Introduction
Diabetes mellitus is a metabolic endocrine disorder due to an overall deficiency of insulin (Type 1) or defective insulin function (Type 2) which causes hyperglycemia. Type 1 diabetes which is usually seen in younger patients accounts for 5% to 10% of cases worldwide and is secondary to the autoimmune destruction of insulin-producing B-islet cells of the pancreas which results in complete insulin deficiency. Type 2 diabetes accounts for 90% to 95% of cases worldwide and is due to genetic and environmental factors with resultant insulin resistance and pancreatic beta-cell dysfunction causing relative insulin deficiency. This form of diabetes remains clinically inevident for many years. Although abnormal glucose metabolism which is associated with chronic hyperglycemia results in complications that can either be macrovascular or microvascular. The macrovascular disease affects mainly the cardiovascular and cerebrovascular systems, and the microvascular disease includes nephropathy, retinopathy, and neuropathies.
A debilitating complication of diabetes mellitus is diabetic ulcers, which leads to increased overall morbidity in patients. This complication may be prevented, as the inciting factor is most often minor trauma. Early identification of these cutaneous injuries also can lead to improved outcomes while decreasing the risk of progression. Patients with diabetes mellitus (type 1 or 2) have a total lifetime risk of a diabetic foot ulcer complication as high as 25%. [1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The Six Stages of a Diabetic Foot as described by the 7th Practical Diabetes International Foot Conference
- Stage 1 - Normal foot with no risk factors;
- Stage 2 - High-risk foot
- Stage 3 - Ulcerated foot
- Stage 4 - Cellulitic foot
- Stage 5 - Necrotic foot
- Stage 6 - Foot that cannot be rescued
There are three types of diabetic foot ulcer described namely neuropathic, neuroischaemic, and ischaemic.[2] [3] Sensory neuropathy leads to the majority of ulcers as a result of minor trauma which is not perceived by the patient and further goes untreated as there are no associated pain symptoms unless there is a routine evaluation to assist in identification. [4] Myocardial infarction is one of the most significant events related to peripheral arterial disease increased risk of ischemia. However, ischemia leading to diabetic ulcers adds severe morbidity and health care cost as it can be a chronic complication which is difficult to treat as there is insufficient blood supply.
Major Risk Factors [5]
- Peripheral motor neuropathy: Abnormal foot anatomy and biomechanics, with clawing of toes, high arch, and subluxed metatarsophalangeal joints, leading to excess pressure, callus formation, and ulcers
- Peripheral sensory neuropathy: Lack of protective sensation, leading to unattended minor injuries caused by excess pressure or mechanical or thermal injury
- Peripheral autonomic neuropathy: Deficient sweating leading to dry, cracking skin
- Neuro-osteoarthropathy deformities (i.e., Charcot disease) or limited joint mobility
- Abnormal anatomy and biomechanics, leading to excess pressure, especially in the midplantar area
- Vascular (arterial) insufficiency: Impaired tissue viability, wound healing, and delivery of neutrophils
- Hyperglycemia and other metabolic derangements: Impaired immunological (especially neutrophil) function and wound healing and excess collagen cross-linking
Epidemiology
The pooled worldwide prevalence of diabetic foot ulceration was 6.3%. North America had the highest prevalence of 13%; Oceania had the lowest prevalence of 3%. The prevalence in Africa was 7.2% which was higher than Asia 5.5%. Diabetic foot ulceration was more prevalent in male patients with diabetes mellitus, 4.5%, than female patients, 3.5%. Patients with type 2 diabetes mellitus (T2DM) had a higher prevalence of ulceration at 6.4% compared to patients with type 1 diabetes mellitus (T1DM), 5.5%. [6][7]
In a systematic review and meta-analysis by Zhang et al. published in 2016, patients with diabetic foot ulceration had the following characteristics: older age (61.7 plus or minus 3.7 versus 56.1 plus or minus 3.9), longer diabetic duration (11.3 plus or minus 2.5 versus 7.4 plus or minus 2.2), lower body mass Index (BMI, 23.8 ± 1.7 versus 24.4 plus or minus 1.7), higher percentage of smokers (29.1%, 95%CI: 18.3% to 39.8% versus 17.4%, 95% CI: 12.4% to 22.4%), hypertension (63.4%, 95%CI: 49.4% to 88.3% versus 53.1%, 95%CI: 33.8% to 72.5%), and diabetic retinopathy (63.6%, 95%CI: 38.8% to 88.3%% versus 33.3%, 95%CI: 13.8% to 52.7%) than patients that did not develop diabetic foot ulceration.
