Introduction
The cranial nerves provide afferent and efferent innervation principally to the head and neck structures. Unlike spinal nerves, whose roots are neural fibers from the spinal grey matter, cranial nerves are composed of the neural processes associated with distinct brainstem nuclei and cortical structures. Unlike the spinal nerves, cranial nerve nuclei are functionally organized into distinct nuclei within the brainstem. Typically, the more posterior and lateral nuclei tend to be sensory, and the more anterior tend to be motor. Cranial nerves I (olfactory), II (optic), and VIII (vestibulocochlear) are considered purely afferent. Cranial nerves III (oculomotor), IV (trochlear), VI (abducens), XI (spinal accessory), and XII (hypoglossal) are purely efferent. The remaining cranial nerves, V (trigeminal), VII (facial), IX (glossopharyngeal), and X (vagus), are functionally mixed (sensory and motor).[1] See Image. Cranial Nerves.
While this is the classical way of organizing and indexing cranial nerves, the scientific reality is more complex. It is still debated in the academic realm, including the classification and identification of the routes of distinct cranial nerve fibers and the presence or absence of other less recognized structures, such as the terminal nerve, also called nerve nulla or cranial nerve zero. The latter could be classified as a pure afferent nerve following the traditional organization of cranial nerves—damage to the cranial nerves, their tracts, or nuclei results in stereotyped clinical syndromes.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The cranial nerves can be considered in terms of their anatomical numbering from I to XII, which describes their sequential origins from the caudal to the ventral brainstem, or in groups according to their developmental functions (ie, sensory, motor, mixed). Here, we broadly detail the 12 cranial nerves in their anatomical ordering before briefly outlining their functional groupings. See Image. Human Brain Cranial Nerves.
Cranial nerve I (olfactory nerve)
Special visceral afferent bipolar sensory neurons reside in the olfactory mucosa, an area of approximately 2 to 4 cm2 over the superior nasal concha and nasal septum). Here, they are organized into nerve bundles called filia olfactoria, which comprise the olfactory nerve. They enter the cranium through the cribriform plate of the ethmoid bone to synapse in the olfactory bulb, which forms the anterior-most aspect of the olfactory tract at the inferior aspect of the frontal lobe, and which extends posteriorly between the orbital gyrus and the gyrus rectus until bifurcating at the olfactory trigone as the medial and lateral olfactory stria which terminate in higher-order cortex.[2] Some olfactory projections travel medially to the septal area and the contralateral bulb via the anterior commissure. In contrast, other fibers travel laterally to the amygdala and piriform cortex, also known as the primary olfactory cortex, where conscious odorant sense is processed.[3]
Cranial nerve II (optic nerve)
Cranial nerve II, the optic nerve, conveys special somatic afferent visual sensory information from the rods and cones of retinal sensory receptors to the thalamus, especially the lateral geniculate nucleus (LGN) and the superior colliculus (SC). Ganglion cells, whose cell bodies are located deep in the retina, have central projections that form the optic nerve fibers, which traverse the optic canal to enter the cranium. From there, fibers representing the medial visual fields travel posteriorly without crossing at the optic chiasm, while fibers of the lateral visual fields cross within the chiasm. Therefore, regions of the visual field are retinotopically organized within the optic nerve and at their synapses in the LGN. Collaterals are also given off centrally to innervate the SC, which is responsible for the pupillary light reflex and connections within the pulvinar of the thalamus, providing unconscious optic input responsible for the phenomenon of blindsight.[4] In cortically blind individuals, these pulvinar collaterals from the optic nerve allow for unconscious eye movements in response to the detection of light and a weak directional sense of the location of the light within the visual field.[5][6][7]
Cranial nerves III, IV, and VI (oculomotor, trochlear, and abducens nerve)
Cranial nerves III, IV, and VI (oculomotor, trochlear, and abducens nerves, respectively) are general somatic efferent (GSE) nerves responsible for innervating the extraocular muscles within the orbit (see Image. Orbit, Anterior View). These nerves travel ipsilaterally from the brainstem to the calvarium through the superior orbital fissure from synonymous brainstem nuclei. The oculomotor nerve (CN III) travels through the common tendinous ring, the common attachment in the posterior orbit for the 4 extraocular recti muscles, and the abducens nerve (cranial nerve VI). The trochlear nerve (CN IV) travels into the orbit outside the common tendinous ring to innervate the superior oblique muscle of the eye. The abducens nerve innervates the lateral rectus muscles only; thereby, this nerve can be tested by evaluating the abduction of the eye gaze.
