Introduction
Diarrhea consists of the passage of watery and loose stools multiple times a day (usually more than 3), though specific definitions may vary when applied for distinct studies or populations.[1][2] Diarrhea is among the most common medical conditions, and mild occurrences may not require medical attention. For health care providers, it is crucial to be familiar with this entity regardless of specialty and scope of practice.[3]
Bacterial diarrhea, in specific, is a more severe condition with increased severity of symptoms. It is important to be familiar with this pathology and differentiate it from other, less severe, causes of diarrhea. Clinical decision making includes determining the appropriate use of diagnostic stool testing and determining when to treat with antibiotics, both of which are necessary with bacterial diarrhea. Most of the cases of bacterial diarrhea in the United States (U.S.) are foodborne.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Diarrhea can be acute or chronic: acute is defined as lasting less than two weeks, chronic lasts more than a month, between 2 to 4 weeks is dubbed persistent.
Chronic diarrhea may reflect a functional issue as in cases of irritable bowel syndrome. Still, chronic diseases, including inflammatory bowel disease (IBD), malabsorption, and medication side effects, can be other etiologies. Chronic diarrhea is more often non-infectious, although chronic infections produce it as well. Bacterial infection with Clostridiodes difficile can result in chronic diarrhea, as can protozoa such as Giardia, Entamoeba, Cryptosporidium, or Isospora. Patients at increased risk of chronic diarrhea from these organisms include young children, the elderly, immune-compromised, or international travelers.
Acute diarrhea usually has an infectious etiology. Most of the episodes of acute diarrhea are viral, with common pathogens including norovirus, rotavirus, or adenovirus. Rehydration is the mainstay of treatment, especially in children who have increased morbidity and mortality. In developing countries, diarrhea is a major cause of mortality in young children, and prompt treatment with oral rehydration solutions (ORS) replaces water and electrolytes lost during diarrheal episodes, significantly reducing morbidity and mortality.[5]
Bacterial diarrhea can produce more severe forms of acute diarrhea. Dysentery is diarrhea associated with blood (plus or minus mucus) and represents more invasive infection. The most frequently identified organisms causing bacterial diarrhea are Escherichia coli (most common worldwide), Shigella, Salmonella, Campylobacter (most common in children), Yersinia, and Clostridium spp.
Traveler's diarrhea can be most commonly the result of Shiga-toxin producing E. coli (STEC), as well as Shigella, Salmonella, Entamoeba histolytic, Giardia, Cryptosporidium, Cyclospora, and enteric viruses.
Epidemiology
There are 1.7 billion cases of childhood diarrhea every year, and diarrhea is the second leading cause of mortality in children under five years old, with about 525,000 childhood deaths annually. Most of this mortality is preventable through access to care and rehydration therapy. Complications such as ensuing malabsorption can be seen that impact child growth after recovery from the immediate illness. There are an estimated 5.2 million cases of bacterial diarrhea in the U.S. annually, with 80% of infections resulting from foodborne contamination.[6]
Global estimates for the prevalence of specific types of bacterial diarrhea among all diarrheal causes include E.coli 10% to 25%, Shigella 10%, Salmonella 3%, Campylobacter 3 to 6%.[7][8] and bacterial diarrhea in the U.S. was estimated to be approximately 31% of all diarrheas.[9] The proportion of bacterial pathogens resulting in foodborne diarrheal illness in the U.S. is estimated to be: Salmonella 15.4%, Campylobacter 11.8%, Shigella 4.6 %, Shiga-toxin producing E. coli (STEC) around 3%.[10]
Pathophysiology
In bacterial diarrhea, the pathogen attaches to the epithelium and produce toxins that increase the intracellular cyclic-AMP (adenosine monophosphate), a secondary messenger. This ultimately revs up the secretory process in the enterocytes. The toxins may also provoke the release of cytokines responsible for chemotaxis and production of eicosanoids (prostaglandins), worsening the intra-luminal unbalance of water. This excess of water and electrolytes in the intestinal lumen draws more fluid into the lumen, further worsening diarrhea with this osmotic effect.[11]
History and Physical
A history of food intake can help with the diagnosis of foodborne illness, and timing of illness onset after food intake may aid in determining food sources of greatest concern for contamination. Travel history can impact the consideration of additional pathogens and potentially broaden the differential diagnostic considerations.[12] Questions about the job, hobbies, pets, and residential status are all important. Medication use should be documented and carefully reviewed. Almost all medications can have a side effect of diarrhea, and it can be of concern, especially during the initial phases of using new medicine. Some that are more likely to cause diarrhea are antacids, magnesium, laxatives, nonsteroidal inflammatory drugs (NSAIDs), antibiotics, chemotherapy agents, and metformin. The use of antibiotics predisposes to Clostridiodes difficile associated diarrhea.
