Indications
Dopamine (DA) is a peripheral vasostimulant used to treat low blood pressure, low heart rate, and cardiac arrest, especially in acute neonatal cases via a continuous intravenous drip.[1] Low infusion rates (0.5 to 2 micrograms/kg per minute) act on the visceral vasculature to produce vasodilation, including the kidneys, resulting in increased urinary flow. Intermediate infusion rates (from 2 to 10 micrograms/kg/min) stimulate myocardial contractility and increase electrical conductivity in the heart leading to increased cardiac output. Higher doses cause vasoconstriction and increased blood pressure via the adrenergic receptors alpha-1, beta-1, and beta-2, potentially leading to poor peripheral circulation.[2]
Indications for DA include maintenance of blood pressure for chronic congestive heart failure, trauma, renal failure, and even open-heart surgery and shock from myocardial infarction or septicemia. DA administration in low doses may also be beneficial to manage hypotension, low cardiac output, and inadequate organ perfusion (often indicated by low urine production). DA gained significant clinical importance in the central nervous system (CNS) after Hornykiewicz's experiments showed its reduction within the caudate nucleus of patients with Parkinson disease. Furthermore, the intravenous administration of its amino acid precursor, L-DOPA (L-dihydroxyphenylalanine), attenuated the Parkinsonian symptoms.[3] Since the blood-brain barrier prohibits the crossing of DA into the CNS from the systemic circulation, DA is ineffective on central neurological deficits such as Parkinson disease. However, L-DOPA successfully crosses the blood-brain barrier and can be administered systemically, including oral pills. Although the therapeutic replacement of dopamine effectively alleviates motor symptoms, it may lead to motor side-effects and behavioral issues associated with addiction (i.e., impulse control disorders.)[4]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Dopamine biosynthesis occurs following the same enzymatic sequence as norepinephrine (NE). In fact, DA is a precursor in the synthesis of NE (see Figure).[5][6] The first step of DA synthesis is rate-limiting and involves converting L-tyrosine to L-DOPA by the enzyme tyrosine hydroxylase (TH) enzyme.[7][8][9] This conversion requires oxygen, an iron co-factor, and tetrahydrobiopterin (BH4 or THB) and results in adding a hydroxyl group to the aromatic ring to form L-DOPA. This molecule subsequently converts to DA by the aromatic L-amino acid decarboxylase, involving removing the carboxyl group. Once synthesized, DA is transported into synaptic vesicles via the vesicular monoamine transporter 2 (VMAT2) to the synaptic terminals.[10][11][12]
If an individual regularly consumes L-tyrosine in abundance, it readily crosses the blood-brain barrier, as does L-DOPA.[13]. But its utility is spatially restricted because DA cannot cross the blood-brain barrier. However, if L-tyrosine levels are low, L-phenylalanine may be converted into L-tyrosine by phenylalanine hydroxylase.
After DA release into the synaptic space, it interacts with various receptors on the pre and post-synaptic terminals, causing neuronal excitation or inhibition at the target neuron. There are two entire families of DA receptors composed of five different isoforms, each affecting different intracellular signaling pathways.[14] Both families of dopamine receptors, D1 and D2, are, by definition, G-protein-coupled receptors, but the D1 receptor class results in the neuron's depolarization, whereas the D2 receptors inhibit neuronal firing.[15]
Once in the synaptic cleft, DA is transported back into the pre-synaptic neuron via DA transporters (DAT) for repackaging or can remain in the extracellular space to be taken up by glial cells or metabolized by the cellular membrane. DA may be metabolized extraneuronally by catechol-o-methyltransferase (COMT) to 3-methoxytyramine (3-MT), while monoamine oxidase-B (MAO-B) will rapidly metabolize 3-MT to homovanillic acid (HVA).[16][17] Alternatively, it may undergo metabolism inside the cytoplasm, where the dual action of MAO-A and aldehyde dehydrogenase (ALDH) will convert DA to the phenolic acid 3, 4-dihydroxyphenylacetic acid (DOPAC).[18]
Given this complex sequence, the modulation of dopamine can occur at various levels, such as the entire neuron, its projections, or the neuronal circuitry across the nervous system. Also, during the synthesis of DA (transcriptional, translational, and post-translational regulation), synaptosomal packaging (regulation of VMAT, transport of vesicle to synapse), DA release (neuronal depolarization, calcium signaling, vesicle fusion), and via reuptake and metabolism through regulation of the respective enzymes and their spatial localization relative to their substrate.[18][19]