Cranial nerve III innervates most of the eye muscles by splitting into a superior and an inferior branch to innervate the remaining 3 recti muscles, the inferior oblique, and the skeletal muscle component of the levator palpebrae superioris. However, cranial nerve III also has a general visceral efferent (GVE) component originating in the Edinger-Westphal nucleus (also called accessory or visceral oculomotor). These fibers travel with cranial nerve III to synapse in the ciliary ganglion within the orbit. The post-ganglionic sympathetic fibers of the ciliary ganglion pierce the eye's sclera to innervate the pupillary sphincter and ciliary smooth muscles responsible for pupillary constriction and lens accommodation. Pupillary constriction can be tested using the pupillary light reflex through the efferents from the superior colliculus to the accessory oculomotor nucleus.[8]
The eye movements test (abduction, adduction, infraduction, supraduction) effectively assesses the viability of the GSE components of cranial nerves III, IV, and VI.
Cranial nerve V (trigeminal nerve)
Cranial Nerve V is the trigeminal nerve responsible for the face's general somatic sensory innervation (GSA) through its 3 main branches, V1, V2, and V3 (ophthalmic, maxillary, and mandibular). This cranial nerve (via V3) is also responsible for motor innervation (SVE) of the muscles of mastication, the anterior belly of the digastric, mylohyoid, and 2 tiny tensor muscles: the tensor veli palatini and tensor tympani. While no autonomic fibers travel with the fifth cranial nerve as it exits the pons, parasympathetic fibers from the other mixed cranial nerves join with peripheral branches of cranial nerve V to innervate their respective target structures, such as the lacrimal, parotid, submandibular and sublingual glands. In this sense, central nuclear or supranuclear lesions may result in ipsilateral sensory or motor deficits. Still, peripheral nerve damage to the respective branches only impairs parasympathetic functions.[9]
Cranial nerve VII (facial nerve)
Cranial nerve VII (facial nerve) has motor and autonomic fibers with minor somatosensory components. Special visceral efferent (SVE) motor innervation is to the muscles of facial expression and exits the skull through the stylomastoid foramen deep to the parotid gland. Damage to these fibers results in ipsilateral facial paralysis (facial palsy). General visceral efferents (GVE) and special visceral afferents (SVA) fibers initially exit the brainstem as nervus intermedius. This separate nerve bundle joins with the other components of the facial nerve within the facial canal. The GVE components from the superior salivary nucleus are responsible for parasympathetic innervation of the glands and mucosae of the face, except for the parotid gland and the smaller buccal and labial glands. Taste fibers from the anterior two-thirds of the tongue travel centrally as the chorda tympani nerve to their cell body origin in the geniculate ganglion before synapsing centrally in the solitary nucleus. Depending on the location of the lesion, these visceral components may also be impacted in lesions of the facial nerve. Somatic afferents (GSA) provide sensory innervation from the auricle and a small external portion of the auditory canal.[10]
Cranial nerve VIII (vestibulocochlear nerve)
Cranial nerve VIII, the vestibulocochlear nerve, is responsible for the auditory and vestibular sense of orientation of the head. This nerve conveys special sensory afferents (SSA) from the inner ear to the cochlear nuclei and the vestibular nuclei in the caudal medulla oblongata. Hair cells within the cochlear duct, semi-circular canals, utricle, and saccule are polarized sensory receptor cells with apical ciliary extensions that transduce an electrochemical signal upon mechanical deformation. Ganglionic neurons within the cochlea and the vestibular nerve receive this signal peripherally and transmit it centrally through the internal auditory meatus before entering the medulla.[11]
Cranial nerve IX (glossopharyngeal nerve)
Cranial nerve IX (glossopharyngeal nerve) is responsible for motor (SVE) innervation of the stylopharyngeus and the pharyngeal constrictor muscles by the nucleus ambiguus. Inferior salivary nucleus fibers travel with cranial nerve IX to provide general visceral efferent (GVE) innervation to parotid, buccal, and labial glands. In contrast, visceral afferents (GVA and SVA) receive sensory information from the carotid body and carotid sinus and taste from the posterior third of the tongue to synapse on the solitary nucleus. The sensory afferents (GSA) receive information from the skin over the tongue, oropharynx, middle ear cavity, and auditory canal.[12]
Cranial nerve X (vagus nerve)
Cranial nerve X is the vagus nerve. The parasympathetic efferents (GVE) fibers from the dorsal vagal nucleus to the thoracic and abdominal viscera to the splenic flexure of the colon represent its major neural component. These fibers form a comprehensive plexus that travels along the esophageal serosa to the viscera. It also has a considerable motor output (SVE) from the nucleus ambiguous to the pharyngeal and soft palate muscles and the intrinsic laryngeal muscles via the superior and recurrent laryngeal nerves. Somatic afferents (GSA) supply the posterior cranial dura and a portion of the ear and external auditory canal epithelium. Visceral afferents (GVA) from the pharynx, larynx, aorta, thoracic and abdominal viscera, and taste buds from the root of the tongue and epiglottis (SVA) synapse on the solitary nucleus as well. Damage to the recurrent laryngeal branch of the vagus nerve can result in vocal hoarseness or acute dyspnea with bilateral avulsion.