Pathophysiology
Atherosclerosis and diabetic peripheral neuropathy are the two main causes leading to a complication of diabetes such as ulcers. Atherosclerosis leads to decreased blood flow in large and medium-sized vessels secondary to thickening of capillary basement membrane, loss of elasticity, and deposition of lipids within the walls. Further arteriosclerosis leads to small vessel ischemia. Peripheral neuropathy affects the sensory, motor, and autonomic nervous system. There are multifactorial causes such as vascular disease occluding the vasa nervorum, endothelial dysfunction, chronic hyperosmolarity, and effects of increased sorbitol and fructose.
History and Physical
The evaluation of patients presenting with diabetic ulcers can be divided into a clinical and radiologic assessment.
A clinically pertinent history of the type of diabetes, medication history, comorbidities, symptoms of peripheral neuropathy, and vascular insufficiency should be elucidated. Symptoms of neuropathy include hypoesthesia, hyperesthesia, paresthesia, dysesthesia, and radicular pain. Vascular insufficiency has varying presentations and most patients are asymptomatic. However, they can present with intermittent claudication, rest pain, and healing or non-healing ulcers.
In the examination of the legs and foot, an inspection should be performed in a well-lit room with appropriate exposure. Proper documentation using descriptions of ulcer characteristics with size, depth, appearance, and location performed. Presence of discoloration, necrosis, or areas of drainage are signs of infection, and further care is required. Other abnormalities such as nail discoloration, callus formation, and deformities should be noted. Imbalance in the innervations of the foot muscles from neuropathic damage can lead to the development of common deformities seen in affected patients. Hyperextension of the metatarsal-phalangeal joint with interphalangeal or distal phalangeal joint flexion leads to hammer toe and claw toe deformities, respectively. Charcot arthropathy is a commonly seen deformity. Assessment of footwear is important as it can be a contributing factor to the development of foot ulceration. The presence of callus or nail abnormalities should be noted.
Examine the cardiovascular system, checking popliteal, posterior tibial, and dorsalis pedis pulse. Claudication, loss of hair, and the presence of pale, thin, shiny, or cool skin are physical findings suggestive of potential ischemia. If a vascular disease is a concern, the evaluator should measure the ankle-brachial index (ABI). ABIs can, however, be falsely elevated in patients with diabetes mellitus due to calcification of vessels. More reliable methods of assessing the potential for healing foot ulcers in patients with diabetes mellitus suspected of having peripheral ischemia involve systolic toe pressure measurements by photoplethysmography or measurement of distal transcutaneous oxygen tension.
Evaluation
Based on wound depth and necrotic tissue, diabetic ulcers can be classified by the Wagner ulcer classification system. [8][9][10]
Wagner-Meggitt Classification of Diabetic Foot
- Grade 0 - Foot symptoms like pain, only
- Grade 1 - Superficial ulcers involving skin and subcutaneous tissue
- Grade 2 - Deep ulcers involving ligaments, muscles, tendons, etc
- Grade 3 - Ulcer with bone involvement
- Grade 4 - Forefoot gangrene
- Grade 5 - Full-foot gangrene
CBC
Serum Inflammatory Markers
X-Ray/Ultrasound: Performed for the detection of the spread of the lesion and soft tissue involvement.
MRI: Radiologic evaluation involves plain radiographs in two-thirds of the views assessing for deformity.If there is suspicion of osteomyelitis, tendonitis, or joint inflammation MRI imaging should be performed.
Probe-to-bone Test
Monofilament Test
Bone Scan: Can identify the involvement of deep wounds.
Biopsy and Culture: Specimen of bone and other tissue involved and histopathological examination is performed with the culture. This can also guide antibiotic treatment in case of a bacterial infection.
Treatment / Management
Multimodal Diabetic Ulcer Management[11][12]
- Patient Education: Education on foot care, as well as control of blood sugar levels, should be performed early. This can also be done with the aid of diabetic educators and social workers.
- Blood-Sugar Control: This is managed using a team approach of primary care physician, podiatry, and vascular specialist and based on the severity of the disease and the patient’s attitude toward medication, especially insulin.
