
Introduction
Diffuse intrinsic pontine glioma (DIPG) is an aggressive tumor of the brainstem. It almost always affects the pediatric population, with approximately 200 to 300 new annual cases in the United States. Most patients survive less than one year.[1] These patients were primarily treated with radiation therapy, as surgical resection was not a viable option for them. The effects of radiation therapy are temporary, and no chemotherapeutic agent has been effective in treating this pathology. Several clinical trials of new agents and novel therapeutic approaches have emerged over the past decades to improve the outcome of patients with DIPGs, yet no success has been obtained.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The formation of this tumor may be linked to brain development. Studies suggest that the disease process is created by particular cells that exist in very high concentrations, while the cerebral tissue is developing. This theory is supported by the fact that this tumor rarely occurs in adults and almost always occurs in mid-childhood (ages 5 to 10), a period in which the cerebral tissue is very active in development. The model has identified the neural precursor-like cell population in the normal human ventral pons that is linked both anatomically and temporally to the incidence of DIPG.[2][3] The frequency of this cell type during mid-childhood mirrors the bell-shaped incidence curve of DIPG. These cells are notably absent in the midbrain, where DIPGs are virtually nonexistent.[1][4]
On the molecular level, recent advances in the biological understanding of the disease have identified the H3K27M mutation in nearly 80% of DIPGs, leading to the 2016 World Health Organization (WHO) classification of diffuse midline glioma H3K27M-mutant, a grade IV brainstem tumor.[5]
Epidemiology
Brainstem gliomas affect approximately 300 children in the United States each year and are the major cause of death in children with brain tumors. The most common of these is DIPG comprising 80% of the cases. Incidence is 1 to 2 cases per 100,000 population. DIPG has a peak incidence of 6-9 years and a slight preference for males.[6] Among all the tumors in children, they represent 20% of them.
Pathophysiology
One of the most accepted theories for the development of DIPG is a mutation in the H3 gene. Mutations in the N-terminal tail of histone H3 gene have been recently found in midline pontine high-grade gliomas and at a high frequency in DIPG. Substitution of the lysine at position 27 of the H3 encoding gene is the driving force behind DIPG oncogenesis.[7] It is implied that whichever histone H3 variant is targeted by the mutation (H3.1, H3.2, or H3.3), may lead to the development of a DIPG. The H3K27 mutation and loss of H3K27me3 are of paramount importance since it is characteristic of DIPG and likely represents the first genomic event leading to transformation in these tumors. DIPG thus appears as a homogeneous tumor group defined as a glial neoplasm with a stereotypical epigenetic drive consecutive to the histone H3 mutation. All H3K27 mutations described in DIPG appear to have the same epigenomic consequences on the polycomb repressive complex 2 despite the distinct functions and genomic distribution of the different variants.[8]
Histopathology
DIPG belongs to the fibrillary astrocytoma family. Most lesions are WHO grade III or IV.[1][9] Very few cases are WHO grade II, but they act similar to the high-grade cases.[10] The disparity between histological grade and clinical outcome may be overcome by using molecular features in the tumoral cells.[11]
Microscopically, DIPG infiltrates grey and white matter structures. The tumor cells are generally small and monomorphic, but sometimes can be large and pleomorphic. They typically have an astrocytic morphology, although oligodendroglial morphology is also a recognized pattern. The majority of the tumors have mitotic figures, microvascular proliferation, and necrosis. About 10% of DIPGs lack mitotic figures and microvascular proliferation; thus, they are histologically consistent with WHO grade II.