The number, consistency, volume, and other characteristics of the stool should be determined. The diagnostician should seek associated symptoms. Small intestinal diarrhea is usually voluminous, watery, and comes with abdominal discomfort, bloating, and pain. Large intestinal diarrhea is less voluminous and comes with painful bowel movements and minimal abdominal discomfort. E.coli (toxicogenic - STEC), Salmonella spp., Vibrio cholerae, Clostridium perfringens affect the small bowel, whereas Campylobacter, Shigella, Yersinia, E. coli (enteroinvasive) primarily involve the colon.[13][14][3]
Fever, blood, and mucus in the stool are usually concerning symptoms and are a sign of enteroinvasive disease in the colon. When there is clear red blood in the stool, chances of presence of STEC will increase. STEC starts with watery diarrhea that will turn bloody in 1 to 5 days. Severe cramping is usually present, and diarrhea is more than five times a day. STEC is the most common reason for renal failure and hemolytic uremic syndrome in children.
General medical history is essential. Underlying immunosuppressed or compromised states (cancer, transplant, HIV,etc.) can increase the risk of specific pathogens or increase the severity of illness. Certain medical conditions are associated with certain organisms (i.e., cirrhosis with Vibrio, hemochromatosis with Yersinia, pregnancy with Listeria).
Reheated fried rice is associated with Bacillus cereus infection, raw beef like a hamburger is associated with STEC, raw milk can harbor Salmonella, and Campylobacter, seafood such as shellfish can have contamination with Vibrio cholerae or V. parahemolyticus, undercooked pork is associated with diarrhea from Yersinia spp.
Persons with human immunodeficiency virus (HIV) have an increased risk of diarrhea caused by Cryptosporidium, Microspora, Isospora, or Cytomegalovirus. Listeriosis is associated with immune suppression as well as with pregnancy.
Certain medications can cause diarrhea: antibiotics, laxatives, antiacids, colchicine, and chemotherapy regimen have all been implicated. Microscopic colitis or radiation colitis can also be a problem.
General physical examination with a focus on vital signs and signs of hypovolemia is of importance. The abdominal exam should evaluate for distension, tenderness, presence of normal bowel sounds or ileus, and clinical evidence of peritonitis.
Clostridiodes difficile infection usually presents with watery diarrhea, nausea, fever, anorexia in the setting of recent antibiotic use. Antibiotic use can be up to 10 weeks before the symptom onset. Although any antibiotic can cause this, the most frequently associated are fluoroquinolones, penicillins, and clindamycin. Very low potassium levels can also present in this entity.
Salmonella infection is usually associated with poultry, eggs, and milk. The enteric fever version results from S. typhi and S. paratyphi. It presents as a febrile illness with abdominal pain, fever, bradycardia, pulse-temperature disassociation, rose spots, hepatosplenomegaly, anemia, and leukopenia. Diarrheal illness is usually from non-typhoidal types, which are commonly isolated from the diarrheal stool. They are typically self-limited courses of diarrhea, fever, cramps, and nausea. No antibiotics are recommended ordinarily for non-typhoidal unless the host is immunocompromised.
Shigellosis presents with abdominal cramps, high fever, bloody mucosal diarrhea, tenesmus, leukemoid reaction, and lasts for up to seven days. It is usually self-limited, but complications can be reactive arthritis, seizure, hemolytic-uremic syndrome, rectal prolapse, toxic megacolon, obstruction, and perforation.
