Introduction
A craniotomy is a surgical procedure in which a part of the skull is temporarily removed to expose the brain and perform an intracranial procedure.[1] The most common conditions that can be treated via this approach include brain tumors, aneurysms, arterio-venous malformations, subdural empyemas, subdural hematomas, and intracerebral hematomas.[2] Specialized tools and equipment are utilized to remove the section of bone, which is called the bone flap. The bone flap is temporarily removed, held at the surgical instrument table, and then placed back after the brain surgery has concluded. In some cases, depending on the etiology and indication for the procedure, the bone can be discarded, stored in the abdominal subcutaneous space, or cryopreserved under cold storage conditions.[3] If the bone flap is discarded or not placed back into the skull during the same operation, the procedure is called a craniectomy. In a decompressive craniectomy used for the treatment of malignant brain edema, the bone flap is placed back a few weeks after the brain swelling has improved.[4][5] The surgical procedure to reconstruct and place the bone flap back into the skull during a second intervention is known as cranioplasty.[6]
From a historical context and perspective, cranial interventions varied from a single burr hole trephine to a larger craniectomy. Modern craniotomies are performed by connecting a series of burr holes. Although trephination is the oldest cranial surgical technique with ancient reports dating back to 2300 years, our current modern surgical technique for a craniotomy is the final cured result of the procedure introduced at the end of the 19th century by the self-educated surgeon Wilhelm Wagner.[1][7][8] Although it was much later in the course of history that the transition from trephination to a tailored resection via craniotomy happened, ancient civilizations, such as the Incas in Peru, must have had some basic familiarity with anatomy and surgical interventions despite their rudimentary knowledge of pathology.[7][9]
Depending on the type of intracranial lesion, pathology, and the surgical approach, some craniotomy procedures can be assisted by neuronavigation guidance based on magnetic resonance imaging or computed tomographic scans to tailor the procedure to the size of the tumor using the smallest incision possible. Neuronavigation is a modern computerized technology that can help surgeons localize the pathology more precisely by merging a series of craniofacial points in the patient. Neuronavigation offers better guidance, orientation, and localization. It provides a higher level of confidence for the surgeon and an improved outcome for the patient.[10]
History
The craniotomy approach has evolved over time. Trepanation, meaning “borer” became synonymous with trephination because of the French instrument tres fines meaning “three ends”.[11] Trephination has been found to be performed by prehistoric men either for magic or religious rituals to release demons and malignant spirits or to wear them as amulets as early as 1783. During the neolithic era, therapeutic drilling was performed by pointed or sharp cutting tools made up of silica or obsidian.[12] The principle of bow drilling was obtained from that of fire-making and was used by the Egyptians in 1400 years BC. The approach to craniotomy has been presumed to be written by Imhotep around 2900 BCE.[12] The therapeutic usage of craniotomy for managing fractures was undertaken in the 5 Century BC by Hippocrates. The instruments were detailed as early as 1518 in “De fractura calvae” by Berengario. Celso advocated trephination sequentially involving the external cortex, diploic tissue, and lastly internal cortex, safeguarding the meninges. Craniotomy evolved in the Renaissance period (firearms and grenades) in the 16th and 17th centuries. The use of angulated manual trephines, equipped with a series of perforating or cutting terminals, was applied in the 16th century. In 1889 Wagner first performed an osteoplastic bone flap. Gigli saw was used by Obalinski in 1897. Beginning of the 19th Century the use of craniotomy declined mostly due to infections and trephining was limited to exceptional cases. Advancement in antisepsis and general anesthesia in the 19th century led to the exponential growth of trephining and craniotomy.[12][13]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
There are many types of craniotomies described in the literature, and a basic understanding of anatomy and physiology is necessary to perform an adequate craniotomy with fewer complications. The type of craniotomy is named depending on the skull bone, which is opened. Typical skull bones targeted for craniotomy include the frontal, parietal, temporal, and occipital bones. Depending on the location of the pathology to be addressed, supratentorial or infratentorial (posterior fossa) craniotomies can be utilized.
One of the most traditional craniotomies utilized is the pterional craniotomy, a supratentorial craniotomy that can be utilized for aneurysms of the anterior circulation, basilar tip artery aneurysms, direct surgical approaches to the cavernous sinus, frontal and temporal lobe tumors, as well as suprasellar tumors such as pituitary adenomas and craniopharyngiomas.[14][15][16][17] Another type of supratentorial craniotomy is the temporal or subtemporal craniotomy, which can be utilized for temporal lobe biopsy, temporal lobectomy, temporal epilepsy surgery, temporal lobe tumors, as well as access to the floor of the middle cranial fossa.[18][19]
The frontal craniotomy is used to access the frontal skull base and the frontal lobe of the brain for approaches to the third ventricle or sellar region tumors, craniopharyngiomas, planum sphenoidale meningiomas, frontal lobe tumors, and repair of anterior cerebrospinal fluid fistulas. Other types of craniotomies include parietal, occipital, and retrosigmoid, among many others.[20]
Indications
Indication for craniotomy:
Trauma
- Acute extradural hematoma, acute subdural hematoma, brain contusions, depressed skull fractures, intracranial foreign bodies, and cerebrospinal fluid (CSF) leak repair.
Tumor
- Meningioma, high-grade and low-grade glioma, epidermoid, ependymoma, oligodendroglioma, metastases, orbital tumors, cerebellopontine angle tumors, sellar and parasellar lesions.
Vascular
- Intracerebral hemorrhage, Malignant Middle cerebral artery (MCA) territory infarction, cortical venous thrombosis (CVT) with hemorrhagic infarction, aneurysms, and vascular malformations (arterio-venous malformation, cavernous angioma, arterio-venous fistula).
