Introduction
The thyroid gland is the first endocrine gland that develops during fetal embryology, which starts between the third and fourth gestational weeks. The primary origin of the thyroid gland is the endoderm, which gives rise to the median (the significant portion of each lateral lobe, isthmus and thyroglossal duct with pyramidal lobe), and the two lateral anlages which contain c-cells, solid nests cells and portions of the lateral thyroid.[1] Failure of the thyroid fails to descend from the thyroid anlage region to its final location in front of the trachea is called an ectopic thyroid (see Image. Ectopic Thyroid). Ectopic thyroid can present at any position from the foramen caecum at the base of the tongue to the mediastinum.[2] Dr. Hickman described the first ectopic thyroid in a newborn who died after 16 hours of life due to severe respiratory distress and suffocation. Eventually, the cause turned to be due to ectopic lingual thyroid.[3] The ectopic thyroid is classified under the category of congenital hypothyroidism, and it is one of the top causes of thyroid dysgenesis.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The majority of the causes are multifactorial associated with the embryological process, and recently the genetic research has demonstrated that the gene transcription factors TITF-1(Nkx2-1), Foxe1(TITF-2) and PAX-8 are essential for thyroid maturation and differentiation. Mutation in these genes may share a connection with abnormal migration of the thyroid.[4] The category of the genes listed below may be contributing to the process of ectopic as well as the unusual morphology of the thyroid.[5][6]
- Thyroid ectopy: Genes: 1- NKX2-5 (Ectopy, no cardiac alterations) 2- FOXE1 (Bamforth-Lazarus syndrome)
- Thyroid hypoplasia: Genes: 1- NKX2-1 (Choreoathetosis, hypothyroidism, and pulmonary alterations) 2- TSHR (Resistance to TSH) 3- PAX8 (Hypothyroidism)
- Athyreosis: Genes: 1- FOXE1 (Bamforth-Lazarus syndrome)2- NKX2-5 (Athyreosis, no cardiac alterations) 3- PAX8 (Hypothyroidism)
Epidemiology
The prevalence of ectopic thyroid gland is one case for every 100000 to 300000 of healthy individuals, but it reportedly occurs in one of 4000 to 8000 patients who have thyroid disease.[7] The ectopic thyroid can present at any age, with most cases identified during the neonatal period through newborn screening, but some cases are delayed up to the fourth through the sixth decade when the ectopic thyroid tissue transforms to abnormal tissue pathology and presents with symptomatic manifestations. In other cases, the ectopic thyroid gland enlarges during periods of stress and is then identified during imaging. Both males and females are equally affected.
Pathophysiology
The most common thyroid location in the ectopic cases is the Lingual thyroid. Incomplete migration can lead to a high cervical thyroid, and excessive movement can lead to a superior mediastinal or even paracardiac location. Studies have shown that more than 70% of lingual thyroid cases correlate with the absence of normal cervical thyroid.[8] This percentage is significant to know because not all cases are single ectopic thyroid tissue. Studies are reporting cases of dual and triple ectopic thyroids.[9][10] The other possible locations of ectopic thyroid are:
- In the head and neck: the trachea, submandibular, lateral cervical regions, palatine tonsils, carotid bifurcation, iris of the eye and pituitary gland.
- Axilla
- Heart and ascending aorta
- Lymphoid tissue: thymus
- Gastrointestinal system: esophagus, duodenum, gallbladder, stomach bed, pancreas, mesentery of the small intestine, porta hepatis
- Adrenal gland
- Reproductive system: ovary, fallopian tube, uterus, and vagina
History and Physical
Ectopic lingual thyroid is usually asymptomatic (47%) but may lead to some of the local symptoms such as dysphagia, dysphonia with stomatolalia and upper airway obstruction.[4] Other clinical manifestations of definitive clinical hypothyroidism (like; fatigue, cold intolerance, constipation, dry skin, weight gain, puffy face, hoarseness, muscle weakness) are present in 70% of all reported cases.[11][12] Hyperthyroidism is a very rare association with lingual thyroid, with few cases reported.[13] The local neck examination is essential to rule out other neck masses. The physical examination of the thyroid is not sensitive for identifying the cause of congenital hypothyroidism; the ectopic thyroid could be missed during physical examination even by expert endocrinologists.