Yersiniosis presents with abdominal pain in the right lower quadrant, fever, vomiting, diarrhea, leukocytosis, and can be easily mistaken for appendicitis. "Epidemic appendicitis" describes the sudden appearance of many cases of appendicitis-like patients that is secondary to a yersinia epidemic.
Evaluation
Although most patients with diarrhea will not require any laboratory evaluations, tests are a recommended step after several days have passed with no resolution of symptoms or if the initial treatments were unsuccessful. If the disease is severe, refractory, or affecting high-risk patients, testing may merit more urgent consideration.
Stool studies should preferably take place using a fresh diarrheal stool. The presence of white blood cells (fecal leukocytes) might be a sign of inflammation, although the sensitivity is 70 percent and specificity only 50 percent.[15] Fecal calprotectin is a potential marker of neutrophil activity and can differentiate inflammatory from non-inflammatory diarrhea. Sensitivity and specificity in the 90% range have been proposed for this test.[16] Fecal lactoferrin is another potential marker of neutrophils and might be of help in differentiating infectious diarrhea from inflammatory bowel disease (IBD).[17] Red blood cells will indicate enteroinvasive disease that is causing bleeding. Ova and parasite recognition will confirm these sources of infection. Quantitative stool fat shows an abnormal gastrointestinal mucosa and can help differentiate malabsorption syndromes.[18]
Multi-pathogen molecular panels that identify the genetic material of the organisms can be helpful and may identify the source of infection within hours rather than days for standard culture techniques.[19] Bacterial stool cultures may be indicated to confirm specific bacterial pathogens or to aid in determining antimicrobial susceptibility patterns to guide treatment.
For C. difficile diagnosis, nucleic acid amplification is a process for diagnosis confirmation. Initial screening usually involves stool tests for C. difficile toxin and glutamate dehydrogenase (GDH) antigen. The presence of pseudomembranous colitis either in imaging or endoscopy is also beneficial.
Treatment / Management
Rehydration is the mainstay of treatment of bacterial diarrhea. This strategy is possible through the administration of oral or intravenous fluids. The use of ORS containing sodium, potassium, and glucose delivered in small, frequent volumes is the recommendation in patients who can tolerate this intake, and intravenous (IV) rehydration reserved for those that fail oral rehydration.
All patients should be encouraged to eat nutrient-rich foods to counter diarrhea as soon as dehydration is adequately managed; rather than restrict dietary intake. Breast-fed infants should continue their usual feedings if possible. Zinc supplementation is reported to reduce both the stool volume and stool frequency by 30 percent and is a consideration in severe cases.[20] Although diets such as BRAT (banana, rice, apple, and toast) or bland diet have been proposed to improve the condition and are somewhat better tolerated; no reliable data or prospective studies are available to confirm this, and the assumptions are mostly based on limited studies or personal experiences. Similarly, the exclusion of certain foods, such as dairy products, is not evidence-based. A systematic review suggested that there is little evidence for or against dietary restrictions in diarrhea, and a typical diet can be resumed as tolerated.[21](A1)
Avoid symptomatic treatment with antimotility agents, as their use decreases peristalsis and prolongs the presence of bacteria and toxins in the gut, therefore potentially worsening the disease. Treatment with antimotility agents and reduction of stool volume does not alleviate the need for supportive rehydration.[22](A1)
Some patients with bacterial diarrhea will need antibiotic therapy.[23] When bacterial diarrhea is suspected, the patient is toxic appearing, dysentery is present, or the patient is immunocompromised; empiric antibiotic treatment may be indicated.[2] Whenever local antimicrobial susceptibility data are available, they should guide empiric treatment, and patient stool pathogen results should be used to guide definitive therapy. (A1)
Lactobacillus GG and Saccharomyces boulardii and other probiotics might be used in infectious diarrhea and traveler's diarrhea, although the effects are modest at best.[24] The exact type, dosage, and duration of treatment are also not known. (A1)
Admission is necessary in dehydration, shock, severe nausea and vomiting, the need for intravenous antibiotics, the possibility of complications, and on a case by case basis. Scoring systems have been proposed to facilitate recognizing those with severe diarrhea based on temperature, arterial pressure, white blood cell count, and stool white cells.[25] (B2)
Vaccination for specific travelers against cholera and typhoid may be recommended, based upon the travel destination and country of origin. Vaccination is also available against rotavirus in infants.