- Microvascular decompression.
Infectious
- Abscess, subdural empyema.
Parasitic lesions
- Hydatid cyst, Racemose neurocysticercosis (NCC)
Miscellaneous
Contraindications
There are very few contraindications to performing a craniotomy:
- High anesthetic risks: advanced age, severe medical comorbidities
- Morribond state
- Poor functional status
- High frailty index
- Severe systemic collapse (sepsis, multiorgan failure)
- Coagulation disorders
- Bleeding dyscrasias, and
- Pathologies that can be addressed by a single burr hole.[34]
Absolute contraindication for awake craniotomy:
- Patient refusal, and
- Non-complaint patient.
Relative contraindication for awake craniotomy:
- Obese patients
- Obstructive sleep apnea,
- Difficult airways
- Chronic refractory cough
- Highly vascular lesions, and
- Posterior fossa lesions.[35]
Equipment
A craniotomy is a surgical procedure that requires specific equipment. The following are the requirements to perform a craniotomy:
- Suction tips
- Bipolar cautery forceps
- Scalpel handle and blades
- Needle holders
- Hemostatic clip
- Scalp retractors
- Periosteal elevator
- Bayonet forceps
- Adson forceps
- Head-fixation system
- High-speed pneumatic cranial drill (craniotome)
- Hudson brace with perforating bit attached
- Round burr for Hudson brace
- Gigli wire saw, guide, and handles
- Perforating bits and narrow burr attachment and extension piece
- Bone curette
- Kerrison bone rongeur
- Penfield dissector
- Gerald forceps
- Hemostatic agents (bone wax,surgicel), and
- Dural scissors. [36]
Personnel
An interprofessional team is required to carry out a craniotomy successfully. Following are the person whose input is mandatory:
- Neurosurgeon
- Operating room head nurse
- Surgical technologist (operating room technologist)
- Anesthesiologist
- Anesthetist, and
- Intensive care unit nursing personnel.
Preparation
Preoperatively, the patient must be in the best optimal condition possible to tolerate the procedure. The patient must be with an empty stomach or "nil per os" (NPO), a Latin phrase that translates to "nothing through the mouth" in the English language. In emergency cases, this is usually not possible. Blood-thinning medications such as antiplatelet or antithrombotics should be discontinued between 3 to 10 days preoperatively, depending on the drug.[37] Internal medicine or cardiology evaluation for medical clearance should be obtained for recommendations and surgical risk.
Unless otherwise required, most craniotomy procedures are performed under general anesthesia, requiring a case discussion with the anesthesiology team for any pertinent details regarding the etiology to be treated. Sometimes, an awake craniotomy is performed under a local anesthetic agent to be able to communicate with the patient during surgery involving motor and speech areas.[38][39][40][41] Specific patient preoperative considerations include the patient's procedure informed consent, procedure time-out identifying the correct patient and side of surgical intervention, and blood availability in case it is needed for transfusion during the surgery.[42]
Routine preoperative antibiotics are administered before the procedure starts for wound infection prophylaxis, jointly with other medications that could be necessary, such as anticonvulsant medications or corticosteroids. Initial setup of equipment such as neuronavigation system, surgical microscope, and neuromonitoring are performed. Intensive care unit availability should be discussed preoperatively, as most patients do require this level of care after a craniotomy.
Anesthesia during craniotomy:
- General
- Awake
Awake anesthesia (AA) is comparable mostly in terms of operative and functional outcomes to that of GA. [43]
Propofol-maintained and volatile-maintained anesthesia have similar brain relaxation scores, however, mean intracranial pressure (ICP) values were lower, and cerebral perfusion pressure (CPP) values were higher with propofol-maintained anesthesia. [44]
Technique or Treatment
Once the patient is under anesthesia, the correct position of the head is fixed depending on the approach to be utilized. It is of utmost importance to avoid any pressure points on vulnerable body areas by adequately padding throughout. The location of the incision for the craniotomy depends on the part of the brain to be operated on. If the surgical craniotomy is assisted by neuronavigation, anatomical points are confirmed before the incision at this time.
For surgery in the supratentorial area, the incision is usually made over the frontal, temporal, parietal, or occipital bones or over a combination of bones. For surgery in the infratentorial area, the incision is usually made over the back portion of the skull below the transverse sinus. After the desired location of the incision is chosen on the skin, the hair in the area may be shaved off.[36] The incision should preferably be behind the hairline for cosmetic reasons. Once the incision is confirmed, the surgical area is cleaned with the preferred antiseptic agent, followed by routine sterile draping techniques. A local anesthetic with epinephrine is usually injected into the marked skin incision to help with hemostasis.
After the skin incision is made, the muscles below the scalp are dissected to expose the skull. Retractors can be placed on the edges of the incision to have adequate exposure to the surgical area to be focused on. Alternatively, fish hook retractors or sutures can be used to hold the scalp flap. The pericranium can be separated to be used as a dural substitute if necessary during the closure. Several burr holes are made into the skull utilizing the craniotome or cranial drill.[36] Caution has to be employed to avoid plunging the craniotome into the brain tissue. The holes are cleaned from any bone fragment, and the dura is separated with a Freer elevator or Penfield dissector. The burr holes are connected with a craniotome saw, and a bone flap is elevated after carefully separating it from the dura matter below. The bone flap is held in the surgical instrument table until the closure portion of the surgery. For the intradural procedure, the dura is cut and retracted, exposing the brain.
Once the surgery on the brain concludes, the bone is reattached in position with plates and screws. Adequate hemostasis should be obtained before closing the scalp. The overlying tissues are reattached, and the scalp is then sutured in anatomical layers. Depending on the surgeon’s preference, a subdural or subgaleal drain can be left in place to drain the accumulated blood products.
