polyps are removed, the condition is cured. If the polyp is not removed then it may cause bleeding, intussusception or even become malignant. However, colonic polyps grow slowly, and formation of a small polyp can take up to a decade. The risk of cancer is much higher in hereditary nonpolyposis cancer. The risk of cancer from a sporadic 1 cm colonic polyp is about 8% at ten years and 24% at 20 years. Ultimately the risk of malignancy also depends on the type of polyp, histology and if there is an association with polyposis syndromes. [17][18](Level V)
Media
(Click Image to Enlarge)
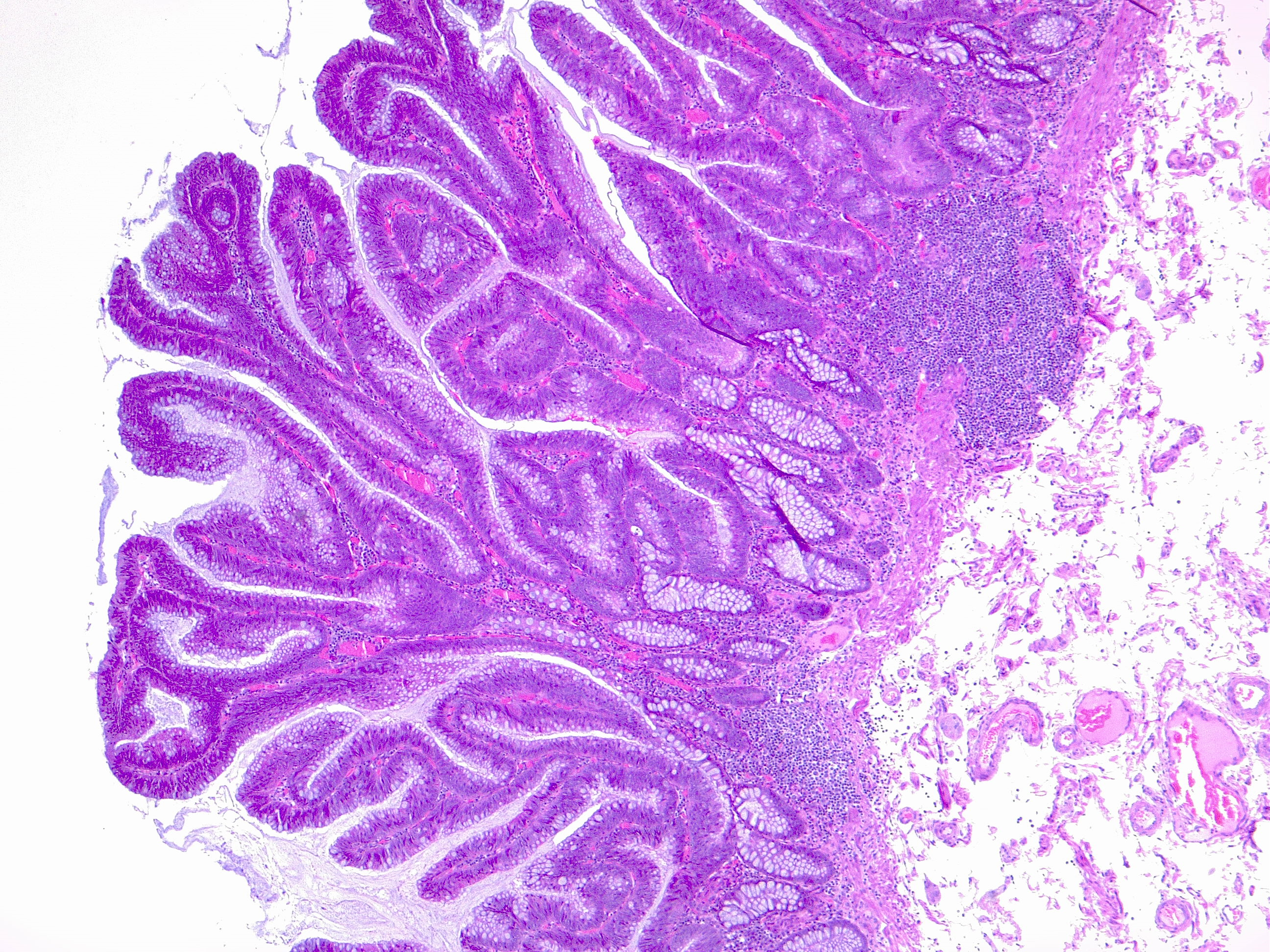
Colon polyp. Villous adenoma, low grade atypia. H/E 4x Contributed by Fabiola Farci, MD
(Click Image to Enlarge)
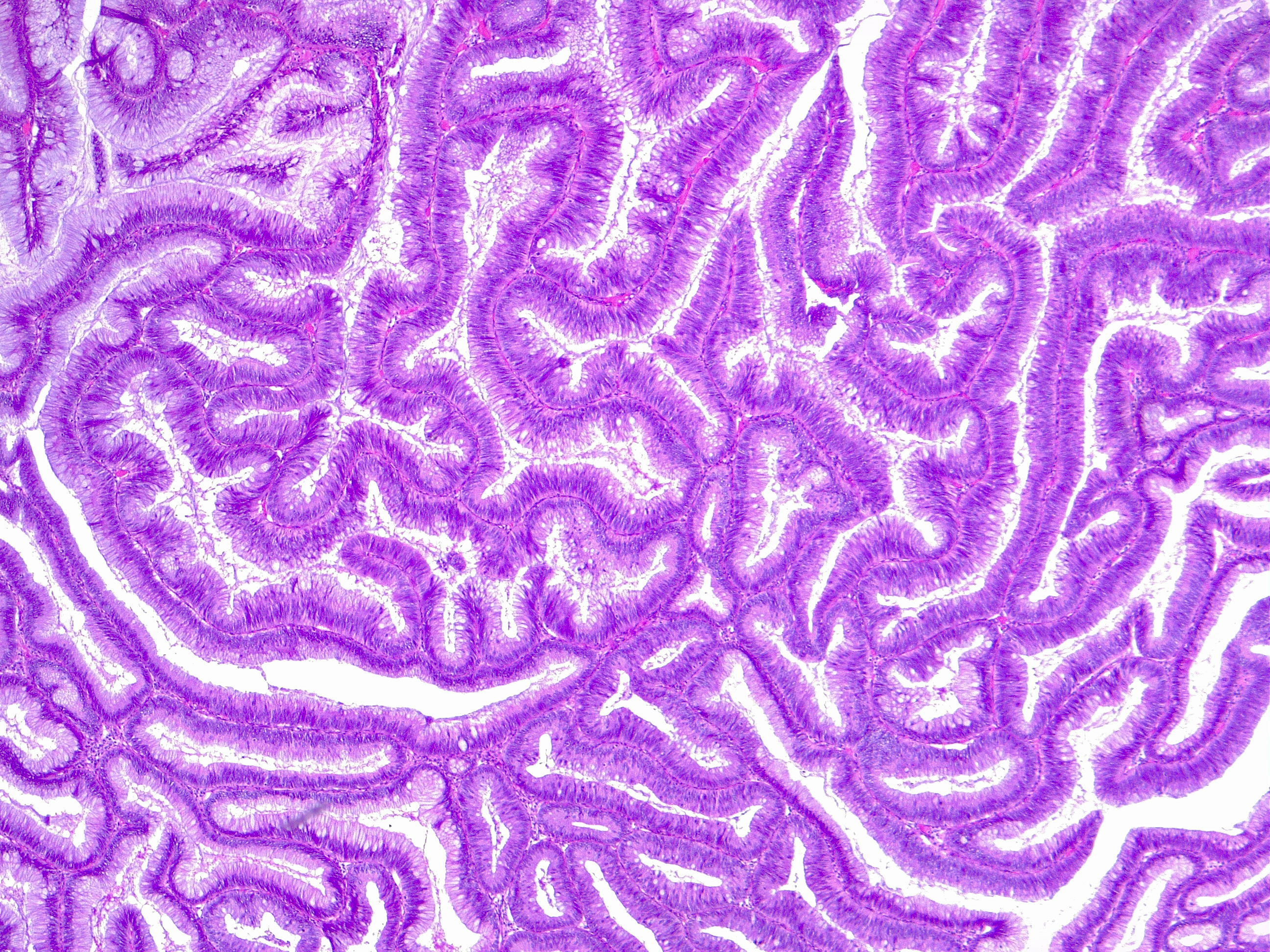
Villous adenoma. Typical complex architecture of mucinous glands, as depicted in this villous colon adenoma. Contributed by Fabiola Farci, MD
(Click Image to Enlarge)
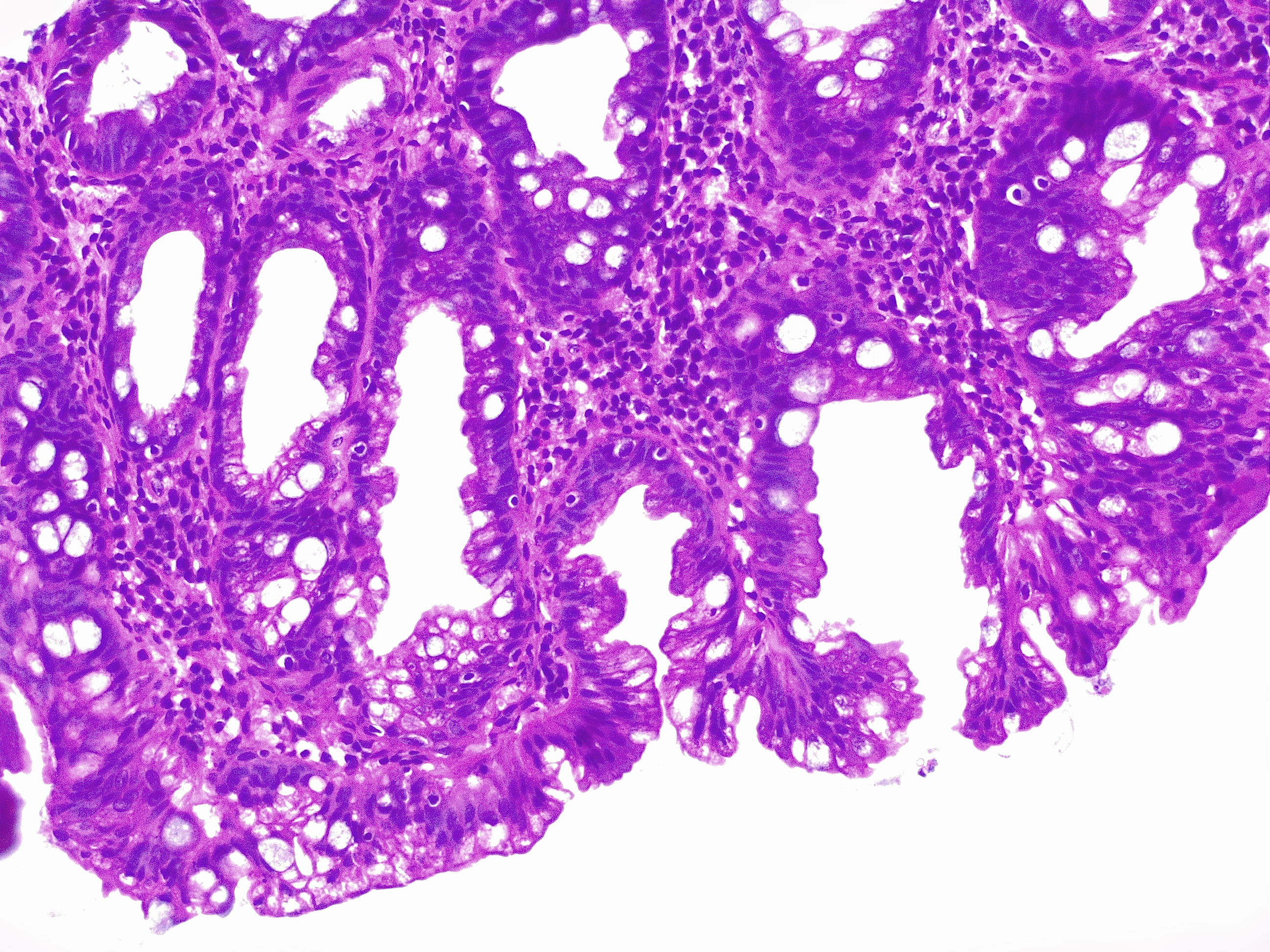
Colon biopsy, polypectomy following a screening colonoscopy. Hyperplastic glands. Contributed by Fabiola Farci, MD
(Click Image to Enlarge)
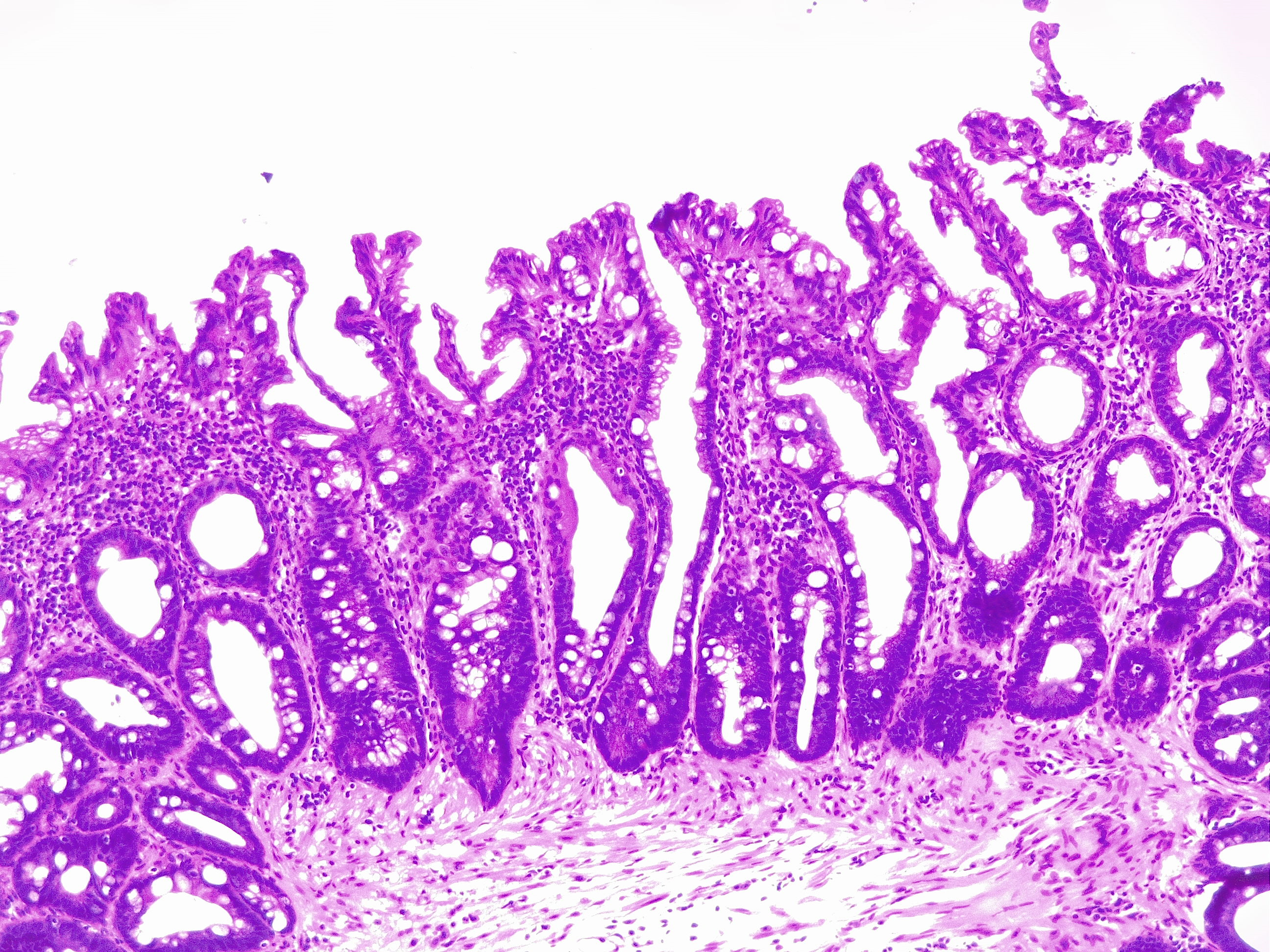