Differential Diagnosis
Bacterial diarrhea is part of the differential diagnosis for systemic illness with acute onset of diarrhea, including the following:
- Viral systemic diseases including viral gastroenteritis, or multi-system viral infections including adenovirus, and influenza merit consideration.
- Protozoal diarrhea, such as Giardia or Cryptosporidium, can also present similarly. In endemic areas, consideration of arboviral syndromes or malaria may also be necessary.[26]
Non-infectious causes should also be excluded, such as
Prognosis
Prognosis is usually excellent in developed countries with appropriate support, hydration, and antibiotics. In developing areas where access to care may limit opportunities for rehydration, morbidity, and mortality are increased, particularly for vulnerable populations.
Complications
Toxic megacolon, gastrointestinal perforation, reactive arthritis, persistent diarrhea, bacteremia and sepsis, hemolytic-uremic syndrome, Guillain-Barre syndrome are all possible complications of this disease, based upon the causative bacterial pathogen.
Deterrence and Patient Education
The World Health Organization (WHO) promotes national policies and invests in diarrhea treatment and control in developing countries. In developed countries, this takes place through local and federal health care agencies. Such organizations have a paramount role in educating the general population and populations at risk. They will help train health care providers and develop region-specific programs to curb the spread of bacterial diarrhea.
Enhancing Healthcare Team Outcomes
Bacterial diarrhea treatment is best via an interprofessional team paradigm. An epidemiologist will study, analyze, and teach infection causes and patterns. Local health authorities will use such information for screening, management, and public awareness. Primary care providers and physician extenders will encounter such cases first and focus on the treatment for dehydration and upholding the hygienic principles that will help prevent the spread of the disease. For severe illness, including hospitalized patients, infectious disease specialists, and gastroenterologists will be an integral part of the team. Nurses have a significant role in team patient care, including the education of the patients, and increasing the awareness of the causes and treatment of bacterial diarrhea. Patients should receive education on appropriate ways to deal with diarrhea and specifically bacterial diarrhea. An infectious disease board-certified pharmacist should also consult on the case, providing optimal antimicrobial regimen recommendations. Hydration and continuation of oral intake of water and food are essential. ORS should be utilized to maintain hydration. General hygienic principals, including using clean water for drinking, bathing, and cleaning items used for food storage as well as appropriate hand hygiene after stooling, will help prevent infections. Close communication between the primary care providers and the infectious disease expert, as well as the involvement of all members of the interprofessional team, can hopefully lead to better outcomes.