Evaluation
Newborn screening is the recommendation since many studies suggest that "almost all individuals with ectopic thyroid are hypothyroid." Thus a biochemical thyroid profile may be necessary at birth. Many centers are now routinely obtaining a thyroid profile in all newborns[14][15][4]
- Serial thyroid function tests (TSH, T3, total T4, free T4, and thyroglobulin are mandatory in the screening and diagnosing of the ectopic thyroid - the majority of the cases will provide evidence of hypothyroidism, while some patients may be euthyroid
- The etiological diagnosis is established by thyroid scintigraphy
- MRI and CT scan also can be used as modalities to determine the exact location of ectopic thyroid
- High-resolution ultrasound scanning could help as an initial assessment, especially in patients presenting with neck masses
- If the case is highly suspicious for malignancy, then tissue biopsy for histology or fine needle aspiration cytology (FNAC) should be performed
Treatment / Management
The quick identification of congenital hypothyroidism and further preventing unwanted intellectual disability by early starting appropriate treatment is paramount.[16] Life long thyroxin replacement therapy and regular follow-up are an optimum choice for such patients.[17][18]
The indications for surgical removal of the ectopic thyroid include the following: malignancy, bleeding or ulceration of the gland, uncontrolled hyperthyroidism, and severe local/respiratory symptoms. Some lingual thyroids are visible in the neck and females prefer surgical removal for cosmetic reasons.[15][19][20][21](B3)
Differential Diagnosis
- Thyroglossal cyst
The differentiation between the lingual ectopic thyroid and thyroglossal duct cyst is by performing thyroid scintigraphy; usually, thyroglossal duct cysts remain unidentified because they do not typically contain sufficient functioning thyroid tissue.[22]
- Other neck masses are included in the differential diagnosis of ectopic thyroid
Complications
Fortunately, the studies have estimated the risk of developing malignancy from ectopic tissue is less than 1%.[23] Benign neoplasms and thyroiditis are also infrequent complications. If the patient is symptomatic and kept without treatment, they are more likely to develop complications of hypothyroidism.
Consultations
For any child who is experiencing frequent high TSH with normal other thyroid function with or without symptoms, especially respiratory or dysphagia symptoms always consider ectopic thyroid and consult the endocrinologist to evaluate the case.
Pearls and Other Issues
Bringing attention to ectopic thyroid is extremely important because it may be the only thyroid tissue or may be causing upper airway symptoms. Also, one should always consider malignancy.