Hyperplastic polyp of the colon. The glands are of "U" shape, the mucin production and maturation is altered in the crypts, resulting in a lightly effaced architecture. There is serration in the upper third. This is a colon polyp without adenomatous features. Contributed by Fabiola Farci, MD
(Click Image to Enlarge)
Colonic polyps Contributed by Sunil Munakomi, MD
References
Chen EY, Vaccaro GM. Small Bowel Adenocarcinoma. Clinics in colon and rectal surgery. 2018 Sep:31(5):267-277. doi: 10.1055/s-0038-1660482. Epub 2018 Sep 4 [PubMed PMID: 30186048]
Hsieh YH, Leung FW. Increase your adenoma detection rate without using fancy adjunct tools. Ci ji yi xue za zhi = Tzu-chi medical journal. 2018 Jul-Sep:30(3):127-134. doi: 10.4103/tcmj.tcmj_86_18. Epub [PubMed PMID: 30069119]
Turner JS, Henry D, Chase A, Kpodzo D, Flood MC, Clark CE. Adenoma Detection Rate in Colonoscopy: Does the Participation of a Resident Matter? The American surgeon. 2018 Jun 1:84(6):1064-1068 [PubMed PMID: 29981650]
Yoshizawa N, Yamaguchi H, Kaminishi M. Differential diagnosis of solitary gastric Peutz-Jeghers-type polyp with stomach cancer: a case report. International journal of surgery case reports. 2018:51():261-264. doi: 10.1016/j.ijscr.2018.09.005. Epub 2018 Sep 10 [PubMed PMID: 30219660]
Level 3 (low-level) evidenceClick B, Pinsky PF, Hickey T, Doroudi M, Schoen RE. Association of Colonoscopy Adenoma Findings With Long-term Colorectal Cancer Incidence. JAMA. 2018 May 15:319(19):2021-2031. doi: 10.1001/jama.2018.5809. Epub [PubMed PMID: 29800214]
Mouchli MA, Ouk L, Scheitel MR, Chaudhry AP, Felmlee-Devine D, Grill DE, Rashtak S, Wang P, Wang J, Chaudhry R, Smyrk TC, Oberg AL, Druliner BR, Boardman LA. Colonoscopy surveillance for high risk polyps does not always prevent colorectal cancer. World journal of gastroenterology. 2018 Feb 28:24(8):905-916. doi: 10.3748/wjg.v24.i8.905. Epub [PubMed PMID: 29491684]
Dabbous HK,Mohamed YAE,El-Folly RF,El-Talkawy MD,Seddik HE,Johar D,Sarhan MA, Evaluation of Fecal M2PK as a Diagnostic Marker in Colorectal Cancer. Journal of gastrointestinal cancer. 2018 Apr 7 [PubMed PMID: 29626277]