[30] [Level 5]
Media
(Click Image to Enlarge)
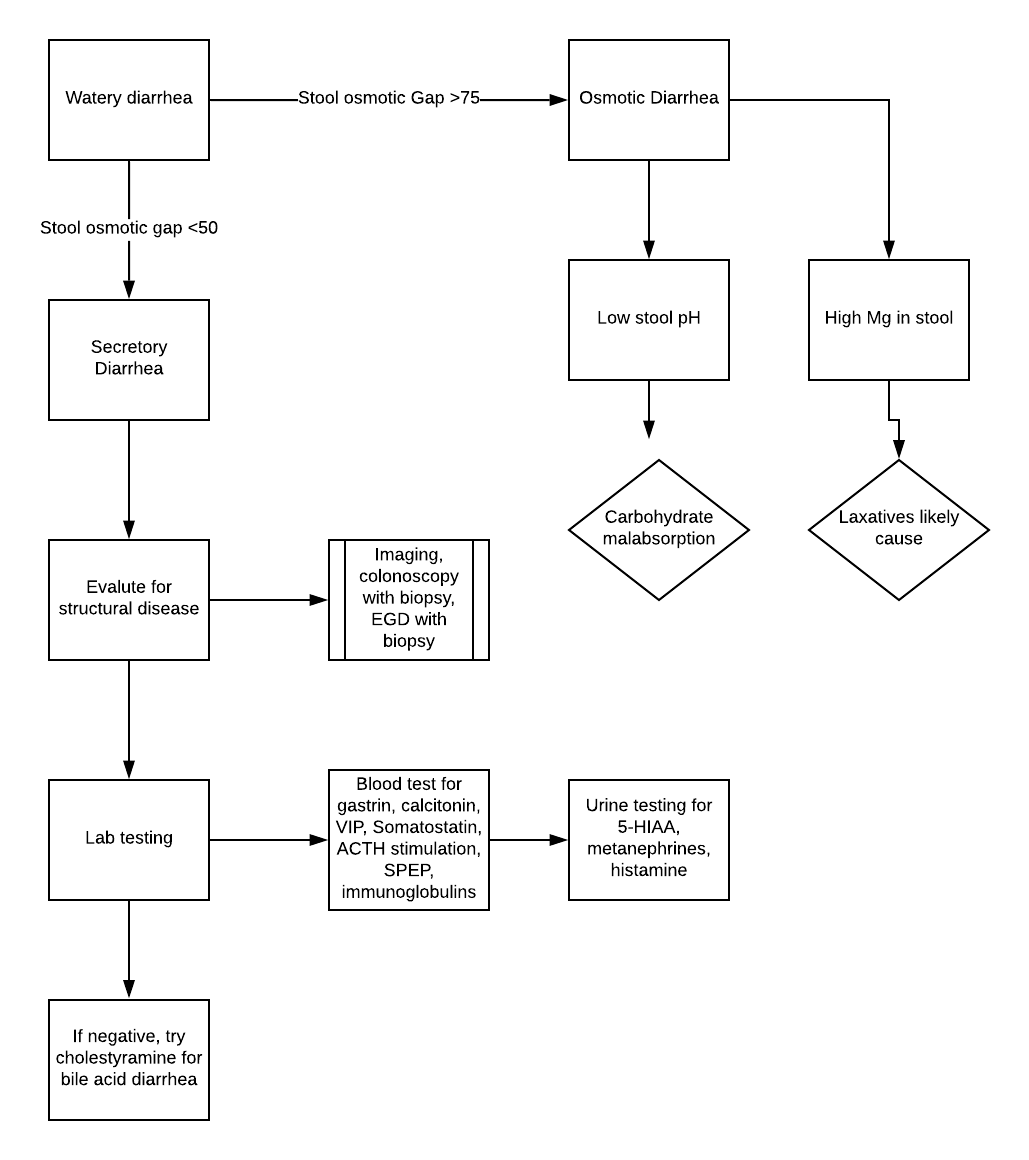
Diagnostic approach for watery diarrhea Gastroenterology Volume 116, Issue 6, Pages 1464-1486 (June 1999) DOI: 10.1016/S0016-5085(99)70513-5
References
Riddle MS, DuPont HL, Connor BA. ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults. The American journal of gastroenterology. 2016 May:111(5):602-22. doi: 10.1038/ajg.2016.126. Epub 2016 Apr 12 [PubMed PMID: 27068718]
Shane AL, Mody RK, Crump JA, Tarr PI, Steiner TS, Kotloff K, Langley JM, Wanke C, Warren CA, Cheng AC, Cantey J, Pickering LK. 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2017 Nov 29:65(12):e45-e80. doi: 10.1093/cid/cix669. Epub [PubMed PMID: 29053792]
Level 1 (high-level) evidenceDuPont HL. Persistent Diarrhea: A Clinical Review. JAMA. 2016 Jun 28:315(24):2712-23. doi: 10.1001/jama.2016.7833. Epub [PubMed PMID: 27357241]
DuPont HL. Acute infectious diarrhea in immunocompetent adults. The New England journal of medicine. 2014 Apr 17:370(16):1532-40. doi: 10.1056/NEJMra1301069. Epub [PubMed PMID: 24738670]
Houston KA, Gibb JG, Maitland K. Oral rehydration of malnourished children with diarrhoea and dehydration: A systematic review. Wellcome open research. 2017:2():66. doi: 10.12688/wellcomeopenres.12357.3. Epub 2017 Oct 27 [PubMed PMID: 29090271]
Level 1 (high-level) evidenceMead PS, Slutsker L, Dietz V, McCaig LF, Bresee JS, Shapiro C, Griffin PM, Tauxe RV. Food-related illness and death in the United States. Emerging infectious diseases. 1999 Sep-Oct:5(5):607-25 [PubMed PMID: 10511517]
Level 3 (low-level) evidenceNotario R, Borda N, Gambande T, Sutich E. Species and serovars of enteropathogenic agents associated with acute diarrheal disease in Rosario, Argentina. Revista do Instituto de Medicina Tropical de Sao Paulo. 1996 Jan-Feb:38(1):5-7 [PubMed PMID: 8762632]
Mikhail IA, Fox E, Haberberger RL Jr, Ahmed MH, Abbatte EA. Epidemiology of bacterial pathogens associated with infectious diarrhea in Djibouti. Journal of clinical microbiology. 1990 May:28(5):956-61 [PubMed PMID: 2351738]
Level 2 (mid-level) evidenceTalan D, Moran GJ, Newdow M, Ong S, Mower WR, Nakase JY, Pinner RW, Slutsker L, EMERGEncy ID NET Study Group. Etiology of bloody diarrhea among patients presenting to United States emergency departments: prevalence of Escherichia coli O157:H7 and other enteropathogens. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2001 Feb 15:32(4):573-80 [PubMed PMID: 11181120]