History and Physical
The clinical course for children with DIPG is rapid.[4] Most symptoms start less than four weeks before seeking medical attention. Symptoms are caused by dysfunction of pontine structures, including long tracts and cranial nerve nuclei. Diplopia is usually the first sign secondary to abducens nerve palsy. Damage to the facial nucleus will produce facial weakness or paralysis. Damage to the long motor tracts will produce weakness and hyperreflexia. Dysfunction of the cerebellopontine connections will cause ataxia, dysmetria, dysarthria. A classic triad in DIPG is present in about 50% of the patients, which includes long tract signs, cerebellar signs, and cranial nerve neuropathies.[1][4] Hydrocephalus occurs in less than 10% of the cases, but if untreated, it can progress to coma and death.[12]
Evaluation
Magnetic resonance imaging (MRI) of the brain with and without contrast is the best diagnostic study to evaluate a patient with suspected DIPG. Usually, more than half of the enlarged ventral pons will show an increased signal on the T2 FLAIR MRI sequence. The tumor will not show contrast enhancement, but occasionally, small areas of necrosis can enhance. Higher values on the apparent diffuse coefficient derived from diffusion-weighted MRI images correlates with better median survival.[13][14] Brain MRI will assess leptomeningeal tumor dissemination. MRI of the entire spine is recommended to exclude spinal seeding.[15] In patients without hydrocephalus, a lumbar puncture can be performed for cerebrospinal fluid analysis to evaluate for tumoral cells and circulating tumoral DNA (ctDNA, detecting the H3K27 mutation).[16][17][18]
Treatment / Management
Steroids, specifically dexamethasone, are given, and the goal of treatment is the stabilization of neurological symptoms until possible neurosurgical biopsy or radiation therapy. Complications due to long term use should be avoided; thus, it should be weaned off as quickly as tolerated.[19][20] Steroids stabilize the blood-brain barrier and can affect tissue penetration of systemic therapies.[21] Additionally, dexamethasone use in high-grade gliomas is associated with worse overall survival.[22] During the management, less than 10% of patients diagnosed with DIPGs develop hydrocephalus and require a third ventriculostomy or ventricular shunt.[23](A1)
The most important step in management is obtaining a tissue diagnosis. First, it characterizes the lesion for classification and treatment, and second, it is used for research and development of more effective management strategies. Nevertheless, there has been a historical resistance to biopsy of these tumors, because of anatomical access. Fortunately, the technology has advanced, and stereotactic biopsy is a safe and minimally invasive procedure that has a very low complication rate. Based on the literature, a stereotactic biopsy of DIPG is as safe and diagnostic as a supratentorial biopsy, and the amount of tissue in the biopsy allows for analysis, including whole-genome sequencing.[17][24][25][26](B2)
Radiation oncologists are consulted immediately after diagnosis to plan further treatment. Even though there have been tremendous advancements in radiation and research in oncology, outcomes for survival for children with DIPGs have not changed significantly over the past 20 years.[27] Conventionally fractionated radiotherapy is still the standard of care for children with DIPGs, but hypofractionated radiotherapy has shown promising results when compared with conventional radiotherapy.[27] Radiotherapy is usually given to the tumor for a total dose of 54 Gy for six weeks (1.8-Gy daily fractions). Hypofractionated radiation with 39 Gy using fewer fractions have similar outcomes and is better tolerated in young children.[28][29] Re-irradiation for tumor progression can be considered with 25 Gy given over ten fractions producing a mild symptom or survival benefit.[30][31] Radiosensitizing agents do not improve survival.(A1)
Several clinical trials of various systemic therapies, including stem cell transplantation, temozolomide, gemcitabine, capecitabine, and tyrosine kinase inhibitors have been tested or are ongoing. Still, none have proved to increase the survival of children with DIPGs.[15][32] Convection-enhanced drug delivery systems have brought hope to the treatments of DIPGs. Improvements in this field may provide better drug delivery systems and target these tumor cells directly, especially at the normal brain tissue interface.[33] A new therapy for the management of DIPG is adjuvant multimodal immunotherapy. This therapy consists of vaccination cycles (Newcastle disease virus, mature dendritic cells) and immunogenic cell death therapy (temozolomide, local modulated electro-hyperthermia), offering improved overall survival but warrants further investigation.[34]
Differential Diagnosis
- Midbrain gliomas
- Cervicomedullary glioma
- Pilocytic astrocytoma
- Cavernous malformation
- Demyelinating disease
- Infectious diseases
Prognosis
The prognosis of DPIG is dismal due to the absence of effective therapies. This tumor is the principal cause of death among brain tumors affecting childhood. Most patients are diagnosed before seven years of age. After diagnosis, median survival is usually nine months. Only 10% live for more than two years.[35] When compared to pediatric glioblastoma, the prognosis for DIPG is the worst with less overall survival.