Systematic review supports the use of Regional scalp block (RSB). [45]
The dictum of craniotomy:
- Adequate surgical exposure to the underlying lesion.
- Shortest traversal to the target.
- Should encompass minimal normal brain retraction.
- Incision
- The incision should be tailored to the lesion.
- Emphasis is focused on wound healing and cosmetic aspects.
- Should be mostly placed behind the hairline.
- Skin incision should ideally be along Langer’s line (skin tension lines).
- Coronal incision gives better exposure and cosmetic result as preserves all aesthetic units of the forehead.
- The base of the flap should be wider with its length not more than 1.5 times the base of the flap.
- Safeguard the vascularity of the flap (should be ideally based on at least two named arteries) avoiding crossed incisions.
Positioning of the patient should encompass:
- Direct access to the surgical target.
- Promote gravity-assisted brain retraction.
- Should ensure effective cerebral venous return and airway patency.
- Comply with the surgical ergonomics.
Head fixation
Based upon three-point rigid cranial fixation constituting of two-point swivel arm and a contralateral single pin. It should avoid:
- The course of skin incision
- Pneumotized sinuses
- Sutures
- Dural venous sinuses
- Neurovascular structures (superficial temporal artery, supraorbital artery, and nerve, occipital artery),and
- Thin calvaria such as temporal squamosa, pterion.
The maximum allowable pin pressure is 80 lbs.
Steps during craniotomy:
- Thorough preoperative assessment.
- Proper positioning of the patient.
- Adequate scalp preparation.
- Stringent scalp toileting.
- Marking of the appropriate incision.
- Proper draping of the surgical site.
Types:
- Trephine craniotomy
- Flap craniotomy: Free bone flap or osteoplastic
- Keyhole Craniotomy
- Stereotactic Craniotomy
The salient steps of the procedure:
Types of flaps:
- Bicoronal/Souttar flap
- Frontal flap
- Temporal flap
- Pterional (fronto-temporal) flap
- Fronto-temporo-parietal (question mark) flap
- Horseshoe flap
- Occipital skin (Mitre) flap
- Midline suboccipital incision
- Retromastoid skin incision
- Linear and curvilinear incisions
Bicoronal/ Souttar flap
- Starts from the superior aspect of the zygomatic arch, 1 cm anterior to the tragus courses over the bregma to the corresponding contralateral side. The flap is reflected anteriorly up to the supra-orbital rim.
Frontal
- Can be unilateral or bifrontal.
- It curves course along the coronal suture to end at the mid-hairline.
- Performed for exposure of lesions within the anterior interhemispheric, sellar, lamina terminalis, and anterior third ventricular regions.
Temporal
- A linear or question mark incision.
- Based on the zygoma, goes behind the ear, then courses just above the superior temporal line up to the hairline anteriorly.
- Provides access to the middle fossa, anterior superior brainstem, trigeminal, petroclival lesions, and basilar aneurysm.
- Can be combined with an anterior petrosectomy.[12]
Parietal
- Interhemispheric approach for parafalcine, medial parietal, and splenial lesions.
- The transcortical route through the non-eloquent superior parietal lobule.
- Should spare the motor and sensory cortices via Cortical mapping, navigation, or functional MRI (fMRI).
Pterional (Frontotemporal)
- Developed by Gazi Yasargil.
- Centered on the pterion.
- Allow access to the frontal and temporal operculum, Sylvian fissure, and supra-sellar cisterns.
- Can be combined with a sub-frontal approach for exposing the anterior cranial fossa.[12]
Orbitozygomatic (OZ)
- First described by Pellerin and Hakuba.
- Can be one or two-piece osteotomies. The two-piece approach is made by removing a traditional pterional bone flap followed by a supraorbital craniotomy.
- Used for lesions within the orbital apex, paraclinoid, and para-sellar areas, the cavernous sinuses, the basal cisterns, and the upper clivus.[12]
Trauma flap
- For traumatic lesions, and malignant MCA infarct.
- Based on zygoma.
- Blood supply from superficial temporal and supraorbital vessels.
- Curves around 3.5 cm posterior to the external auditory meatus.
Retrosigmoid
- Popularized by Woolsey and Krause as the lateral suboccipital approach.
- Vertical incision 1 cm medial to mastoid.
- Can be a ‘Lazy S’ incision, or an inverted ‘J’/Hockey stick incision.
- Provides access to the cerebellopontine and cerebellomedullary cisterns.
- Also applied for neurovascular decompression.[12]
Horseshoe flap
- Inverted ‘U’ shape to expose any part of cerebral convexity.
Mitre skin flap
- Vertical limb extends from inion to vertex.
- The anterior limb eclipse the posterior parietal region towards the ear.
- Vascularity is based on the occipital artery.
- Applied for assessing lesions on the occipital lobe, posterior falx, and superior tentorial surface.
Suboccipital
- Developed by Rand and Yasargil.
- Extends from external occipital protuberance (EOP) to C2 level.
- Allows exposure of the cerebellar hemispheres, tonsils, vermis, medulla, fourth ventricle, craniocervical junction, and foramen magnum.[12]
Burr hole:
- A handheld drill like a Hudson brace or motorized drill attached to a perforating bit.
- Kept perpendicular to the skull and turned rapidly.
- Difficult initially to penetrate the outer but relatively easy through the cancellous bone.
- Cogwheel resistance is felt once the inner cortex is engaged.
- Visually inspect to confirm the breach of the inner cortex.
- The drill is substituted with a sharp bone curette or a round burr for the Hudson brace to safely enlarge the hole.
- Bone wax is applied to the edges of the burr. [36]
Bone flap:
- Direct and shortest access to the target.