Marder EP, Cieslak PR, Cronquist AB, Dunn J, Lathrop S, Rabatsky-Ehr T, Ryan P, Smith K, Tobin-D'Angelo M, Vugia DJ, Zansky S, Holt KG, Wolpert BJ, Lynch M, Tauxe R, Geissler AL. Incidence and Trends of Infections with Pathogens Transmitted Commonly Through Food and the Effect of Increasing Use of Culture-Independent Diagnostic Tests on Surveillance - Foodborne Diseases Active Surveillance Network, 10 U.S. Sites, 2013-2016. MMWR. Morbidity and mortality weekly report. 2017 Apr 21:66(15):397-403. doi: 10.15585/mmwr.mm6615a1. Epub 2017 Apr 21 [PubMed PMID: 28426643]
Azer SA, Tuma F. Infectious Colitis. StatPearls. 2024 Jan:(): [PubMed PMID: 31335045]
Lutz J, Rieke A, Rieke B. [Traveling with immunodeficiency-Problems and prevention]. Der Internist. 2019 Jul:60(7):701-708. doi: 10.1007/s00108-019-0617-4. Epub [PubMed PMID: 31098645]
Riddle MS, Connor BA, Beeching NJ, DuPont HL, Hamer DH, Kozarsky P, Libman M, Steffen R, Taylor D, Tribble DR, Vila J, Zanger P, Ericsson CD. Guidelines for the prevention and treatment of travelers' diarrhea: a graded expert panel report. Journal of travel medicine. 2017 Apr 1:24(suppl_1):S57-S74. doi: 10.1093/jtm/tax026. Epub [PubMed PMID: 28521004]
Valilis E, Ramsey A, Sidiq S, DuPont HL. Non-O157 Shiga toxin-producing Escherichia coli-A poorly appreciated enteric pathogen: Systematic review. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2018 Nov:76():82-87. doi: 10.1016/j.ijid.2018.09.002. Epub 2018 Sep 14 [PubMed PMID: 30223088]
Level 1 (high-level) evidenceHuicho L, Sanchez D, Contreras M, Paredes M, Murga H, Chinchay L, Guevara G. Occult blood and fecal leukocytes as screening tests in childhood infectious diarrhea: an old problem revisited. The Pediatric infectious disease journal. 1993 Jun:12(6):474-7 [PubMed PMID: 8345979]
van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ (Clinical research ed.). 2010 Jul 15:341():c3369. doi: 10.1136/bmj.c3369. Epub 2010 Jul 15 [PubMed PMID: 20634346]
Level 1 (high-level) evidenceAbraham BP. Fecal Lactoferrin Testing. Gastroenterology & hepatology. 2018 Dec:14(12):713-716 [PubMed PMID: 30804718]
Dinleyici M, Vandenplas Y. Clostridium difficile Colitis Prevention and Treatment. Advances in experimental medicine and biology. 2019:1125():139-146. doi: 10.1007/5584_2018_322. Epub [PubMed PMID: 30689174]
Level 3 (low-level) evidenceBinnicker MJ. Multiplex Molecular Panels for Diagnosis of Gastrointestinal Infection: Performance, Result Interpretation, and Cost-Effectiveness. Journal of clinical microbiology. 2015 Dec:53(12):3723-8 [PubMed PMID: 26311866]