As indicated earlier, the systemic action of DA is subject to mediation by various receptors (D1, D2, D3, D4, and D5) and the alpha- and beta-adrenergic receptors. These G-coupled receptors generally group as either D1 or D2, primarily based on their traditional biochemical functions showing that dopamine can modulate adenylyl cyclase activity.[6][20] However, based on their molecular structure, biochemical properties, and pharmacological functions, DA receptors are further classified either as D1-class (D1 and D5) or D2-class (D2, D3, D4).[21][22][23][15]
Activation of the D1 receptors on smooth muscle, the proximal renal tubule, and cortical collecting duct increase diuresis.[24] D2 receptors are located pre-synaptically on the renal nerves and within the glomeruli and adrenal cortex. The activation of these nerves results in decreased renal sodium and water excretion.[25] Apomorphine is a DA receptor agonist and may have similar activation on these DA receptors.[26] Adrenergic receptors also bind DA increasing arterial smooth muscle contraction and cardiac sinoatrial node conductivity, which explains its cardiac therapeutic benefits.
While the blood-brain barrier specifically restricts the transport of DA from the systemic circulation to the central nervous system, further research has led to the discovery of its central role in reward-seeking behavior, wherein its transmission becomes markedly increased. Current DA research includes epigenetic changes and their involvement in a variety of psychiatric conditions, including substance abuse and addiction, schizophrenia, and attention deficit disorder.[27][28] Altogether, these conditions involve disorders of the mesolimbic and mesocortical DA pathways. One common effect of addictive drugs in the CNS is the increased release of DA in the striatum, classically associated with high locomotor activity and stereotypy.[29][30] The striatal DA increase results from axon projections arising directly from the pars compacta of the substantia nigra (SN) and the ventral tegmental area (VTA), respectively, which project to the nucleus accumbens and amygdala, implicated in reward-stimulation and the fear-response.[29][31][32]
Another DA circuit, the tuberoinfundibular pathway, is mainly responsible for regulating the neuroendocrine prolactin from the anterior pituitary gland, known for its role as a lactation inducer, but also has lesser roles in water/salt homeostasis and immune response and cell-cycle regulation.[33][34] The nigrostriatal pathway is the main pathway involved in the motor deficits observed in Parkinson's disease.[35] This pathway comprises dopaminergic neurons originating in the substantia nigra (pars compacta) and projects to the striatum via the medial forebrain bundle, forming synapses with several neuronal populations at the putamen, caudate nucleus, globus pallidus internus (GPi), and the subthalamic nucleus (STN), respectively. This elaborated network forms the afferent connections of the substantia nigra to the circuitry involved in motor movement, namely the basal ganglia. In the latter, DA plays a pivotal function in controlling motor movement and learning new motor skills.[36]
Administration
For stimulation of the sympathetic nervous system, the indication is for a continuous intravenous drip administration. Dopamine half-life in the systemic circulation is between 1 to 5 minutes; thus, slower forms of administration, such as oral administration, are typically ineffective.[37]
In addition to its peripheral sympathetic effects, DA is also critical for neurological movement function in Parkinson’s disease.[35] L-DOPA administration is via the oral route, and after its absorption, a small percentage transports to the brain, where the neurons use it in the basal ganglia. L-DOPA is generally administered concomitantly with carbidopa to inhibit the peripheral effects of L-DOPA in the sympathetic nervous system. Carbidopa is a decarboxylase inhibitor that prevents the systemic conversion of L-DOPA to DA, which decreases the presentation of common side effects such as nausea and emesis.[38]
Adverse Effects
Dopamine administration can adversely affect kidney function, causing increased urinary flow and irregular heartbeat.[39] Excessive administration may cause deleterious conditions such as cerebrovascular accidents due to elevated blood pressure in the brain.[40]
As previously stated, the neurotransmitter DA also acts centrally within the mesocorticolimbic pathway and has roles in processing reward and fear, as well as focusing attention and executive functioning, including complex planning.[31][32] While systemic dopamine does not cross the blood-brain barrier, central dopamine carries implications in somnolence, schizophrenia, addiction, and impulse control disorders.[13][27][41] Patients with neurologic conditions using high doses of L-DOPA for Parkinson disease may experience such physiological alterations from the dysregulation of DA within the CNS pathways.