- Decreasing Pressure, preventing further or new trauma: Offloading pressure to the area can be done with crutches, wheelchairs, and casting. Ulcer healing is improved with total contact casting, irremovable cast walkers compared to removable cast walkers. [13]
- Improve Peripheral Vascular Circulation: Antiplatelet agents are the initial drug therapy; however, insufficiency requires surgical bypass.
- Prevent or Control Infection: Systemic and source control is achieved using antibiotics and surgical debridement.
- Topical Ulcer Care: Principles of wound care include the use of topical agents with dressing and debridement. Shallow ulcers can be managed with occlusive and semi-occlusive dressings. A specialized dressing containing hyaluronic acid, collagen, and surgical intervention for debridement is usually required in full-thickness ulcers.
Differential Diagnosis
- Venous Ulcers: It is caused by chronic elevation of venous pressure leading to incompetent valves. Venous blood from deep veins refluxes into superficial veins causing varicose veins and lower limb edema.Leakage of plasma proteins and leukocytes causing edema and free radical damage to the tissue resulting in ulcer formation. The most common locations are the pretibial area and above the medial malleolus. Usually, a shallow ulcer with irregular borders and overlying fibrinous exudate is present.
- Diabetic Dermatopathy: These are purplish, round asymptomatic lesions that usually occur in the lower extremities but can be present anywhere on the body of diabetic patients. These lesions usually require no intervention.
- Malignancy:- Different malignancies can present as cutaneous ulcers but systemic signs and symptoms ( fever, weight loss, malaise, etc) are also usually present. The diagnosis can be confirmed by microscopic examination of the biopsy specimen.
- Superficial Thrombophlebitis: Characterized by pain, erythema, tenderness overlying inflamed and thrombosed superficial veins.
- Leukocytoclastic Vasculitis: Inflammation of blood vessels and surrounding tissues caused by the deposition of immune complexes.
- Gouty Arthritis: Monosodium urate crystal deposits in joints can result in inflammation, usually associated with hyperuricemia.
- Infection: Primary infectious ulcer results either by direct inoculation or systemic spread. Clinical features vary with the types of infection.
- Sickle Cell Disease: Sickle cell disease can result in painful leg ulcers commonly on medial and lateral malleoli.
- Drugs:-Some drugs e.g, warfarin, heparin, hydroxyurea can result in ulcer formation.
Prognosis
The prognosis of diabetic ulcers is dependant on various factors such as strict diabetes control, patient education, a healthy lifestyle, and proper wound care. Poor blood supply, infection, prolonged duration, and recurrent ulcers are associated with poor prognosis. These prognostic indicators are utilized to take necessary interventions and precautionary measures to reduce the risk of severe complications such as osteomyelitis and amputation.[14][15]
Complications
Diabetic ulcers can lead to many complications and are responsible for hospitalizations and functional disabilities in diabetic patients.[16]
Postoperative and Rehabilitation Care
Proper debridement, wound irrigation and dressing care are necessary for the prevention of infection and healing. Off-loading in patients with diabetic foot ulcers by total contact casts and postoperative shoes is an effective measure for promoting wound healing. In diabetic patients, postoperative care is of even greater importance in the presence of various risk factors such as impaired mobility, decreased perfusion, malnutrition, and reduced sensation.[19]
Consultations
Early detection and treatment can help in decreasing complications. Timely interventions and consultations with the following are recommended:[20]
- Endocrinologist
- Infectious disease specialist
- Vascular surgeon
- Podiatrist
- Orthopedic surgeon
- Plastic surgeon
Deterrence and Patient Education
Patient education about the proper care of wounds and the risk of recurrence is necessary to improve the quality of life of the patients. Reducing hospital visits and increasing the ulcer-free duration is the goal. Long term surveillance and information sharing can maximize the results of the care provided. Sharing articles written in plain and easy to understand language is the key to successful communication. Health care providers should be encouraged to provide necessary information available on various platforms.[21]
Pearls and Other Issues
Diabetes can lead to serious complications if they are not identified and managed adequately. Diabetic ulcers are a common complication of uncontrolled diabetes. The frequency of these complications can be lowered by controlling blood glucose, self-examination of feet, and regular check-ups by doctors.
The following are some risk factors associated with diabetic foot ulcers:-
- Abnormality of foot anatomy(e.g Charcot arthropathy)
- Poor blood circulation(e.g weak pulse, cold skin, or blue skin)
- Abnormality of peripheral sensations(e.g inability to sense pain in diabetic neuropathy)
- Smoking can reduce circulation to the feet.