Raab M, Sanhaji M, Matthess Y, Hörlin A, Lorenz I, Dötsch C, Habbe N, Waidmann O, Kurunci-Csacsko E, Firestein R, Becker S, Strebhardt K. PLK1 has tumor-suppressive potential in APC-truncated colon cancer cells. Nature communications. 2018 Mar 16:9(1):1106. doi: 10.1038/s41467-018-03494-4. Epub 2018 Mar 16 [PubMed PMID: 29549256]
Castro J, Cuatrecasas M, Balaguer F, Ricart E, Pellisé M. Serrated polyposis syndrome associated with long-standing inflammatory bowel disease. Revista espanola de enfermedades digestivas. 2017 Nov:109(11):796-798. doi: 10.17235/reed.2017.5068/2017. Epub [PubMed PMID: 29027468]
Hakimian S, Jawaid S, Guilarte-Walker Y, Mathew J, Cave D. Video capsule endoscopy as a tool for evaluation of obscure overt gastrointestinal bleeding in the intensive care unit. Endoscopy international open. 2018 Aug:6(8):E989-E993. doi: 10.1055/a-0590-3940. Epub 2018 Aug 3 [PubMed PMID: 30083589]
Iwai T, Imai K, Hotta K, Ito S, Yamaguchi Y, Kawata N, Tanaka M, Kakushima N, Takizawa K, Ishiwatari H, Matsubayashi H, Ono H. Endoscopic prediction of advanced histology in diminutive and small colorectal polyps. Journal of gastroenterology and hepatology. 2019 Feb:34(2):397-403. doi: 10.1111/jgh.14409. Epub 2018 Aug 16 [PubMed PMID: 30070395]