Complications
- Facial paralysis
- Dysphagia
- Respiratory insufficiency
- Hemiparesis
- Deep vein thrombosis
- Hydrocephalus
- Radiation necrosis
- Brain herniation
- Coma
- Surgical complications (intracranial hemorrhage, edema, seizures, and cranial nerve injury)
Consultations
- Neuro oncologist
- Radiation oncologist
- Neuroradiologist
- Neurosurgeon
- Neurologist
- Neuropathologist
- Pediatric intensivist
An early consideration should be the consultation of advanced pediatric care or pediatric palliative care specialists. Offering palliative care services to all patients with DIPG early in the course of the disease provides support for the immediate and ongoing physical, psychological, and social effects this lethal disease will have on the patient and the family. Combined neuro-oncologic and palliative care support maximize how patients and families perform during their treatment and can even help to identify disease-related changes before clinically or radiographically suspected progression.[36]
Deterrence and Patient Education
Patients with DIPG and family members should have a complete understanding of the disease and prognosis to have realistic expectations. The timeline of how early the patient is diagnosed will have an important part in how the family reacts to the situation. It is why, in the early phase, psychologists, psychiatrists, and family therapists should form part of the team. The realities of deficits, physical impediments, and overall conditions after treatments should be clearly explained to the parents. Thorough training of how to manage these situations is necessary, including nasogastric nutrition, foley catheter, the possibility of being bedridden, and sacral ulcers.
Enhancing Healthcare Team Outcomes
While the pediatrician is almost always involved in the care of a patient with DIPG, it is essential to consult with an interprofessional team of specialists that include a neurosurgeon, neuro-oncologist, and radiation oncologist. The nurses are also vital members of the interprofessional group as they will monitor the patient's vital signs and assist with the education of the patient and the family. In the perioperative period for pain, wound infection, and nausea/vomit, the pharmacist will ensure that the patient is on the right analgesics, antiemetics, and appropriate antibiotics. The problem gets even more complicated when the parents suffer the emotional burden of the dismal prognosis of DIPG. Early phase interaction with psychologists, psychiatrists, and family therapists are needed to handle this critical issue.
Media
(Click Image to Enlarge)
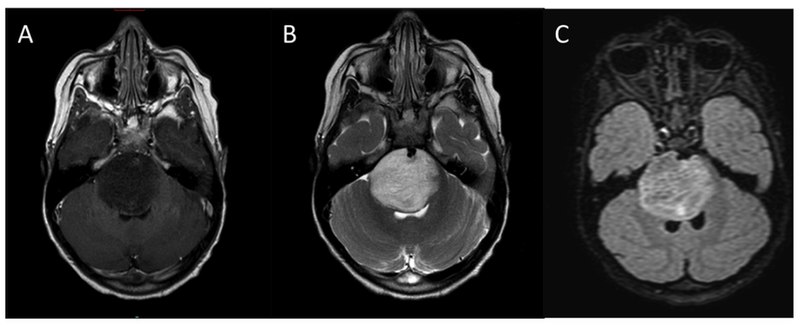
Typical MRI appearance of diffuse intrinsic pontine glioma (DIPG). (A) T1-weighted post contrast, (B) T2-weighted, (C) FLAIR. Contributed from Warren KE (2012) Diffuse intrinsic pontine glioma: poised for progress. Front. Oncol. 2:205. doi:10.3389/fonc.2012.00205 (CC BY 3.0 https://creativecommons.org/licenses/by/3.0/deed.en)