- Centered over lesion for convexity lesions.
- Careful separation of underlying dura with Penfield’s dissector.
- Beveling to avoid sinking of the bone flap.
- The cuts along /across dural venous sinuses should be performed last.
- Liberal dural hitch/tack-up stitches to prevent and minimize dural bleeding.
Durotomy
- Epidural tacking sutures should be applied.
- Flap based on sinuses should be made.
- First opened with the help of a sharp hook and knife.
- Further opening with dural scissors with the placement of cottonoid beneath.
- Keep a suitable cuff of dura for closure at the end of the procedure.
Wound closure
- Dural repair should be watertight but not under undue tension.
- Bone flap replacement whenever feasible.
- Use of monofilament sutures- resist the ingress of bacteria, have minimal drag, and tissue reactivity.
- Should obliterate all potential dead space.
- Even distribution of tension on the suture line.
- Adequate tensile strength of the suture is needed.
- Tension-free closure.
- Interrupted suture better preserves galeal vessels supplying the scalp.
- Skin is closed in two layers.
Augmented and virtual reality (AR, VR) assisted awake craniotomy for lesions within the eloquent regions can supplement, augment, or even replace conventional approaches. [46]
Post-procedure management
Routine ward admission appears safe in most patients. Approximately 2% of unplanned intensive care unit (ICU) admission are reported. Factors such as:
- Lengthy operation
- Profound blood loss
- High anesthetic risks
- New neurological and lower cranial nerve deficits
- Reduced consciousness or deficits of the lower cranial nerves, and
- Provisions for delayed extubation necessitate ICU admission. [47][48]
Factors to take into account for ICU admission include:
- Patient-specific risk factors: age, neurological status, anesthesia-associated risks, frailty index, and medical comorbidities.
- Surgical factors: location, size and type of the lesion, surgical type and approach, duration of surgery, nature of procedures (elective Vs. emergency), and perioperative complications.
- Anticipated postoperative complications: stringent neurological and hemodynamic assessment, and management of hormonal or electrolyte imbalance such as systemic inappropriate anti-diuretic hormone (SIADH), diabetes insipidus (DI), or cerebral salt wasting (CSW).
Univariate analysis showed diabetics, intra-operative high blood loss, need for blood transfusion, older patients, and longer surgical procedures whereas multivariate analysis showed diabetes and age as predictive variables of the need for postoperative intensive care unit admission. [49]
A "safe transition pathway" model has to be adopted.
General postoperative management:
- Stringent neurological assessment and monitoring
- Hemodynamic stability
- Seizure prophylaxis
- Adequate analgesia and sedation-Opioids, paracetamol/NSAIDs, and regional anesthesia are effective.[50]
- Fluid and electrolyte monitoring
- Chest physiotherapy
- Nutritional support, and
- Deep venous thrombosis (DVT) prophylaxis-low molecule weight heparin (LMWH) and intermittent compression devices (ICDs) are both effective in the prevention of VTE. [51]
The enhanced Recovery after Surgery (ERAS)principle incorporates:
- Mental state assessment
- Antimicrobial, steroidal, and antiepileptic prophylaxes
- Nutritional assessment
- Postoperative nausea and vomiting (PONV) prophylaxis
- Regional field block or scalp block
- Avoidance, minimization, and early removal of invasive monitoring
- Use of absorbable skin sutures
- Avoidance of wound drains
- Early extubation
- Early mobilization
- Early fluid de-escalation
- Early initiation of oral intake, and
- Early postoperative imaging.[52]
Multimodal monitoring and patient-centered optimization of neurosurgical care in the perioperative period are pivotal.[52][53]
Complications
Complications of head fixation devices:
- Scalp laceration
- Skull fractures
- Pin site infections and osteomyelitis
- Venous air embolism and
- Acute epidural, subdural hematoma, and brain contusions.
Complications increased in
- Prone/lateral prone
- Emergency cases
- Low depth of anesthesia
- Increased length of operation, and
- Thin scalp.[54]
Scalp Flap necrosis
Specific complications to flaps:
Frontal flaps:
- Cosmetic deformity
- Cerebrospinal fluid (CSF) leak
- Injury of the superior sagittal sinus
- Retraction-induced bilateral frontal lobes injury.[12]
Temporal flaps:
- The vein of Labbe injury.[12]
- Temporal hollowing: Preserving the temporalis origin and avoiding dissection between the leaflets of the deep temporal fascia or intermediate fat pad minimizes temporal hollowing.[55]
Parietal flaps:
- Injury to the vein of the Trolard
- Injury to the superior sagittal sinus and overlying cortical veins- bleeding and sinus/cortical vein thrombosis
- Injury to the motor cortex.[12]
Pterional flaps:
- The frontal sinus may be violated
- The frontalis branches of the facial nerve may be injured
- Osteotomy involving the sphenoid may extend into the optic canal.[12]
Orbitzygomatic flaps
- Fractures of the orbital roof and rim lead to injury of the optic nerve
- Fractures of the sphenoid and ethmoid sinuses can cause CSF leaks
Retrosigmoid flaps:
- Injury to the lesser occipital and greater auricular nerves causes postoperative headache and dysesthesia
- Retraction injury to the cerebellum
- Transverse, sigmoid, torcula, and occipital venous sinuses injury
- Damage to the cranial nerves and brainstem
- CSF leaks and pseudomeningocele
- The mastoid emissary vein can cause substantial bleeding and be a source of air embolism.
- Injury to the vertebral artery
- Bone-dust-induced meningitis.[12]
Suboccipital:
- Pooling of the blood within the operative bed limit visibility in prone positioning
- Pressure on eyes and face in prone positioning
- The sitting position has the risk of venous air embolism and hemodynamic instability
- Injury to the transverse, sigmoid, torcula, and occipital venous sinuses
- CSF leak and pseudomenigocele.