Laghari GS, Hussain Z, Shahzad H. Effect of Zinc Supplementation on the Frequency and Consistency of Stool in Children with Acute Diarrhea. Cureus. 2019 Mar 11:11(3):e4217. doi: 10.7759/cureus.4217. Epub 2019 Mar 11 [PubMed PMID: 31106100]
de Bruyn G. Diarrhoea in adults (acute). BMJ clinical evidence. 2008 Mar 4:2008():. pii: 0901. Epub 2008 Mar 4 [PubMed PMID: 19450323]
Level 1 (high-level) evidenceMurphy GS, Bodhidatta L, Echeverria P, Tansuphaswadikul S, Hoge CW, Imlarp S, Tamura K. Ciprofloxacin and loperamide in the treatment of bacillary dysentery. Annals of internal medicine. 1993 Apr 15:118(8):582-6 [PubMed PMID: 8452323]
Level 1 (high-level) evidenceDryden MS, Gabb RJ, Wright SK. Empirical treatment of severe acute community-acquired gastroenteritis with ciprofloxacin. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1996 Jun:22(6):1019-25 [PubMed PMID: 8783703]
Level 1 (high-level) evidenceAllen SJ, Martinez EG, Gregorio GV, Dans LF. Probiotics for treating acute infectious diarrhoea. The Cochrane database of systematic reviews. 2010 Nov 10:2010(11):CD003048. doi: 10.1002/14651858.CD003048.pub3. Epub 2010 Nov 10 [PubMed PMID: 21069673]
Level 1 (high-level) evidenceXiao HL, Ma SX, Qi HY, Li X, Wang Y, Yin CH. A scoring system for assessing the severity of acute diarrhea of adult patients. World journal of emergency medicine. 2016:7(2):130-4. doi: 10.5847/wjem.j.1920-8642.2016.02.008. Epub [PubMed PMID: 27313808]
Level 2 (mid-level) evidenceYetmar ZA, Beckman TJ. 41-Year-Old Man With Fever and Bloody Diarrhea. Mayo Clinic proceedings. 2019 Aug:94(8):1594-1598. doi: 10.1016/j.mayocp.2019.01.052. Epub [PubMed PMID: 31378234]
Barros LL, Farias AQ, Rezaie A. Gastrointestinal motility and absorptive disorders in patients with inflammatory bowel diseases: Prevalence, diagnosis and treatment. World journal of gastroenterology. 2019 Aug 21:25(31):4414-4426. doi: 10.3748/wjg.v25.i31.4414. Epub [PubMed PMID: 31496621]
Shah A, Talley NJ, Jones M, Kendall BJ, Koloski N, Walker MM, Morrison M, Holtmann GJ. Small Intestinal Bacterial Overgrowth in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Case-Control Studies. The American journal of gastroenterology. 2020 Feb:115(2):190-201. doi: 10.14309/ajg.0000000000000504. Epub [PubMed PMID: 31913194]
Level 2 (mid-level) evidenceKong LC, Wang B, Wang YM, Hu RG, Atiewin A, Gao D, Gao YH, Ma HX. Characterization of bacterial community changes and antibiotic resistance genes in lamb manure of different incidence. Scientific reports. 2019 Jul 12:9(1):10101. doi: 10.1038/s41598-019-46604-y. Epub 2019 Jul 12 [PubMed PMID: 31300748]
Torres AG. Escherichia coli diseases in Latin America-a 'One Health' multidisciplinary approach. Pathogens and disease. 2017 Mar 1:75(2):. doi: 10.1093/femspd/ftx012. Epub [PubMed PMID: 28158404]