Different measures can be taken to reduce the risk of foot problems. In general, keeping blood glucose in the target range reduces all kinds of diabetic complications. This involves making a healthy diet and lifestyle changes. Avoiding activities associated with foot injuries and avoiding smoking can be helpful. Caring for nails and trimming them straight across to avoid skin injury. Washing feet and choosing socks and shoes wisely. Regular foot exams to avoid unnoticed injuries.[22]
Enhancing Healthcare Team Outcomes
The management of a diabetic ulcer is very difficult and is best done with a team that includes an endocrinologist, surgeon, wound care nurse, internist, physical therapist, vascular surgeon, an infectious disease expert, and dietitian. Besides ensuring that glucose levels are controlled, one has to ensure that the tissue has an adequate blood supply. All diabetics should be urged to stop smoking and resume an exercise program. Close follow up is required by an interprofessional team as these ulcers can rapidly lead to necrosis and loss of a digit or a limb. Diabetic ulcers and wounds should be evaluated by a standardized and evidence-based approach. Well established communication and coordination among the health providers can significantly decrease complications such as amputation.[23][24]
Media
(Click Image to Enlarge)

Diabetic Ulcer Due to neuropathy, vasculopathy, and foot deformity. Note periwound callous formation. Wagner Grade 2 Contributed by Mark A. Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Diabetic Foot Ulcer. Neuropathic ulceration in a patient with diabetes. Note periwound callous formation. Wagner Grade 2.
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)
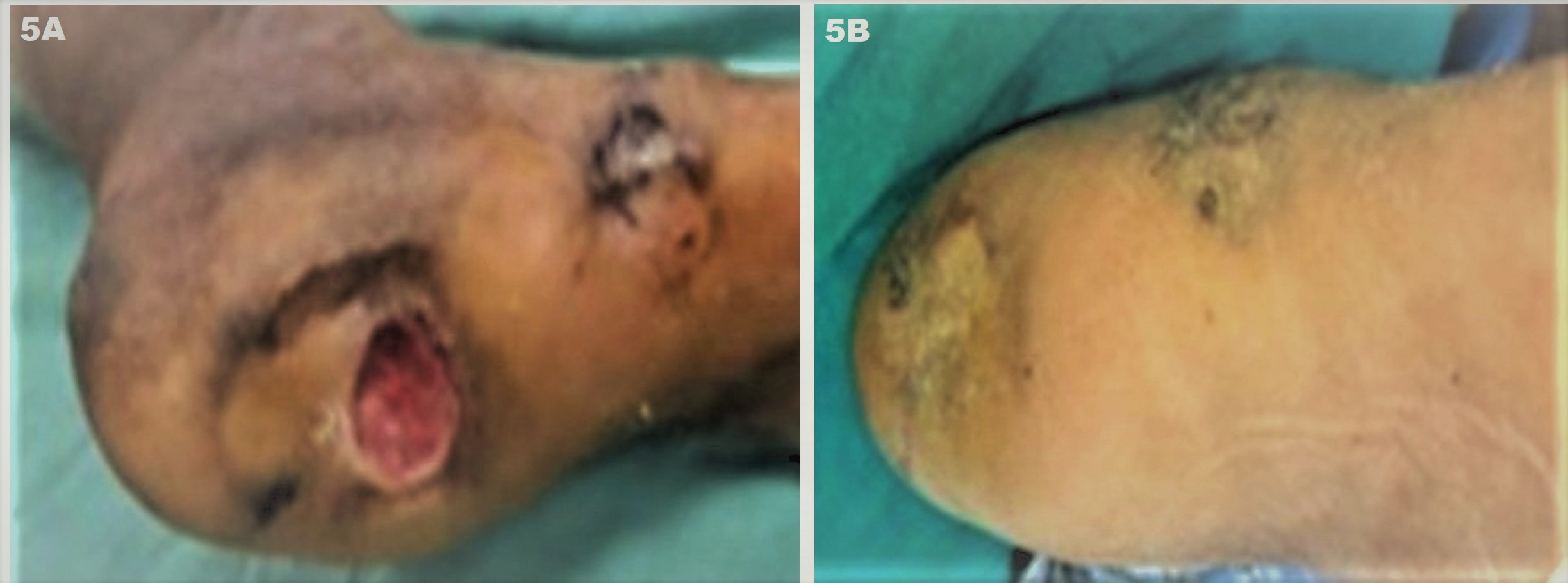
Jodhpur Technique. Depiction of success of the technique in a non-healing foot ulcer of a patient with diabetes with diabetic foot (diabetes controlled with HbA1C < 6.5 X one year). (A) Baseline multiple ulcers over the foot involving the heel and medial malleolus (pressure sites). The lesions are chronic non-healing ulcers (CNHUs) as they failed to heal despite multiple treatment sessions using collagen dressings, platelet-rich fibrin matrix (PRFM), hyperbaric oxygen as well as one flap transplant that necrosed within 4 weeks; and (B) Complete healing of ulcers can be appreciated after 3 months of 2 sessions of JT performed 1 month apart.