- Cerebellar mutism.
Complications of burr holes, craniotomy, and durotomy :
- Opening of air sinus: remove mucosa, pack with betadine-shocked gel foam, and covered with wax or vascularized flap
- Bone bleed: controlled with bone wax
- Dural venous sinus injury: packed or sewn
- Dural lacerations
- Injury to cortical draining veins, and
- The drill perforator plunge into the brain with a cerebral contusion.[56]
Post-procedure complications of craniotomy:
- Post-craniotomy headache.[2]
- Extraxial hematomas
- Seizures: Levetiracetam is superior to phenytoin for De novo seizure following craniotomy (DSC).[57]
- Electrolyte abnormalities: the most common being hyponatremia and hypernatremia
- Tension pneumocephalus
- Postoperative infection: the incidence of postoperative meningitis is 2.2%. Gram-negative organisms are the most common cause and overall mortality rate of 5%.
- Intracranial hemorrhage (ICH)
- Ventilator-associated pneumonia (VAP): via bronchoalveolar lavage and endotracheal tube aspirate
- Cerebral edema
- Cerebral ischemia
- Vasospasm
- Pneumocephalus
- CSF leak: A systematic review has shown that dural sealants do not reduce the number of CSF leaks but minimize the risk of surgical-site infection.[58]
- Hydrocephalus, and
- Infection: soft tissue infections, extradural abscess, empyema, and bone flap infection.[59]
A study has shown that variables such as:
- American Society of Anesthesiologists score (>2)
- Other infection
- Duration of operation > 4 hours
- Sinus entry
- CSF leak (OR 7.817)
- CSF drainage
- Surgical drain
- Number of previous operations, and
- Implants were significant variables for surgical site infections (SSIs).[60][61][62] Meta-analysis has shown prophylactic antibiotics significantly minimize the risk of meningitis after craniotomy.[63]
The reported incidence of major complications is 8.3%, with minor complications rising up to 60%. Mortality owing to major complications is reportedly 22% (0.5% in minor complications).[62]
Variables associated with major complications include:
- Age
- An abnormal neurological examination after the end of the surgery, and
- Intra-operative desaturation.[62]
Clinical Significance
The surgical procedure of craniotomy has become one of the essential procedures in modern healthcare for neurological disorders. Before the advent of this procedure, many patients were not able to survive conditions that today are treated daily. Disorders ranging from brain tumors, vascular pathologies, and trauma are routinely treated, which could produce devastating damage to the patient if access to the intracranial cavity was limited. The procedure itself has been modernized and will continue to do so with the advent of new technology as it is developed. Since its beginnings, it has produced a revolution in neurosurgical and neurological patient care.
Depending on the specific type of pathology to be addressed and the clinical judgment of the physician, it is determined if a craniotomy is necessary for the patient. Even with the new endovascular techniques to treat intracranial vascular disorders and the radiosurgery technique to treat intracranial tumors, craniotomy remains the primary tool for the treatment of the majority of neurosurgical pathologies.
Scores used in assessing postoperative outcomes include:
- Preoperative American society of anesthesiologists (ASA) physical status classification
- Karnofsky performance score (KPS)
- Charlson co-morbidity score
- Modified Rankin Scale and
- Sex, KPS, ASA physical status classification, location, and edema (SKALE).[64]
KPS has the strongest evidence for predicting surgery-related outcomes.No scores strongly predict nonsurgical outcomes after elective craniotomies. KPS and ASA physical status classification predict early (≤ 30-day) morbidity in tumor patients. The Charlson co-morbidity predicts mortality of elective aneurysms. [64]
Enhancing Healthcare Team Outcomes
To enhance healthcare team outcomes, measures should aim to provide the safest yet most effective intervention for the patient. Different improvement strategies aiming to improve patient care and healthcare team outcomes can be implemented and divided into preoperative, intraoperative, and postoperative.
Preoperative measures start in the emergency department once the patient arrives or in the outpatient clinic. An interprofessional approach to patient care after successful communication between the neurosurgeon, emergency department physician, internal medicine physician, or cardiologist improves outcomes.
Intraoperatively, effective communication between the team members in the operating room is always needed. This communication will ensure the correct patient is operated, on and the correct procedure is performed on the right side, minimizing potential errors or mistakes. Patient safety should be the top priority at all times. All personnel needs to know the procedure to be performed and how it is performed. For intraoperative neuromonitoring, technicians become part of the essential team that will provide the best care for the patient. Experienced neurosurgeons provide the patient with the best result and outcomes for those complicated and rare cases. Neuroanesthesiologists are very important during the wake-up process to avoid coughing or agitation to prevent bleeding into the surgical area.[65][66]
During the postoperative period, once the patient wakes up from anesthesia, nursing personnel from the recovery room and intensive care unit communicate to transfer and receive the patient. Pharmacists will also become an integral part of the team needed for the essential care of the patient by providing treatment recommendations and modifications.
Nursing, Allied Health, and Interprofessional Team Interventions
Team-based practices are necessary for performing a successful craniotomy procedure. Interaction between the neurosurgeon and the anesthesiologist usually happens even before the patient is in the operating room by discussing the case and the desired approach. Discussing the necessary equipment with the operating room head nurse is essential. A discussion of non-anesthetic agents to be administered by the anesthetist takes place before commencing the incision. Once the patient is under general anesthesia, effective communication between the anesthesia team and the neurosurgeon during the procedure minimizes complications and unexpected events.