Contraindications
In patients with conditions of the heart or circulatory system, the intravenous administration of dopamine is contraindicated. These conditions may include ventricular arrhythmias and tachycardia, blood vessel blockage, low blood-oxygen content, decreased blood volume, acidosis, and adrenal gland dysfunctions resulting in high blood pressure such as pheochromocytoma. For patients recently treated with monoamine oxidase inhibitors, DA is initially used in fractional doses (one-tenth usual dose) and closely monitored for further effects. Medications to treat hypertension, such as beta and alpha-adrenergic inhibitors, antagonize the therapeutic effects of DA. Haloperidol also blocks the systemic effects of DA. The anticonvulsant phenytoin has been reported to cause hypotension and decreased heart rate when used with DA. On the other hand, tricyclic antidepressants increase the DA response, similar to anesthetic agents such as cyclopropane and halogenated. In combination with oxytocin, the use of DA can lead to chronic hypertension and may also cause cerebrovascular accidents.[42]
Monitoring
Monitoring blood pressure and urine flow is necessary — monitoring of more advanced hemodynamic parameters such as cardiac output, including rhythm and pulmonary wedge pressure, is also recommended. It is worth noting that dopamine agonists and mimetics that cross the blood-brain barrier interact with the neurological circuitry involved in motor, executive, and limbic functions, including addiction-linked reward systems, impulse control mechanisms, and arousal. Thus, the cessation of DA therapies may lead to a condition called dopamine agonist withdrawal syndrome. This condition has wide-ranging symptoms, including anxiety, depression, panic attacks, fatigue, hypotension, nausea, irritability, and even suicidal ideations.[43] Therefore, recommendations are to taper patients off of these centrally acting DA agonists.
Toxicity
According to "Sax's Dangerous Properties of Industrial Materials" (by Richard J. Lewis, 2004 - DOI: 10.1002/0471701343), studies in rodents showed an LD50 (a lethal dose in 50% of subjects) between 59 to 163 mg/kg. In humans, dopamine can lead to peripheral vasoconstriction resulting in gangrenous extremities and cardiac arrhythmias.[44][45]
Enhancing Healthcare Team Outcomes
Dopamine administration affects the cardiovascular system, as well as other organs, including the kidneys and the brain. Contraindications include specific pharmaceutical agents, lifestyle, and nutrition factors that can impact similar organs with DA treatment. These factors and medications include psychopharmacological agents, neuroleptics, general anesthetics, and even physical therapy-induced cardiac challenges. Communication among all interprofessional healthcare team members, including clinicians, mid-level practitioners, nurses, pharmacists, and therapists, is critical to ensuring proper application of DA to mitigate potentially harmful or chronic adverse effects while considering a holistic healthcare approach along with specific outcome objectives. By engaging in interprofessional teamwork and communication, dopamine therapy can achieve its best possible outcomes with the fewest adverse events. [Level 5]
Media
(Click Image to Enlarge)
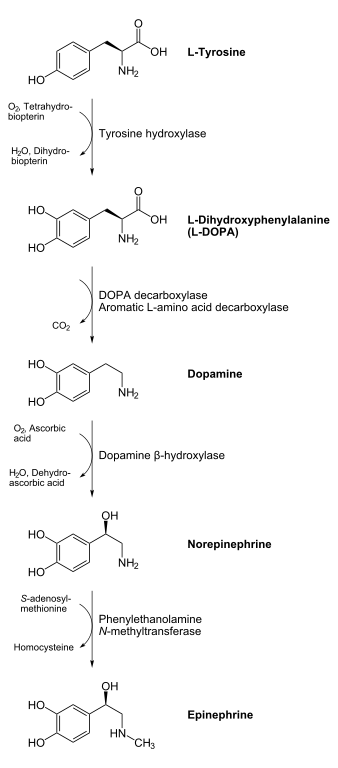