Cranial nerve XI (Accessory nerve)
Cranial nerve XI, the spinal accessory nerve, is responsible for the general somatic efferent (GSE) motor innervation of the trapezius and sternocleidomastoid muscles by way of the spinal nucleus of the accessory nerve. The spinal nucleus of the accessory nerve is located within the cervical spinal cord from the levels of C1 through approximately C5/6. The fibers emerge as independent roots, separate from the anterior or dorsal spinal roots of the central spinal grey matter, and ascend through the foramen magnum to enter the cranial cavity. These fibers exit via the jugular foramen and cranial nerves IX and X.
Cranial nerve XII (Hypoglossal nerve)
Cranial nerve XII, the hypoglossal nerve, is responsible for the general somatic efferent (GSE) innervation of the intrinsic and extrinsic muscles of the tongue, except the palatoglossus muscle, from the nerve’s synonymous nucleus. This includes the genioglossus, geniohyoid, hyoglossus, and styloglossus muscles. Fibers from the hypoglossal nucleus exit the medulla from the sulcus between the pyramids and the olives as a collection of fibers that coalesce before entering the hypoglossal canal to exit the cranium.[13]
The cranial nerves can also be grouped according to their functional roles: efferent nerves (motor output), efferent nerves (sensory input), or mixed nerves. Cranial nerves I, II, and VIII are considered purely afferent nerves since they conduct sensory information from the olfactory region, the retina of the eye, and the inner ear structures, respectively. Cranial nerves III, IV, VI, XI, and XII are considered purely efferent due to their motor output to the orbit, the neck, and the tongue. Cranial nerves V, VII, IX, and X are considered mixed cranial nerves due to afferent and efferent fibers with sensory and motor components.
Clinical Significance
CN I
Traumatic injury, especially “whiplash” from automobile collisions, can sever the olfactory projections through the cribriform plate, resulting in anosmia, which has been associated with the development of depression.[14][15][16] The sense of olfaction also appears to have a nonconscious role in activating the limbic system, which may account for such an effect.[17]
CV VIII
Damage to the vestibular component of this nerve causes dizziness, while damage to the cochlear part causes peripheral or sensorineural hearing loss. The internal auditory meatus is a narrow canal of the temporal bone through which these nerves course. The schwannoma of this meatus's vestibular or cochlear nerves easily compresses and impinges these nerves. Early signs and symptoms are progressively worsening hearing loss with tinnitus and imbalance, leading to a sense of pressure in the ear and facial weakness or paralysis.[18] Vestibular schwannomas have an incidence rate of 6 to 9 new cases per year per million people and are readily treatable with surgery or radiation.[19] However, if the condition is left untreated, it can result in potentially significant and life-threatening tumors.
CN XI
Central root or nuclear damage to the spinal accessory nerve results in ipsilateral flaccid paralysis of the sternocleidomastoid (with difficulty turning the head against force) and partial ipsilateral trapezius paralysis leading to shoulder drop. The trapezius is innervated by anterior horn grey matter from cervical spinal regions C3 through C4/5 in addition to the spinal accessory nerve. Thus, complete paralysis of the trapezius muscle does not occur following a simple focal lesion.[20]
CN XII
Damage to the nucleus or nerve fibers results in tongue deviation toward the side of the lesion, as the ipsilateral genioglossus muscle becomes weak or flaccid, reducing its ability to protrude the tongue.
Other Issues
In addition, the terminal or cranial nerve zero has been identified as a separate cranial nerve in the human brain dating back to 1914. Still, it is overlooked by most current anatomical textbooks.[21] Also called nervus terminalis (for its proximity to the lamina terminalis) or the nerve nulla (ie, nothing, zero), cranial nerve zero is comprised of an independent central plexus of small unmyelinated (possibly special visceral afferent [SVA]) fibers located medially and in very close proximity to the olfactory tract by the olfactory trigone. Its discrete positioning may explain its poor identification during standard dissection techniques. The cranial nerve zero fibers travel centrally to subcortical structures; it sends projections to the medial pre-commissural septum and the medial septal nucleus, among others. It appears to have a rich bundle of well-vascularized fibers ascending from the nasal submucosa and projecting to important limbic structures (eg, amygdala, hypothalamic nuclei).