Postoperative care for a patient who has undergone a craniotomy also involves an interprofessional team including intensive care unit nursing personnel, and in some cases, speech pathologists, physical medicine and rehabilitation physician, practical nurses, physical therapists, respiratory therapists, and even discharge planning team and social work team personnel.[67]
Media
(Click Image to Enlarge)
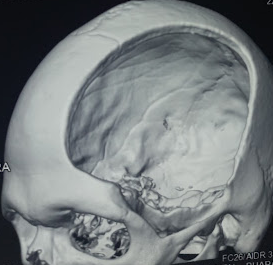
Decompressive hemicraniectomy Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)
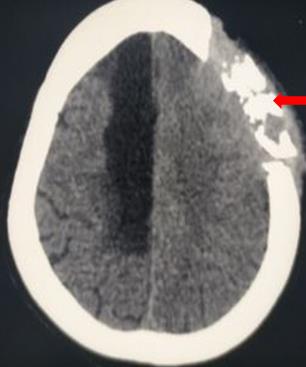
Osteomyelitis Contributed by Sunil Munakomi, MD
References
González-Darder JM, [History of the craniotomy]. Neurocirugia (Asturias, Spain). 2016 Sep-Oct; [PubMed PMID: 27006140]
Subbarao BS,Eapen BC, Post Craniotomy Headache 2020 Jan; [PubMed PMID: 29493922]
Bhaskar IP,Zaw NN,Zheng M,Lee GY, Bone flap storage following craniectomy: a survey of practices in major Australian neurosurgical centres. ANZ journal of surgery. 2011 Mar; [PubMed PMID: 21342384]
Level 3 (low-level) evidenceSchizodimos T,Soulountsi V,Iasonidou C,Kapravelos N, An overview of management of intracranial hypertension in the intensive care unit. Journal of anesthesia. 2020 May 21; [PubMed PMID: 32440802]
Level 3 (low-level) evidenceSahuquillo J,Dennis JA, Decompressive craniectomy for the treatment of high intracranial pressure in closed traumatic brain injury. The Cochrane database of systematic reviews. 2019 Dec 31; [PubMed PMID: 31887790]
Level 1 (high-level) evidenceAlkhaibary A,Alharbi A,Alnefaie N,Aloraidi A,Khairy S, Cranioplasty: A Comprehensive Review of the History, Materials, Surgical Aspects and Complications. World neurosurgery. 2020 May 5; [PubMed PMID: 32387405]
Rifkinson-Mann S, Cranial surgery in ancient Peru. Neurosurgery. 1988 Oct; [PubMed PMID: 3059210]
Buchfelder M, From trephination to tailored resection: neurosurgery in Germany before World War II. Neurosurgery. 2005 Mar; [PubMed PMID: 15730586]
Andrushko VA,Verano JW, Prehistoric trepanation in the Cuzco region of Peru: a view into an ancient Andean practice. American journal of physical anthropology. 2008 Sep; [PubMed PMID: 18386793]
Enchev Y, Neuronavigation: geneology, reality, and prospects. Neurosurgical focus. 2009 Sep; [PubMed PMID: 19722813]
Hobert L,Binello E, Trepanation in Ancient China. World neurosurgery. 2017 May; [PubMed PMID: 27769950]
Rao D,Le RT,Fiester P,Patel J,Rahmathulla G, An Illustrative Review of Common Modern Craniotomies. Journal of clinical imaging science. 2020; [PubMed PMID: 33408956]
Sperati G, Craniotomy through the ages. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale. 2007 Jun; [PubMed PMID: 17883195]
Yasargil MG,Antic J,Laciga R,Jain KK,Hodosh RM,Smith RD, Microsurgical pterional approach to aneurysms of the basilar bifurcation. Surgical neurology. 1976 Aug; [PubMed PMID: 951657]
Yaşargil MG,Reichman MV,Kubik S, Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. Journal of neurosurgery. 1987 Sep; [PubMed PMID: 3612281]
Hendricks BK,Cohen-Gadol AA, The Extended Pterional Craniotomy: A Contemporary and Balanced Approach. Operative neurosurgery (Hagerstown, Md.). 2020 Feb 1; [PubMed PMID: 31172173]
Choque-Velasquez J,Hernesniemi J, One burr-hole craniotomy: Lateral supraorbital approach in Helsinki Neurosurgery. Surgical neurology international. 2018; [PubMed PMID: 30159200]
Choque-Velasquez J,Hernesniemi J, One burr-hole craniotomy: Subtemporal approach in helsinki neurosurgery. Surgical neurology international. 2018; [PubMed PMID: 30186665]
Zieliński G,Sajjad EA,Robak Ł,Koziarski A, Subtemporal Approach for Gross Total Resection of Retrochiasmatic Craniopharyngiomas: Our Experience on 30 Cases. World neurosurgery. 2018 Jan; [PubMed PMID: 28987834]
Level 3 (low-level) evidenceZhou C,Evins AI,Boschi A,Tang Y,Li S,Przepiorka L,Sadhwani S,Stieg PE,Xu T,Bernardo A, Preoperative identification of the initial burr hole site in retrosigmoid craniotomies: A teaching and technical note. The international journal of medical robotics computer assisted surgery : MRCAS. 2019 Jun; [PubMed PMID: 30721556]
Stachniak JB,Layon AJ,Day AL,Gallagher TJ, Craniotomy for intracranial aneurysm and subarachnoid hemorrhage. Is course, cost, or outcome affected by age? Stroke. 1996 Feb; [PubMed PMID: 8571423]
Legnani FG,Saladino A,Casali C,Vetrano IG,Varisco M,Mattei L,Prada F,Perin A,Mangraviti A,Solero CL,DiMeco F, Craniotomy vs. craniectomy for posterior fossa tumors: a prospective study to evaluate complications after surgery. Acta neurochirurgica. 2013 Dec; [PubMed PMID: 24078114]