References
Fisher PG, Breiter SN, Carson BS, Wharam MD, Williams JA, Weingart JD, Foer DR, Goldthwaite PT, Tihan T, Burger PC. A clinicopathologic reappraisal of brain stem tumor classification. Identification of pilocystic astrocytoma and fibrillary astrocytoma as distinct entities. Cancer. 2000 Oct 1:89(7):1569-76 [PubMed PMID: 11013373]
Level 2 (mid-level) evidenceShors TJ, Miesegaes G, Beylin A, Zhao M, Rydel T, Gould E. Neurogenesis in the adult is involved in the formation of trace memories. Nature. 2001 Mar 15:410(6826):372-6 [PubMed PMID: 11268214]
Level 3 (low-level) evidenceWeiss S, Dunne C, Hewson J, Wohl C, Wheatley M, Peterson AC, Reynolds BA. Multipotent CNS stem cells are present in the adult mammalian spinal cord and ventricular neuroaxis. The Journal of neuroscience : the official journal of the Society for Neuroscience. 1996 Dec 1:16(23):7599-609 [PubMed PMID: 8922416]
Level 3 (low-level) evidenceDonaldson SS, Laningham F, Fisher PG. Advances toward an understanding of brainstem gliomas. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2006 Mar 10:24(8):1266-72 [PubMed PMID: 16525181]
Level 3 (low-level) evidenceWilliams JR, Young CC, Vitanza NA, McGrath M, Feroze AH, Browd SR, Hauptman JS. Progress in diffuse intrinsic pontine glioma: advocating for stereotactic biopsy in the standard of care. Neurosurgical focus. 2020 Jan 1:48(1):E4. doi: 10.3171/2019.9.FOCUS19745. Epub [PubMed PMID: 31896081]
Chen J, Lin Z, Barrett L, Dai L, Qin Z. Identification of new therapeutic targets and natural compounds against diffuse intrinsic pontine glioma (DIPG). Bioorganic chemistry. 2020 Jun:99():103847. doi: 10.1016/j.bioorg.2020.103847. Epub 2020 Apr 13 [PubMed PMID: 32311581]
Level 2 (mid-level) evidenceCastel D, Philippe C, Calmon R, Le Dret L, Truffaux N, Boddaert N, Pagès M, Taylor KR, Saulnier P, Lacroix L, Mackay A, Jones C, Sainte-Rose C, Blauwblomme T, Andreiuolo F, Puget S, Grill J, Varlet P, Debily MA. Histone H3F3A and HIST1H3B K27M mutations define two subgroups of diffuse intrinsic pontine gliomas with different prognosis and phenotypes. Acta neuropathologica. 2015 Dec:130(6):815-27. doi: 10.1007/s00401-015-1478-0. Epub 2015 Sep 23 [PubMed PMID: 26399631]
Chan KM, Fang D, Gan H, Hashizume R, Yu C, Schroeder M, Gupta N, Mueller S, James CD, Jenkins R, Sarkaria J, Zhang Z. The histone H3.3K27M mutation in pediatric glioma reprograms H3K27 methylation and gene expression. Genes & development. 2013 May 1:27(9):985-90. doi: 10.1101/gad.217778.113. Epub 2013 Apr 19 [PubMed PMID: 23603901]
Yoshimura J, Onda K, Tanaka R, Takahashi H. Clinicopathological study of diffuse type brainstem gliomas: analysis of 40 autopsy cases. Neurologia medico-chirurgica. 2003 Aug:43(8):375-82; discussion 382 [PubMed PMID: 12968803]
Level 3 (low-level) evidenceBuczkowicz P, Bartels U, Bouffet E, Becher O, Hawkins C. Histopathological spectrum of paediatric diffuse intrinsic pontine glioma: diagnostic and therapeutic implications. Acta neuropathologica. 2014 Oct:128(4):573-81. doi: 10.1007/s00401-014-1319-6. Epub 2014 Jul 22 [PubMed PMID: 25047029]