Contributed by D Kachhawa, MD, and S Sonthalia, MD, DNB, MNAMS
References
Boulton AJ, Armstrong DG, Albert SF, Frykberg RG, Hellman R, Kirkman MS, Lavery LA, LeMaster JW, Mills JL Sr, Mueller MJ, Sheehan P, Wukich DK. Comprehensive foot examination and risk assessment. A report of the Task Force of the Foot Care Interest Group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Physical therapy. 2008 Nov:88(11):1436-43 [PubMed PMID: 19137633]
Edmonds M, Bates M, Doxford M, Gough A, Foster A. New treatments in ulcer healing and wound infection. Diabetes/metabolism research and reviews. 2000 Sep-Oct:16 Suppl 1():S51-4 [PubMed PMID: 11054889]
McNeely MJ, Boyko EJ, Ahroni JH, Stensel VL, Reiber GE, Smith DG, Pecoraro RF. The independent contributions of diabetic neuropathy and vasculopathy in foot ulceration. How great are the risks? Diabetes care. 1995 Feb:18(2):216-9 [PubMed PMID: 7729300]
Level 2 (mid-level) evidenceUçkay I, Aragón-Sánchez J, Lew D, Lipsky BA. Diabetic foot infections: what have we learned in the last 30 years? International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2015 Nov:40():81-91. doi: 10.1016/j.ijid.2015.09.023. Epub 2015 Oct 13 [PubMed PMID: 26460089]
Gariani K, Uçkay I, Lipsky BA. Managing diabetic foot infections: a review of the new guidelines. Acta chirurgica Belgica. 2014 Jan-Feb:114(1):7-16 [PubMed PMID: 24720132]
Level 1 (high-level) evidenceGeraghty T, LaPorta G. Current health and economic burden of chronic diabetic osteomyelitis. Expert review of pharmacoeconomics & outcomes research. 2019 Jun:19(3):279-286. doi: 10.1080/14737167.2019.1567337. Epub 2019 Jan 21 [PubMed PMID: 30625012]
Zhang X, Sun D, Jiang GC. Comparative efficacy of nine different dressings in healing diabetic foot ulcer: A Bayesian network analysis. Journal of diabetes. 2019 Jun:11(6):418-426. doi: 10.1111/1753-0407.12871. Epub 2018 Nov 25 [PubMed PMID: 30324760]
Level 2 (mid-level) evidenceLevy N, Gillibrand W. Management of diabetic foot ulcers in the community: an update. British journal of community nursing. 2019 Mar 1:24(Sup3):S14-S19. doi: 10.12968/bjcn.2019.24.Sup3.S14. Epub [PubMed PMID: 30817189]
Bolton L. Managing Patients With Diabetic Foot Ulcers. Wounds : a compendium of clinical research and practice. 2018 Dec:30(12):380-381 [PubMed PMID: 30507549]
Parker CN, Shuter P, Maresco-Pennisi D, Sargent J, Collins L, Edwards HE, Finlayson KJ. Implementation of the Champions for Skin Integrity model to improve leg and foot ulcer care in the primary healthcare setting. Journal of clinical nursing. 2019 Jul:28(13-14):2517-2525. doi: 10.1111/jocn.14826. Epub 2019 Mar 24 [PubMed PMID: 30791154]
Borys S, Hohendorff J, Frankfurter C, Kiec-Wilk B, Malecki MT. Negative pressure wound therapy use in diabetic foot syndrome-from mechanisms of action to clinical practice. European journal of clinical investigation. 2019 Apr:49(4):e13067. doi: 10.1111/eci.13067. Epub 2019 Jan 29 [PubMed PMID: 30600541]
Giacomozzi C, Sartor CD, Telles R, Uccioli L, Sacco ICN. Ulcer-risk classification and plantar pressure distribution in patients with diabetic polyneuropathy: exploring the factors that can lead to foot ulceration. Annali dell'Istituto superiore di sanita. 2018 Oct-Dec:54(4):284-293. doi: 10.4415/ANN_18_04_04. Epub [PubMed PMID: 30575564]