Biosynthesis of catecholamines adrenaline (epinephrine) and noradrenaline (norepinephrine), intermediates DOPA and dopamine Contribtued by NEUROtiker, CC-BY-SA 2.5 ( https://creativecommons.org/licenses/by-sa/2.5/ )
References
Bhatt-Mehta V, Nahata MC. Dopamine and dobutamine in pediatric therapy. Pharmacotherapy. 1989:9(5):303-14 [PubMed PMID: 2682552]
De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C, Brasseur A, Defrance P, Gottignies P, Vincent JL, SOAP II Investigators. Comparison of dopamine and norepinephrine in the treatment of shock. The New England journal of medicine. 2010 Mar 4:362(9):779-89. doi: 10.1056/NEJMoa0907118. Epub [PubMed PMID: 20200382]
Level 1 (high-level) evidenceHornykiewicz O. A brief history of levodopa. Journal of neurology. 2010 Nov:257(Suppl 2):S249-52. doi: 10.1007/s00415-010-5741-y. Epub [PubMed PMID: 21080185]
Level 3 (low-level) evidenceGhadery C, Valli M, Mihaescu A, Strafella R, Navalpotro I, Kim J, Strafella AP. Molecular Imaging of Addictive Behavior in Idiopathic Parkinson's Disease. International review of neurobiology. 2018:141():365-404. doi: 10.1016/bs.irn.2018.07.030. Epub 2018 Aug 13 [PubMed PMID: 30314604]
Blaschko H. The activity of l(-)-dopa decarboxylase. The Journal of physiology. 1942 Nov 30:101(3):337-49 [PubMed PMID: 16991567]
Snyder SH. What dopamine does in the brain. Proceedings of the National Academy of Sciences of the United States of America. 2011 Nov 22:108(47):18869-71. doi: 10.1073/pnas.1114346108. Epub 2011 Nov 21 [PubMed PMID: 22106252]
CARLSSON A, LINDQVIST M, MAGNUSSON T. 3,4-Dihydroxyphenylalanine and 5-hydroxytryptophan as reserpine antagonists. Nature. 1957 Nov 30:180(4596):1200 [PubMed PMID: 13483658]
Abbott A. Neuroscience: the molecular wake-up call. Nature. 2007 May 24:447(7143):368-70 [PubMed PMID: 17522649]
Level 3 (low-level) evidenceMONTAGU KA. Catechol compounds in rat tissues and in brains of different animals. Nature. 1957 Aug 3:180(4579):244-5 [PubMed PMID: 13451690]
Level 3 (low-level) evidenceSANO I, GAMO T, KAKIMOTO Y, TANIGUCHI K, TAKESADA M, NISHINUMA K. Distribution of catechol compounds in human brain. Biochimica et biophysica acta. 1959 Apr:32():586-7 [PubMed PMID: 14441532]
Carlsson A, Kehr W, Lindqvist M, Magnusson T, Atack CV. Regulation of monoamine metabolism in the central nervous system. Pharmacological reviews. 1972 Jun:24(2):371-84 [PubMed PMID: 4564607]
Level 3 (low-level) evidenceHaavik J, Toska K. Tyrosine hydroxylase and Parkinson's disease. Molecular neurobiology. 1998 Jun:16(3):285-309 [PubMed PMID: 9626667]
Level 3 (low-level) evidenceHardebo JE, Edvinsson L, Owman C, Rosengren E. Quantitative evaluation of the blood-brain barrier capacity to form dopamine from circulating L-DOPA. Acta physiologica Scandinavica. 1977 Mar:99(3):377-84 [PubMed PMID: 848309]
Level 3 (low-level) evidenceSibley DR, Monsma FJ Jr, Shen Y. Molecular neurobiology of dopaminergic receptors. International review of neurobiology. 1993:35():391-415 [PubMed PMID: 8463063]
Level 3 (low-level) evidenceDavid C, Fishburn CS, Monsma FJ Jr, Sibley DR, Fuchs S. Synthesis and processing of D2 dopamine receptors. Biochemistry. 1993 Aug 17:32(32):8179-83 [PubMed PMID: 8347618]