Functionally, it has been regarded as pheromones processing unconsciously by regulating autonomic responses through hypothalamic gonadotropin-releasing hormone (GnRH), possibly via the kisspeptin neuronal network. Clinically, a disruption of the normal embryological migratory pathway of GnRH neural crest cells of the olfactory placode and basal forebrain can result in Kallman syndrome, a genetic condition characterized by hypogonadotropic hypogonadism with partial or total anosmia, also resulting in abnormal sexual development in both sexes.[22]
The canonical descriptions of the cranial nerves serve as an overview of the current medical literature. Still, research advances continuously reveal new information, leading to riveting debates regarding the original classification of some cranial nerve fibers. For instance, it has been found that the nervus intermedius, known for carrying taste fibers from the tongue and associated with cranial nerve VII, has visceral efferent connections with the vestibulocochlear nerve in the internal auditory meatus.[23] Indeed, varied populations of efferent fibers to the organ of Corti hair cells modulate afferent transduction sensitivity and are present in mammals and vertebrates.[24][25][26][27][25]
Also, the classification of the cranial accessory nerve as a portion of either vagus or accessory nerves is continually disputed. In most cases, the cranial accessory nerve, with its fibers originating in the nucleus ambiguus of the medulla, has no connections with the spinal accessory nerve and its fibers originating in the spinal accessory nucleus of the spinal cord.[28] Also, cranial nerve zero has been recognized in human embryos since 1905 and in adult humans since 1914. While historical textbooks included this nerve, modern anatomical textbooks have omitted it from the official list of cranial nerves.[29][30] However, the sensory function and modulation of the hypothalamic endocrine and autonomic systems make it physiologically and clinically relevant.[21] Similarly, it has been argued that the optic nerve (cranial nerve II) is not a peripheral nerve but a central cranial tract.[29] This is evidence of the continuous changes brought to accepted anatomical and medical terminology and the structures reflected by those terms.[31][32] As such, a holistic view of cranial nerves may be more valuable than the categorical organization in most textbook narratives. These issues warrant attention since all cranial nerve nuances are particularly relevant for medical and health professions education.
Media
(Click Image to Enlarge)
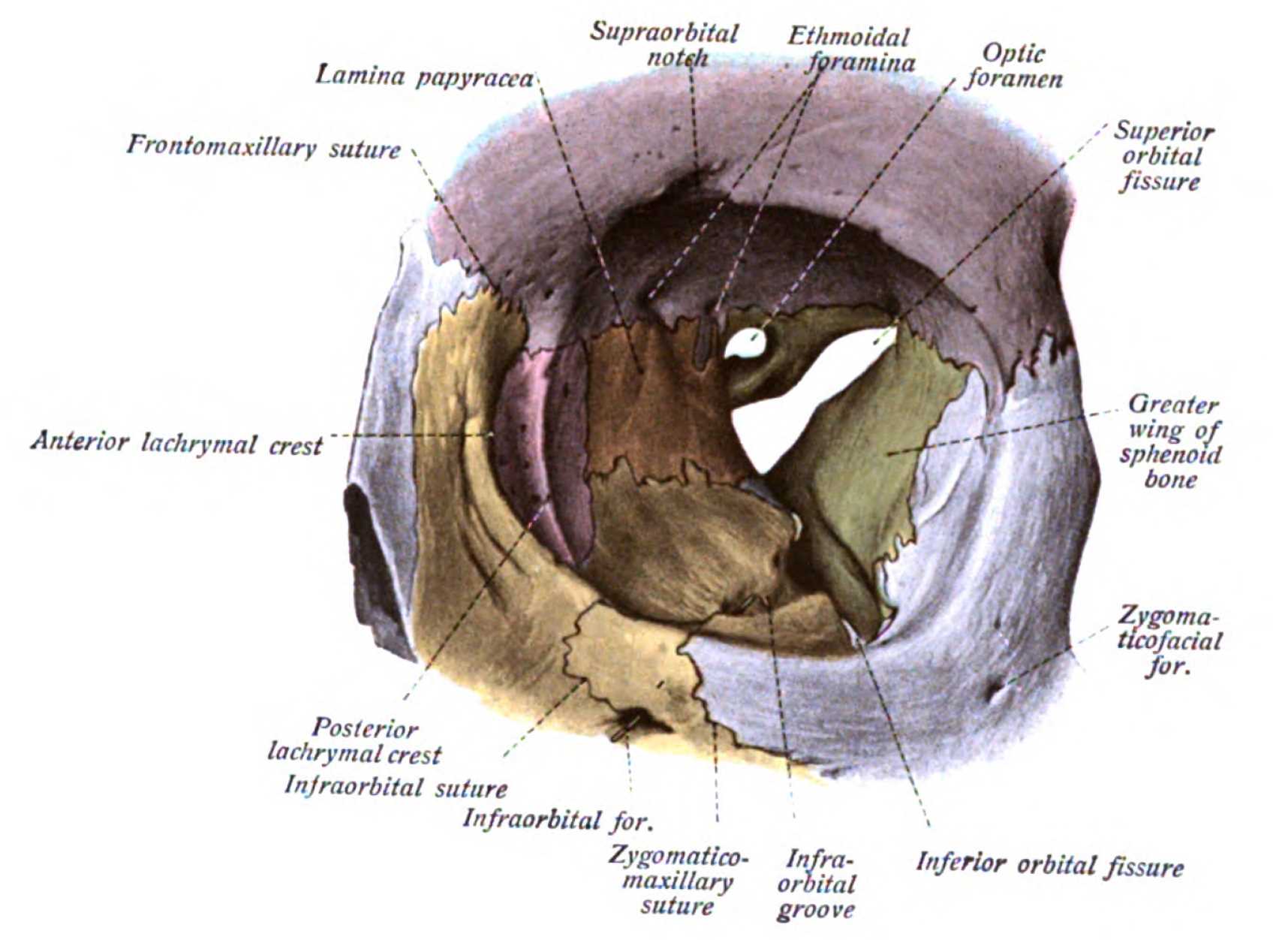
Orbit, Anterior View. Shown in this illustration are the supraorbital notch, ethmoidal foramina, optic foramen, superior orbital fissure (hourglass configuration), greater wing of the sphenoid bone, zygomaticofacial foramen, inferior orbital fissure, infraorbital groove, zygomaticomaxillary suture, infraorbital foramen, infraorbital suture, posterior lacrimal crest, anterior lacrimal crest, frontomaxillary suture, and lamina papyracea. The walls of the orbit include the frontal bone superiorly; ethmoid, frontal, lacrimal, and sphenoid bones medially; maxilla, zygomatic, and palatine bones inferiorly; and zygomatic and sphenoid bones laterally.