Level 2 (mid-level) evidenceJohung TB, Monje M. Diffuse Intrinsic Pontine Glioma: New Pathophysiological Insights and Emerging Therapeutic Targets. Current neuropharmacology. 2017:15(1):88-97 [PubMed PMID: 27157264]
Schroeder KM, Hoeman CM, Becher OJ. Children are not just little adults: recent advances in understanding of diffuse intrinsic pontine glioma biology. Pediatric research. 2014 Jan:75(1-2):205-9. doi: 10.1038/pr.2013.194. Epub 2013 Nov 5 [PubMed PMID: 24192697]
Level 3 (low-level) evidenceLober RM, Cho YJ, Tang Y, Barnes PD, Edwards MS, Vogel H, Fisher PG, Monje M, Yeom KW. Diffusion-weighted MRI derived apparent diffusion coefficient identifies prognostically distinct subgroups of pediatric diffuse intrinsic pontine glioma. Journal of neuro-oncology. 2014 Mar:117(1):175-82. doi: 10.1007/s11060-014-1375-8. Epub 2014 Feb 13 [PubMed PMID: 24522717]
Leach JL, Roebker J, Schafer A, Baugh J, Chaney B, Fuller C, Fouladi M, Lane A, Doughman R, Drissi R, DeWire-Schottmiller M, Ziegler DS, Minturn JE, Hansford JR, Wang SS, Monje-Deisseroth M, Fisher PG, Gottardo NG, Dholaria H, Packer R, Warren K, Leary SES, Goldman S, Bartels U, Hawkins C, Jones BV. MR imaging features of diffuse intrinsic pontine glioma and relationship to overall survival: report from the International DIPG Registry. Neuro-oncology. 2020 Nov 26:22(11):1647-1657. doi: 10.1093/neuonc/noaa140. Epub [PubMed PMID: 32506137]
Vitanza NA, Monje M. Diffuse Intrinsic Pontine Glioma: From Diagnosis to Next-Generation Clinical Trials. Current treatment options in neurology. 2019 Jul 10:21(8):37. doi: 10.1007/s11940-019-0577-y. Epub 2019 Jul 10 [PubMed PMID: 31290035]
Huang TY, Piunti A, Lulla RR, Qi J, Horbinski CM, Tomita T, James CD, Shilatifard A, Saratsis AM. Detection of Histone H3 mutations in cerebrospinal fluid-derived tumor DNA from children with diffuse midline glioma. Acta neuropathologica communications. 2017 Apr 17:5(1):28. doi: 10.1186/s40478-017-0436-6. Epub 2017 Apr 17 [PubMed PMID: 28416018]
Level 2 (mid-level) evidenceSaratsis AM,Yadavilli S,Magge S,Rood BR,Perez J,Hill DA,Hwang E,Kilburn L,Packer RJ,Nazarian J, Insights into pediatric diffuse intrinsic pontine glioma through proteomic analysis of cerebrospinal fluid. Neuro-oncology. 2012 May; [PubMed PMID: 22492959]
Level 2 (mid-level) evidencePan C, Diplas BH, Chen X, Wu Y, Xiao X, Jiang L, Geng Y, Xu C, Sun Y, Zhang P, Wu W, Wang Y, Wu Z, Zhang J, Jiao Y, Yan H, Zhang L. Molecular profiling of tumors of the brainstem by sequencing of CSF-derived circulating tumor DNA. Acta neuropathologica. 2019 Feb:137(2):297-306. doi: 10.1007/s00401-018-1936-6. Epub 2018 Nov 20 [PubMed PMID: 30460397]
Coutinho AE, Chapman KE. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Molecular and cellular endocrinology. 2011 Mar 15:335(1):2-13. doi: 10.1016/j.mce.2010.04.005. Epub 2010 Apr 14 [PubMed PMID: 20398732]