Level 3 (low-level) evidenceTank AW, Weiner H, Thurman JA. Enzymology and subcellular localization of aldehyde oxidation in rat liver. Oxidation of 3,4-dihydroxyphenylacetaldehyde derived from dopamine to 3,4-dihydroxyphenylacetic acid. Biochemical pharmacology. 1981 Dec 15:30(24):3265-75 [PubMed PMID: 7034733]
Level 3 (low-level) evidenceKopin IJ. Catecholamine metabolism: basic aspects and clinical significance. Pharmacological reviews. 1985 Dec:37(4):333-64 [PubMed PMID: 3915090]
Level 3 (low-level) evidenceMeiser J, Weindl D, Hiller K. Complexity of dopamine metabolism. Cell communication and signaling : CCS. 2013 May 17:11(1):34. doi: 10.1186/1478-811X-11-34. Epub 2013 May 17 [PubMed PMID: 23683503]
Seamans JK, Yang CR. The principal features and mechanisms of dopamine modulation in the prefrontal cortex. Progress in neurobiology. 2004 Sep:74(1):1-58 [PubMed PMID: 15381316]
Level 3 (low-level) evidenceMeder D, Herz DM, Rowe JB, Lehéricy S, Siebner HR. The role of dopamine in the brain - lessons learned from Parkinson's disease. NeuroImage. 2019 Apr 15:190():79-93. doi: 10.1016/j.neuroimage.2018.11.021. Epub 2018 Nov 20 [PubMed PMID: 30465864]
Mills A. Dopamine: from Cinderella to Holy Grail. Trends in pharmacological sciences. 1992 Nov:13(11):399-400 [PubMed PMID: 1440875]
Level 3 (low-level) evidenceBeaulieu JM, Gainetdinov RR. The physiology, signaling, and pharmacology of dopamine receptors. Pharmacological reviews. 2011 Mar:63(1):182-217. doi: 10.1124/pr.110.002642. Epub 2011 Feb 8 [PubMed PMID: 21303898]
Level 3 (low-level) evidenceAndersen PH, Gingrich JA, Bates MD, Dearry A, Falardeau P, Senogles SE, Caron MG. Dopamine receptor subtypes: beyond the D1/D2 classification. Trends in pharmacological sciences. 1990 Jun:11(6):231-6 [PubMed PMID: 2200181]
Level 3 (low-level) evidenceGoldberg LI. Dopamine receptors and hypertension. Physiologic and pharmacologic implications. The American journal of medicine. 1984 Oct 5:77(4A):37-44 [PubMed PMID: 6148892]
Level 3 (low-level) evidenceVelasco M, Luchsinger A. Dopamine: pharmacologic and therapeutic aspects. American journal of therapeutics. 1998 Jan:5(1):37-43 [PubMed PMID: 10099036]
Montastruc JL, Chamontin B, Rostin M, Rascol O, Valet P, Gaillard G, Tran MA, Van TT, Ader JL, Montastruc P. Experimental and clinical approaches to treatment of hypertension by dopamine receptor agonists. Clinical and experimental hypertension. Part A, Theory and practice. 1987:9(5-6):1069-84 [PubMed PMID: 3304729]
Feng J, Nestler EJ. Epigenetic mechanisms of drug addiction. Current opinion in neurobiology. 2013 Aug:23(4):521-8. doi: 10.1016/j.conb.2013.01.001. Epub 2013 Jan 29 [PubMed PMID: 23374537]
Level 3 (low-level) evidenceHowes OD, McCutcheon R, Owen MJ, Murray RM. The Role of Genes, Stress, and Dopamine in the Development of Schizophrenia. Biological psychiatry. 2017 Jan 1:81(1):9-20. doi: 10.1016/j.biopsych.2016.07.014. Epub 2016 Aug 6 [PubMed PMID: 27720198]
Wise RA. Addictive drugs and brain stimulation reward. Annual review of neuroscience. 1996:19():319-40 [PubMed PMID: 8833446]
Level 3 (low-level) evidenceWise RA. Drug-activation of brain reward pathways. Drug and alcohol dependence. 1998 Jun-Jul:51(1-2):13-22 [PubMed PMID: 9716927]
Level 3 (low-level) evidenceJellinger KA. Post mortem studies in Parkinson's disease--is it possible to detect brain areas for specific symptoms? Journal of neural transmission. Supplementum. 1999:56():1-29 [PubMed PMID: 10370901]