Dr. Johannes Sobotta, Public Domain, Wikimedia Commons
(Click Image to Enlarge)
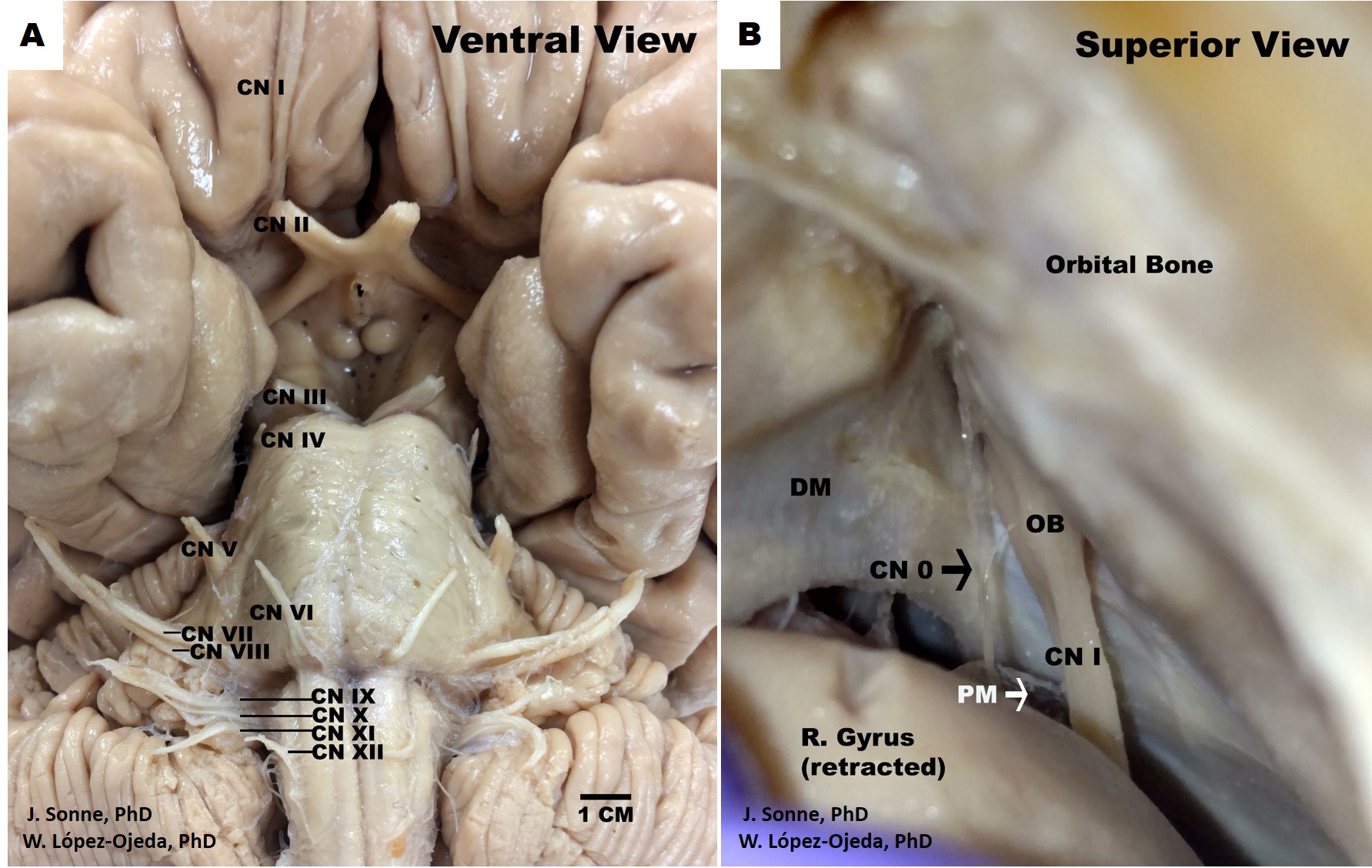
Human Brain Cranial Nerves. Ventral view of the human brain depicting the canonical organization of the 12 pairs of cranial nerves (CN) as described in the classical medical nomenclature (A). Roman numerals (I-XII) are used in progressive order to identify the rostrocaudal organization of the 12 pairs of cranial nerves, (B). Superior view of the human skull and frontal brain lobe following a special dissection procedure to reveal the intact cranial nerve zero (CN 0) (black arrow). DM= dura matter, OB= olfactory bulb, PM= pia matter.