Aihara H, Kumar N, Thompson CC. A Web-Based Education Program for Colorectal Lesion Diagnosis with Narrow Band Imaging Classification. Digestion. 2018:98(1):11-18. doi: 10.1159/000486481. Epub 2018 Apr 19 [PubMed PMID: 29672309]
Jover R, Dekker E, Schoen RE, Hassan C, Pellise M, Ladabaum U, WEO Expert Working Group of Surveillance after colonic neoplasm. Colonoscopy quality requisites for selecting surveillance intervals: A World Endoscopy Organization Delphi Recommendation. Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society. 2018 Nov:30(6):750-759. doi: 10.1111/den.13229. Epub 2018 Jul 26 [PubMed PMID: 29971834]
Level 2 (mid-level) evidenceKang H, Thoufeeq MH. Size of colorectal polyps determines time taken to remove them endoscopically. Endoscopy international open. 2018 May:6(5):E610-E615. doi: 10.1055/a-0587-4681. Epub 2018 May 8 [PubMed PMID: 29756019]
Gibson DJ, Nolan B, Rea J, Buckley M, Horgan G, Sheahan K, Doherty GA, O'Donoghue D, Mulcahy HE, Smith A, Cullen G. A prospective study of faecal immunochemical testing following polypectomy in a colorectal cancer screening population. Frontline gastroenterology. 2018 Oct:9(4):295-299. doi: 10.1136/flgastro-2017-100869. Epub 2017 Nov 4 [PubMed PMID: 30245792]