Hamasaki T,Morioka M,Nakamura H,Yano S,Hirai T,Kuratsu J, A 3-dimensional computed tomographic procedure for planning retrosigmoid craniotomy. Neurosurgery. 2009 May; [PubMed PMID: 19404104]
Broggi G,Broggi M,Ferroli P,Franzini A, Surgical technique for trigeminal microvascular decompression. Acta neurochirurgica. 2012 Jun; [PubMed PMID: 22531963]
Rauen K,Reichelt L,Probst P,Schäpers B,Müller F,Jahn K,Plesnila N, Decompressive Craniectomy Is Associated With Good Quality of Life Up to 10 Years After Rehabilitation From Traumatic Brain Injury. Critical care medicine. 2020 May 18; [PubMed PMID: 32433123]
Level 2 (mid-level) evidenceAlvis-Miranda H,Castellar-Leones SM,Moscote-Salazar LR, Decompressive Craniectomy and Traumatic Brain Injury: A Review. Bulletin of emergency and trauma. 2013 Apr; [PubMed PMID: 27162826]
Schaller K,Cabrilo I, Anterior temporal lobectomy. Acta neurochirurgica. 2016 Jan; [PubMed PMID: 26596998]
Duckworth EA,Vale FL, Trephine epilepsy surgery: the inferior temporal gyrus approach. Neurosurgery. 2008 Jul; [PubMed PMID: 18728594]
Yang PF,Zhang HJ,Pei JS,Lin Q,Mei Z,Chen ZQ,Jia YZ,Zhong ZH,Zheng ZY, Keyhole epilepsy surgery: corticoamygdalohippocampectomy for mesial temporal sclerosis. Neurosurgical review. 2016 Jan; [PubMed PMID: 26277790]
Smyth MD,Tenenbaum MJ,Kaufman CB,Kane AA, The [PubMed PMID: 17328272]
Akai T,Shiraga S,Sasagawa Y,Iizuka H,Yamashita M,Kawakami S, Troubleshooting distraction osteogenesis for craniosynostosis. Pediatric neurosurgery. 2013; [PubMed PMID: 25500456]
Alford J,Derderian CA,Smartt JM Jr, Surgical Treatment of Nonsyndromic Unicoronal Craniosynostosis. The Journal of craniofacial surgery. 2018 Jul; [PubMed PMID: 29570518]
Ciporen J,Lucke-Wold B,Gillham H,Cua D,Kim J,Akins P, Paramedian Forehead Flap for Repair of Refractory High-Flow Anterior Skull Base CSF Leak. Turkish neurosurgery. 2017 Jul 11; [PubMed PMID: 28944942]
Sivanaser V,Manninen P, Preoperative assessment of adult patients for intracranial surgery. Anesthesiology research and practice. 2010; [PubMed PMID: 20700431]
Singh K,Dua A, Anesthesia For Awake Craniotomy. StatPearls. 2022 Jan [PubMed PMID: 34283419]
Donovan DJ,Moquin RR,Ecklund JM, Cranial burr holes and emergency craniotomy: review of indications and technique. Military medicine. 2006 Jan; [PubMed PMID: 16532867]
Greuter L,Ullmann M,Mariani L,Guzman R,Soleman J, Effect of preoperative antiplatelet or anticoagulation therapy on hemorrhagic complications in patients with traumatic brain injury undergoing craniotomy or craniectomy. Neurosurgical focus. 2019 Nov 1; [PubMed PMID: 31675713]
Bilotta F,Rosa G, 'Anesthesia' for awake neurosurgery. Current opinion in anaesthesiology. 2009 Oct; [PubMed PMID: 19623055]
Level 3 (low-level) evidenceFang S,Li Y,Wang Y,Zhang Z,Jiang T, Awake craniotomy for gliomas involving motor-related areas: classification and function recovery. Journal of neuro-oncology. 2020 Apr 29; [PubMed PMID: 32350781]
O'Neill M,Henderson M,Duffy OM,Kernohan WG, The emerging contribution of speech and language therapists in awake craniotomy: a national survey of their roles, practices and perceptions. International journal of language [PubMed PMID: 31778003]
Level 3 (low-level) evidenceÖzlü O, Anaesthesiologist's Approach to Awake Craniotomy. Turkish journal of anaesthesiology and reanimation. 2018 Aug; [PubMed PMID: 30140530]
Oszvald Á,Vatter H,Byhahn C,Seifert V,Güresir E, [PubMed PMID: 23116101]
Lu VM,Phan K,Rovin RA, Comparison of operative outcomes of eloquent glioma resection performed under awake versus general anesthesia: A systematic review and meta-analysis. Clinical neurology and neurosurgery. 2018 Jun; [PubMed PMID: 29655013]
Level 1 (high-level) evidenceChui J,Mariappan R,Mehta J,Manninen P,Venkatraghavan L, Comparison of propofol and volatile agents for maintenance of anesthesia during elective craniotomy procedures: systematic review and meta-analysis. Canadian journal of anaesthesia = Journal canadien d [PubMed PMID: 24482247]
Level 1 (high-level) evidenceGuilfoyle MR,Helmy A,Duane D,Hutchinson PJA, Regional scalp block for postcraniotomy analgesia: a systematic review and meta-analysis. Anesthesia and analgesia. 2013 May; [PubMed PMID: 23477962]
Level 1 (high-level) evidenceMofatteh M,Mashayekhi MS,Arfaie S,Chen Y,Mirza AB,Fares J,Bandyopadhyay S,Henich E,Liao X,Bernstein M, Augmented and virtual reality usage in awake craniotomy: a systematic review. Neurosurgical review. 2022 Dec 19; [PubMed PMID: 36529827]