American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes care. 2018 Jan:41(Suppl 1):S13-S27. doi: 10.2337/dc18-S002. Epub [PubMed PMID: 29222373]
Ndosi M, Wright-Hughes A, Brown S, Backhouse M, Lipsky BA, Bhogal M, Reynolds C, Vowden P, Jude EB, Nixon J, Nelson EA. Prognosis of the infected diabetic foot ulcer: a 12-month prospective observational study. Diabetic medicine : a journal of the British Diabetic Association. 2018 Jan:35(1):78-88. doi: 10.1111/dme.13537. Epub 2017 Nov 20 [PubMed PMID: 29083500]
Level 2 (mid-level) evidenceApelqvist J, Larsson J, Agardh CD. Long-term prognosis for diabetic patients with foot ulcers. Journal of internal medicine. 1993 Jun:233(6):485-91 [PubMed PMID: 8501419]
Muduli IC, P P A, Panda C, Behera NC. Diabetic Foot Ulcer Complications and Its Management-a Medical College-Based Descriptive Study in Odisha, an Eastern State of India. The Indian journal of surgery. 2015 Dec:77(Suppl 2):270-4. doi: 10.1007/s12262-012-0791-2. Epub 2013 Mar 9 [PubMed PMID: 26730008]
Boulton AJ. Diabetic neuropathy and foot complications. Handbook of clinical neurology. 2014:126():97-107. doi: 10.1016/B978-0-444-53480-4.00008-4. Epub [PubMed PMID: 25410217]
Level 3 (low-level) evidenceMegallaa MH, Ismail AA, Zeitoun MH, Khalifa MS. Association of diabetic foot ulcers with chronic vascular diabetic complications in patients with type 2 diabetes. Diabetes & metabolic syndrome. 2019 Mar-Apr:13(2):1287-1292. doi: 10.1016/j.dsx.2019.01.048. Epub 2019 Jan 24 [PubMed PMID: 31336479]
Lázaro-Martínez JL, Aragón-Sánchez J, García-Morales E. Antibiotics versus conservative surgery for treating diabetic foot osteomyelitis: a randomized comparative trial. Diabetes care. 2014:37(3):789-95. doi: 10.2337/dc13-1526. Epub 2013 Oct 15 [PubMed PMID: 24130347]
Level 1 (high-level) evidenceAmmendola M, Sacco R, Butrico L, Sammarco G, de Franciscis S, Serra R. The care of transmetatarsal amputation in diabetic foot gangrene. International wound journal. 2017 Feb:14(1):9-15. doi: 10.1111/iwj.12682. Epub 2016 Oct 3 [PubMed PMID: 27696694]
Dorresteijn JA, Kriegsman DM, Assendelft WJ, Valk GD. Patient education for preventing diabetic foot ulceration. The Cochrane database of systematic reviews. 2014 Dec 16:2014(12):CD001488. doi: 10.1002/14651858.CD001488.pub5. Epub 2014 Dec 16 [PubMed PMID: 25514250]
Level 1 (high-level) evidenceNather A, Cao S, Chen JLW, Low AY. Prevention of diabetic foot complications. Singapore medical journal. 2018 Jun:59(6):291-294. doi: 10.11622/smedj.2018069. Epub [PubMed PMID: 29974120]
Xiang J, Wang S, He Y, Xu L, Zhang S, Tang Z. Reasonable Glycemic Control Would Help Wound Healing During the Treatment of Diabetic Foot Ulcers. Diabetes therapy : research, treatment and education of diabetes and related disorders. 2019 Feb:10(1):95-105. doi: 10.1007/s13300-018-0536-8. Epub 2018 Nov 21 [PubMed PMID: 30465160]
Lim JZ, Ng NS, Thomas C. Prevention and treatment of diabetic foot ulcers. Journal of the Royal Society of Medicine. 2017 Mar:110(3):104-109. doi: 10.1177/0141076816688346. Epub 2017 Jan 24 [PubMed PMID: 28116957]