Arana-Arri E, Imaz-Ayo N, Fernández MJ, Idigoras I, Bilbao I, Bujanda L, Bao F, Ojembarrena E, Gil I, Gutiérrez-Ibarluzea I, Portillo I. Screening colonoscopy and risk of adverse events among individuals undergoing fecal immunochemical testing in a population-based program: A nested case-control study. United European gastroenterology journal. 2018 Jun:6(5):755-764. doi: 10.1177/2050640618756105. Epub 2018 Jan 24 [PubMed PMID: 30083338]
Level 2 (mid-level) evidenceKawamura T, Sakai H, Ogawa T, Sakiyama N, Ueda Y, Shirakawa A, Okada Y, Sanada K, Nakase K, Mandai K, Suzuki A, Morita A, Tanaka K, Uno K, Yasuda K. Feasibility of Underwater Endoscopic Mucosal Resection for Colorectal Lesions: A Single Center Study in Japan. Gastroenterology research. 2018 Aug:11(4):274-279. doi: 10.14740/gr1021w. Epub 2018 Feb 8 [PubMed PMID: 30116426]
Level 2 (mid-level) evidenceObaro AE, Burling DN, Plumb AA. Colon cancer screening with CT colonography: logistics, cost-effectiveness, efficiency and progress. The British journal of radiology. 2018 Oct:91(1090):20180307. doi: 10.1259/bjr.20180307. Epub 2018 Jul 5 [PubMed PMID: 29927637]