Level 1 (high-level) evidenceBadenes R,Prisco L,Maruenda A,Taccone FS, Criteria for Intensive Care admission and monitoring after elective craniotomy. Current opinion in anaesthesiology. 2017 Oct; [PubMed PMID: 28682828]
Level 3 (low-level) evidenceBui JQ,Mendis RL,van Gelder JM,Sheridan MM,Wright KM,Jaeger M, Is postoperative intensive care unit admission a prerequisite for elective craniotomy? Journal of neurosurgery. 2011 Dec; [PubMed PMID: 21888476]
Level 2 (mid-level) evidenceHanak BW,Walcott BP,Nahed BV,Muzikansky A,Mian MK,Kimberly WT,Curry WT, Postoperative intensive care unit requirements after elective craniotomy. World neurosurgery. 2014 Jan; [PubMed PMID: 23182731]
Kulikov A,Tere V,Sergi PG,Bilotta F, Prevention and treatment of postoperative pain in pediatric patients undergone craniotomy: Systematic review of clinical evidence. Clinical neurology and neurosurgery. 2021 Apr 1; [PubMed PMID: 33857811]
Level 1 (high-level) evidenceCollen JF,Jackson JL,Shorr AF,Moores LK, Prevention of venous thromboembolism in neurosurgery: a metaanalysis. Chest. 2008 Aug; [PubMed PMID: 18641095]
Level 1 (high-level) evidenceStumpo V,Staartjes VE,Quddusi A,Corniola MV,Tessitore E,Schröder ML,Anderer EG,Stienen MN,Serra C,Regli L, Enhanced Recovery After Surgery strategies for elective craniotomy: a systematic review. Journal of neurosurgery. 2021 May 7; [PubMed PMID: 33962374]
Level 1 (high-level) evidenceSiegemund M,Steiner LA, Postoperative care of the neurosurgical patient. Current opinion in anaesthesiology. 2015 Oct; [PubMed PMID: 26263123]
Level 3 (low-level) evidenceCheng G,Hao S,Ye Z,Wang B,Huangpu B,Zhang P,Wang H,Hao Q, Potential risk analysis and experience summarization of unstable factors of cranial fixation devices in neurosurgical operations: three-case reports and systematic review. Chinese neurosurgical journal. 2021 Apr 28; [PubMed PMID: 33910652]
Level 3 (low-level) evidenceVaca EE,Purnell CA,Gosain AK,Alghoul MS, Postoperative temporal hollowing: Is there a surgical approach that prevents this complication? A systematic review and anatomic illustration. Journal of plastic, reconstructive [PubMed PMID: 27894915]
Level 1 (high-level) evidenceBeniwal M,Shukla D, Management of Perforator Plunge in the Transverse Sinus. Pediatric neurosurgery. 2016; [PubMed PMID: 27193189]
Lee CH,Koo HW,Han SR,Choi CY,Sohn MJ,Lee CH, Phenytoin versus levetiracetam as prophylaxis for postcraniotomy seizure in patients with no history of seizures: systematic review and meta-analysis. Journal of neurosurgery. 2019 Jun 1; [PubMed PMID: 30004278]
Level 1 (high-level) evidenceKinaci A,Algra A,Heuts S,O [PubMed PMID: 29969744]
Chughtai KA,Nemer OP,Kessler AT,Bhatt AA, Post-operative complications of craniotomy and craniectomy. Emergency radiology. 2019 Feb; [PubMed PMID: 30255407]
Schipmann S,Akalin E,Doods J,Ewelt C,Stummer W,Suero Molina E, When the Infection Hits the Wound: Matched Case-Control Study in a Neurosurgical Patient Collective Including Systematic Literature Review and Risk Factors Analysis. World neurosurgery. 2016 Nov; [PubMed PMID: 27506410]
Level 2 (mid-level) evidenceFang C,Zhu T,Zhang P,Xia L,Sun C, Risk factors of neurosurgical site infection after craniotomy: A systematic review and meta-analysis. American journal of infection control. 2017 Nov 1; [PubMed PMID: 28751035]
Level 1 (high-level) evidenceAlexandre V,Guyonaud C,Frasca D,Dahyot-Fizelier C, Major complications after scheduled craniotomy: A justification for systematic postoperative intensive care admission? European journal of anaesthesiology. 2020 Feb; [PubMed PMID: 31913939]
Level 1 (high-level) evidenceAlotaibi AF,Hulou MM,Vestal M,Alkholifi F,Asgarzadeh M,Cote DJ,Bi WL,Dunn IF,Mekary RA,Smith TR, The Efficacy of Antibacterial Prophylaxis Against the Development of Meningitis After Craniotomy: A Meta-Analysis. World neurosurgery. 2016 Jun; [PubMed PMID: 26921699]
Level 1 (high-level) evidenceReponen E,Tuominen H,Korja M, Evidence for the use of preoperative risk assessment scores in elective cranial neurosurgery: a systematic review of the literature. Anesthesia and analgesia. 2014 Aug; [PubMed PMID: 25046789]
Level 1 (high-level) evidenceBilotta F,Guerra C,Rosa G, Update on anesthesia for craniotomy. Current opinion in anaesthesiology. 2013 Oct; [PubMed PMID: 23995058]
Level 3 (low-level) evidenceEckle VS,Schneider G, [Update in neuroanesthesiology - key publications]. Der Anaesthesist. 2017 Jun; [PubMed PMID: 28386682]
Livesay S,Moser H, Evidence-based nursing review of craniectomy care. Stroke. 2014 Nov; [PubMed PMID: 25316281]