Contributed by J Sonne, PhD, and W López-Ojeda, PhD
(Click Image to Enlarge)
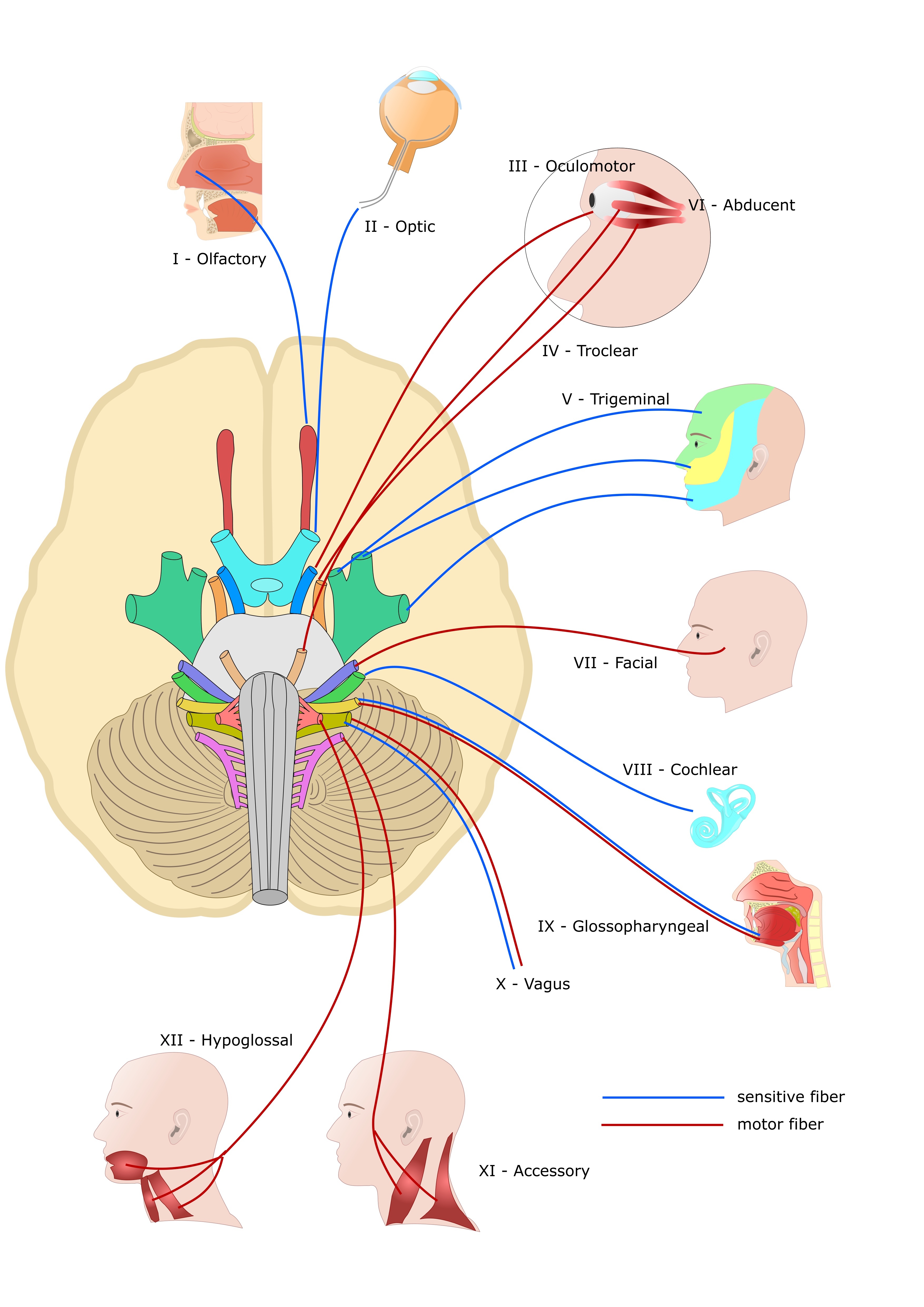
Cranial Nerves. This illustration shows the anatomic relationships between cranial nerves I to XII and some of the organs they supply.