Level 3 (low-level) evidencePappachan JM, Hariman C, Edavalath M, Waldron J, Hanna FW. Cushing's syndrome: a practical approach to diagnosis and differential diagnoses. Journal of clinical pathology. 2017 Apr:70(4):350-359. doi: 10.1136/jclinpath-2016-203933. Epub 2017 Jan 9 [PubMed PMID: 28069628]
Hue CD, Cho FS, Cao S, Dale Bass CR, Meaney DF, Morrison B 3rd. Dexamethasone potentiates in vitro blood-brain barrier recovery after primary blast injury by glucocorticoid receptor-mediated upregulation of ZO-1 tight junction protein. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2015 Jul:35(7):1191-8. doi: 10.1038/jcbfm.2015.38. Epub 2015 Mar 11 [PubMed PMID: 25757751]
Level 3 (low-level) evidenceLuedi MM, Singh SK, Mosley JC, Hatami M, Gumin J, Sulman EP, Lang FF, Stueber F, Zinn PO, Colen RR. A Dexamethasone-regulated Gene Signature Is Prognostic for Poor Survival in Glioblastoma Patients. Journal of neurosurgical anesthesiology. 2017 Jan:29(1):46-58 [PubMed PMID: 27653222]
Guida L, Roux FE, Massimino M, Marras CE, Sganzerla E, Giussani C. Safety and efficacy of Endoscopic Third Ventriculostomy in Diffuse Intrinsic Pontine Glioma related hydrocephalus: a Systematic Review. World neurosurgery. 2018 Dec 29:():. pii: S1878-8750(18)32919-X. doi: 10.1016/j.wneu.2018.12.096. Epub 2018 Dec 29 [PubMed PMID: 30599251]
Level 1 (high-level) evidencePuget S, Beccaria K, Blauwblomme T, Roujeau T, James S, Grill J, Zerah M, Varlet P, Sainte-Rose C. Biopsy in a series of 130 pediatric diffuse intrinsic Pontine gliomas. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2015 Oct:31(10):1773-80. doi: 10.1007/s00381-015-2832-1. Epub 2015 Sep 9 [PubMed PMID: 26351229]
Kieran MW. Time to rethink the unthinkable: upfront biopsy of children with newly diagnosed diffuse intrinsic pontine glioma (DIPG). Pediatric blood & cancer. 2015 Jan:62(1):3-4. doi: 10.1002/pbc.25266. Epub 2014 Oct 4 [PubMed PMID: 25284709]
Carai A, Mastronuzzi A, De Benedictis A, Messina R, Cacchione A, Miele E, Randi F, Esposito G, Trezza A, Colafati GS, Savioli A, Locatelli F, Marras CE. Robot-Assisted Stereotactic Biopsy of Diffuse Intrinsic Pontine Glioma: A Single-Center Experience. World neurosurgery. 2017 May:101():584-588. doi: 10.1016/j.wneu.2017.02.088. Epub 2017 Feb 27 [PubMed PMID: 28254596]
Gallitto M, Lazarev S, Wasserman I, Stafford JM, Wolden SL, Terezakis SA, Bindra RS, Bakst RL. Role of Radiation Therapy in the Management of Diffuse Intrinsic Pontine Glioma: A Systematic Review. Advances in radiation oncology. 2019 Jul-Sep:4(3):520-531. doi: 10.1016/j.adro.2019.03.009. Epub 2019 Mar 30 [PubMed PMID: 31360809]
Level 3 (low-level) evidenceJanssens GO, Jansen MH, Lauwers SJ, Nowak PJ, Oldenburger FR, Bouffet E, Saran F, Kamphuis-van Ulzen K, van Lindert EJ, Schieving JH, Boterberg T, Kaspers GJ, Span PN, Kaanders JH, Gidding CE, Hargrave D. Hypofractionation vs conventional radiation therapy for newly diagnosed diffuse intrinsic pontine glioma: a matched-cohort analysis. International journal of radiation oncology, biology, physics. 2013 Feb 1:85(2):315-20. doi: 10.1016/j.ijrobp.2012.04.006. Epub 2012 Jun 9 [PubMed PMID: 22682807]