Level 3 (low-level) evidenceRoot DH, Fabbricatore AT, Ma S, Barker DJ, West MO. Rapid phasic activity of ventral pallidal neurons during cocaine self-administration. Synapse (New York, N.Y.). 2010 Sep:64(9):704-13. doi: 10.1002/syn.20792. Epub [PubMed PMID: 20340176]
Level 3 (low-level) evidenceGrattan DR. 60 YEARS OF NEUROENDOCRINOLOGY: The hypothalamo-prolactin axis. The Journal of endocrinology. 2015 Aug:226(2):T101-22. doi: 10.1530/JOE-15-0213. Epub 2015 Jun 22 [PubMed PMID: 26101377]
Dobolyi A, Grattan DR, Stolzenberg DS. Preoptic inputs and mechanisms that regulate maternal responsiveness. Journal of neuroendocrinology. 2014 Oct:26(10):627-40. doi: 10.1111/jne.12185. Epub [PubMed PMID: 25059569]
Level 3 (low-level) evidenceChristine CW, Aminoff MJ. Clinical differentiation of parkinsonian syndromes: prognostic and therapeutic relevance. The American journal of medicine. 2004 Sep 15:117(6):412-9 [PubMed PMID: 15380498]
Mink JW. Basal ganglia mechanisms in action selection, plasticity, and dystonia. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society. 2018 Mar:22(2):225-229. doi: 10.1016/j.ejpn.2018.01.005. Epub 2018 Jan 17 [PubMed PMID: 29396175]
Perrin G, Papazian L, Martin C. [Dopexamine: a new dopaminergic agonist]. Annales francaises d'anesthesie et de reanimation. 1993:12(3):308-20 [PubMed PMID: 7902685]
Level 3 (low-level) evidenceGilbert JA, Frederick LM, Ames MM. The aromatic-L-amino acid decarboxylase inhibitor carbidopa is selectively cytotoxic to human pulmonary carcinoid and small cell lung carcinoma cells. Clinical cancer research : an official journal of the American Association for Cancer Research. 2000 Nov:6(11):4365-72 [PubMed PMID: 11106255]
Stoker TB, Torsney KM, Barker RA. Emerging Treatment Approaches for Parkinson's Disease. Frontiers in neuroscience. 2018:12():693. doi: 10.3389/fnins.2018.00693. Epub 2018 Oct 8 [PubMed PMID: 30349448]
De Vecchis R, Ciccarelli A, Pucciarelli A. Unloading therapy by intravenous diuretic in chronic heart failure: a double-edged weapon? Journal of cardiovascular medicine (Hagerstown, Md.). 2010 Aug:11(8):571-4. doi: 10.2459/JCM.0b013e32833d37b9. Epub [PubMed PMID: 20588135]
Cho JR, Treweek JB, Robinson JE, Xiao C, Bremner LR, Greenbaum A, Gradinaru V. Dorsal Raphe Dopamine Neurons Modulate Arousal and Promote Wakefulness by Salient Stimuli. Neuron. 2017 Jun 21:94(6):1205-1219.e8. doi: 10.1016/j.neuron.2017.05.020. Epub 2017 Jun 8 [PubMed PMID: 28602690]
Kittner SJ, Stern BJ, Feeser BR, Hebel R, Nagey DA, Buchholz DW, Earley CJ, Johnson CJ, Macko RF, Sloan MA, Wityk RJ, Wozniak MA. Pregnancy and the risk of stroke. The New England journal of medicine. 1996 Sep 12:335(11):768-74 [PubMed PMID: 8703181]
Yu XX, Fernandez HH. Dopamine agonist withdrawal syndrome: A comprehensive review. Journal of the neurological sciences. 2017 Mar 15:374():53-55. doi: 10.1016/j.jns.2016.12.070. Epub 2017 Jan 2 [PubMed PMID: 28104232]
Colak T, Erdogan O, Yerebakan O, Arici C, Gurkan A. Symmetrical peripheral gangrene and dopamine. Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES. 2003 Jul:9(3):222-4 [PubMed PMID: 12923702]
Level 3 (low-level) evidenceGelfman DM, Ornato JP, Gonzalez ER. Dopamine-induced increase in atrioventricular conduction in atrial fibrillation-flutter. Clinical cardiology. 1987 Nov:10(11):671-3 [PubMed PMID: 3677500]
Level 3 (low-level) evidence