Shutterstock
References
Traylor KS, Branstetter BF 4th. Cranial Nerve Anatomy. Neuroimaging clinics of North America. 2022 Aug:32(3):565-576. doi: 10.1016/j.nic.2022.04.004. Epub [PubMed PMID: 35843663]
López-Elizalde R, Campero A, Sánchez-Delgadillo T, Lemus-Rodríguez Y, López-González MI, Godínez-Rubí M. Anatomy of the olfactory nerve: A comprehensive review with cadaveric dissection. Clinical anatomy (New York, N.Y.). 2018 Jan:31(1):109-117. doi: 10.1002/ca.23003. Epub 2017 Nov 10 [PubMed PMID: 29088516]
Milardi D, Cacciola A, Calamuneri A, Ghilardi MF, Caminiti F, Cascio F, Andronaco V, Anastasi G, Mormina E, Arrigo A, Bruschetta D, Quartarone A. The Olfactory System Revealed: Non-Invasive Mapping by using Constrained Spherical Deconvolution Tractography in Healthy Humans. Frontiers in neuroanatomy. 2017:11():32. doi: 10.3389/fnana.2017.00032. Epub 2017 Apr 10 [PubMed PMID: 28443000]
Direct optic nerve pulvinar connections defined by diffusion MR tractography in humans: implications for photophobia., Maleki N,Becerra L,Upadhyay J,Burstein R,Borsook D,, Human brain mapping, 2012 Jan [PubMed PMID: 21337474]
Zihl J, von Cramon D. Registration of light stimuli in the cortically blind hemifield and its effect on localization. Behavioural brain research. 1980 Aug:1(4):287-98 [PubMed PMID: 7295378]
Ffytche DH, Zeki S. The primary visual cortex, and feedback to it, are not necessary for conscious vision. Brain : a journal of neurology. 2011 Jan:134(Pt 1):247-57. doi: 10.1093/brain/awq305. Epub 2010 Nov 19 [PubMed PMID: 21097490]
Cowey A. Visual system: how does blindsight arise? Current biology : CB. 2010 Sep 14:20(17):R702-4. doi: 10.1016/j.cub.2010.07.014. Epub [PubMed PMID: 20833309]
Level 3 (low-level) evidenceDifferences in pupillary light reflex between optic neuritis and ischemic optic neuropathy., Yoo YJ,Hwang JM,Yang HK,, PloS one, 2017 [PubMed PMID: 29049405]
Patel NM, Jozsa F, Das JM. Neuroanatomy, Spinal Trigeminal Nucleus. StatPearls. 2024 Jan:(): [PubMed PMID: 30969551]
Myckatyn TM, Mackinnon SE. A review of facial nerve anatomy. Seminars in plastic surgery. 2004 Feb:18(1):5-12. doi: 10.1055/s-2004-823118. Epub [PubMed PMID: 20574465]
Benoudiba F, Toulgoat F, Sarrazin JL. The vestibulocochlear nerve (VIII). Diagnostic and interventional imaging. 2013 Oct:94(10):1043-50. doi: 10.1016/j.diii.2013.08.015. Epub 2013 Oct 1 [PubMed PMID: 24095603]
Thomas K, Minutello K, Das JM. Neuroanatomy, Cranial Nerve 9 (Glossopharyngeal). StatPearls. 2024 Jan:(): [PubMed PMID: 30969699]
Loh C, Maya MM, Go JL. Cranial nerve XII: the hypoglossal nerve. Seminars in ultrasound, CT, and MR. 2002 Jun:23(3):256-65 [PubMed PMID: 12169000]
Taalman H, Wallace C, Milev R. Olfactory Functioning and Depression: A Systematic Review. Frontiers in psychiatry. 2017:8():190. doi: 10.3389/fpsyt.2017.00190. Epub 2017 Sep 28 [PubMed PMID: 29033860]
Level 1 (high-level) evidenceO'Donnell ML, Creamer M, Pattison P. Posttraumatic stress disorder and depression following trauma: understanding comorbidity. The American journal of psychiatry. 2004 Aug:161(8):1390-6 [PubMed PMID: 15285964]
Level 3 (low-level) evidenceLemogne C, Smadja J, Zerdazi el-H, Soudry Y, Robin M, Berthoz S, Limosin F, Consoli SM, Bonfils P. Congenital anosmia and emotion recognition: A case-control study. Neuropsychologia. 2015 Jun:72():52-8. doi: 10.1016/j.neuropsychologia.2015.04.028. Epub 2015 Apr 25 [PubMed PMID: 25921869]