Level 2 (mid-level) evidenceZaghloul MS, Eldebawy E, Ahmed S, Mousa AG, Amin A, Refaat A, Zaky I, Elkhateeb N, Sabry M. Hypofractionated conformal radiotherapy for pediatric diffuse intrinsic pontine glioma (DIPG): a randomized controlled trial. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2014 Apr:111(1):35-40. doi: 10.1016/j.radonc.2014.01.013. Epub 2014 Feb 20 [PubMed PMID: 24560760]
Level 1 (high-level) evidenceFreese C, Takiar V, Fouladi M, DeWire M, Breneman J, Pater L. Radiation and subsequent reirradiation outcomes in the treatment of diffuse intrinsic pontine glioma and a systematic review of the reirradiation literature. Practical radiation oncology. 2017 Mar-Apr:7(2):86-92. doi: 10.1016/j.prro.2016.11.005. Epub 2016 Nov 23 [PubMed PMID: 28274399]
Level 1 (high-level) evidenceLassaletta A, Strother D, Laperriere N, Hukin J, Vanan MI, Goddard K, Lafay-Cousin L, Johnston DL, Zelcer S, Zapotocky M, Rajagopal R, Ramaswamy V, Hawkins C, Tabori U, Huang A, Bartels U, Bouffet E. Reirradiation in patients with diffuse intrinsic pontine gliomas: The Canadian experience. Pediatric blood & cancer. 2018 Jun:65(6):e26988. doi: 10.1002/pbc.26988. Epub 2018 Jan 25 [PubMed PMID: 29369515]
Rechberger JS, Lu VM, Zhang L, Power EA, Daniels DJ. Clinical trials for diffuse intrinsic pontine glioma: the current state of affairs. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2020 Jan:36(1):39-46. doi: 10.1007/s00381-019-04363-1. Epub 2019 Sep 6 [PubMed PMID: 31489454]
Janjua MB, Ban VS, El Ahmadieh TY, Hwang SW, Samdani AF, Price AV, Weprin BE, Batjer H. Diffuse intrinsic pontine gliomas: Diagnostic approach and treatment strategies. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2020 Feb:72():15-19. doi: 10.1016/j.jocn.2019.12.001. Epub 2019 Dec 20 [PubMed PMID: 31870682]
Van Gool SW, Makalowski J, Bonner ER, Feyen O, Domogalla MP, Prix L, Schirrmacher V, Nazarian J, Stuecker W. Addition of Multimodal Immunotherapy to Combination Treatment Strategies for Children with DIPG: A Single Institution Experience. Medicines (Basel, Switzerland). 2020 May 19:7(5):. doi: 10.3390/medicines7050029. Epub 2020 May 19 [PubMed PMID: 32438648]
Rashed WM, Maher E, Adel M, Saber O, Zaghloul MS. Pediatric diffuse intrinsic pontine glioma: where do we stand? Cancer metastasis reviews. 2019 Dec:38(4):759-770. doi: 10.1007/s10555-019-09824-2. Epub [PubMed PMID: 31802357]
Mandrell BN, Baker J, Levine D, Gattuso J, West N, Sykes A, Gajjar A, Broniscer A. Children with minimal chance for cure: parent proxy of the child's health-related quality of life and the effect on parental physical and mental health during treatment. Journal of neuro-oncology. 2016 Sep:129(2):373-81. doi: 10.1007/s11060-016-2187-9. Epub 2016 Jun 25 [PubMed PMID: 27344555]
Level 2 (mid-level) evidence