Level 2 (mid-level) evidenceMutic S, Brünner YF, Rodriguez-Raecke R, Wiesmann M, Freiherr J. Chemosensory danger detection in the human brain: Body odor communicating aggression modulates limbic system activation. Neuropsychologia. 2017 May:99():187-198. doi: 10.1016/j.neuropsychologia.2017.02.018. Epub 2017 Feb 28 [PubMed PMID: 28254652]
Kentala E, Pyykkö I. Clinical picture of vestibular schwannoma. Auris, nasus, larynx. 2001 Jan:28(1):15-22 [PubMed PMID: 11137358]
Rosahl S, Bohr C, Lell M, Hamm K, Iro H. Diagnostics and therapy of vestibular schwannomas - an interdisciplinary challenge. GMS current topics in otorhinolaryngology, head and neck surgery. 2017:16():Doc03. doi: 10.3205/cto000142. Epub 2017 Dec 18 [PubMed PMID: 29279723]
Wiater JM, Bigliani LU. Spinal accessory nerve injury. Clinical orthopaedics and related research. 1999 Nov:(368):5-16 [PubMed PMID: 10613148]
Sonne J, Reddy V, Lopez-Ojeda W. Neuroanatomy, Cranial Nerve 0 (Terminal Nerve). StatPearls. 2024 Jan:(): [PubMed PMID: 29083731]
Whitlock KE. Origin and development of GnRH neurons. Trends in endocrinology and metabolism: TEM. 2005 May-Jun:16(4):145-51 [PubMed PMID: 15860410]
Level 3 (low-level) evidenceShane Tubbs R, Hose N, Loukas M, De Caro R, Cohen-Gadol AA. Neural connections between the nervus intermedius and the facial and vestibulocochlear nerves in the cerebellopontine angle: an anatomic study. Surgical and radiologic anatomy : SRA. 2016 Jul:38(5):619-23. doi: 10.1007/s00276-015-1571-z. Epub 2015 Oct 15 [PubMed PMID: 26470871]
Gil-Loyzaga P, Bartolomé V, Vicente-Torres A, Carricondo F. Serotonergic innervation of the organ of Corti. Acta oto-laryngologica. 2000 Mar:120(2):128-32 [PubMed PMID: 11603756]
Level 3 (low-level) evidenceDarrow KN, Simons EJ, Dodds L, Liberman MC. Dopaminergic innervation of the mouse inner ear: evidence for a separate cytochemical group of cochlear efferent fibers. The Journal of comparative neurology. 2006 Sep 20:498(3):403-14 [PubMed PMID: 16871528]
Level 3 (low-level) evidenceWarr WB, Boche JB, Neely ST. Efferent innervation of the inner hair cell region: origins and terminations of two lateral olivocochlear systems. Hearing research. 1997 Jun:108(1-2):89-111 [PubMed PMID: 9213126]
Level 3 (low-level) evidenceCastellano-Muñoz M, Israel SH, Hudspeth AJ. Efferent control of the electrical and mechanical properties of hair cells in the bullfrog's sacculus. PloS one. 2010 Oct 29:5(10):e13777. doi: 10.1371/journal.pone.0013777. Epub 2010 Oct 29 [PubMed PMID: 21048944]
Level 3 (low-level) evidenceRyan S, Blyth P, Duggan N, Wild M, Al-Ali S. Is the cranial accessory nerve really a portion of the accessory nerve? Anatomy of the cranial nerves in the jugular foramen. Anatomical science international. 2007 Mar:82(1):1-7 [PubMed PMID: 17370444]
Winkelmann A. Response to "The neglected cranial nerve: nervus terminalis (cranial nerve N)". Clinical anatomy (New York, N.Y.). 2014 Sep:27(6):806-7. doi: 10.1002/ca.22389. Epub 2014 Mar 21 [PubMed PMID: 24659085]
Level 3 (low-level) evidenceVilensky JA. The neglected cranial nerve: nervus terminalis (cranial nerve N). Clinical anatomy (New York, N.Y.). 2014 Jan:27(1):46-53. doi: 10.1002/ca.22130. Epub 2012 Jul 26 [PubMed PMID: 22836597]
Level 3 (low-level) evidenceBuklijas T. The Science and Politics of Naming: Reforming Anatomical Nomenclature, ca. 1886-1955. Journal of the history of medicine and allied sciences. 2017 Apr 1:72(2):193-218. doi: 10.1093/jhmas/jrw046. Epub [PubMed PMID: 28334954]
Kachlik D, Baca V, Bozdechova I, Cech P, Musil V. Anatomical terminology and nomenclature: past, present and highlights. Surgical and radiologic anatomy : SRA. 2008 Aug:30(6):459-66. doi: 10.1007/s00276-008-0357-y. Epub 2008 May 17 [PubMed PMID: 18488135]