Enhancing Healthcare Team Outcomes
The management of an ectopic thyroid is with an interprofessional team that includes an endocrinologist, ENT surgeon, pediatric surgeon, and a pediatrician. It is crucial to rule out the presence of other functioning thyroid tissue before considering surgical removal. For most patients, removal of the ectopic thyroid tissue has little morbidity, but if it is the only thyroid tissue, the patient will need life long thyroid hormone supplementation.[24] (Level V)
Media
(Click Image to Enlarge)
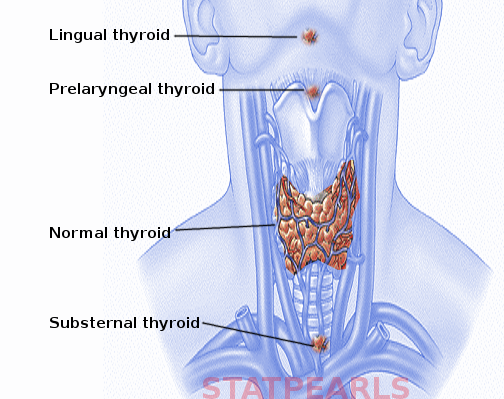
Ectopic Thyroid
Contributed by S Bhimji, MD
References
Johansson E, Andersson L, Örnros J, Carlsson T, Ingeson-Carlsson C, Liang S, Dahlberg J, Jansson S, Parrillo L, Zoppoli P, Barila GO, Altschuler DL, Padula D, Lickert H, Fagman H, Nilsson M. Revising the embryonic origin of thyroid C cells in mice and humans. Development (Cambridge, England). 2015 Oct 15:142(20):3519-28. doi: 10.1242/dev.126581. Epub 2015 Sep 22 [PubMed PMID: 26395490]
Siddique M, Bashir H. 99mTc Sodium Pertechnetate Uptake in Ectopic Mediastinal Thyroid Tissue on Hybrid Thyroid Scintigraphy. Clinical nuclear medicine. 2018 Nov:43(11):820-822. doi: 10.1097/RLU.0000000000002201. Epub [PubMed PMID: 30015662]
Kumar Choudhury B, Kaimal Saikia U, Sarma D, Saikia M, Dutta Choudhury S, Barua S, Dewri S. Dual ectopic thyroid with normally located thyroid: a case report. Journal of thyroid research. 2011:2011():159703. doi: 10.4061/2011/159703. Epub 2011 Jun 16 [PubMed PMID: 21765986]
Level 3 (low-level) evidenceIbrahim NA,Fadeyibi IO, Ectopic thyroid: etiology, pathology and management. Hormones (Athens, Greece). 2011 Oct-Dec; [PubMed PMID: 22281882]
Level 3 (low-level) evidenceNettore IC, Cacace V, De Fusco C, Colao A, Macchia PE. The molecular causes of thyroid dysgenesis: a systematic review. Journal of endocrinological investigation. 2013 Sep:36(8):654-64. doi: 10.3275/8973. Epub 2013 May 22 [PubMed PMID: 23698639]
Level 3 (low-level) evidenceAbu-Khudir R, Paquette J, Lefort A, Libert F, Chanoine JP, Vassart G, Deladoëy J. Transcriptome, methylome and genomic variations analysis of ectopic thyroid glands. PloS one. 2010 Oct 15:5(10):e13420. doi: 10.1371/journal.pone.0013420. Epub 2010 Oct 15 [PubMed PMID: 20976176]
Kim MS, Kong YH, Lee DY. A Case of Subclinical Hypothyroidism with Lingual and Right Pretracheal Ectopic Thyroid. Journal of clinical research in pediatric endocrinology. 2015 Jun:7(2):148-50. doi: 10.4274/jcrpe.1791. Epub [PubMed PMID: 26316439]
Level 3 (low-level) evidenceFisher DA,Klein AH, Thyroid development and disorders of thyroid function in the newborn. The New England journal of medicine. 1981 Mar 19; [PubMed PMID: 6258072]
Level 3 (low-level) evidencePassah A, Arora S, Damle NA, Sharma R. Triple Ectopic Thyroid on Pertechnetate Scintigraphy. Indian journal of endocrinology and metabolism. 2018 Sep-Oct:22(5):712-713. doi: 10.4103/ijem.IJEM_88_18. Epub [PubMed PMID: 30294586]
Matta-Coelho C, Donato S, Carvalho M, Vilar H. Dual ectopic thyroid gland. BMJ case reports. 2018 Oct 2:2018():. pii: bcr-2018-225506. doi: 10.1136/bcr-2018-225506. Epub 2018 Oct 2 [PubMed PMID: 30279251]
Level 3 (low-level) evidenceAmani Mel A, Benabadji N, Benzian Z, Amani S. Ectopic lingual thyroid. Indian journal of nuclear medicine : IJNM : the official journal of the Society of Nuclear Medicine, India. 2012 Apr:27(2):124-6. doi: 10.4103/0972-3919.110718. Epub [PubMed PMID: 23723588]
Level 3 (low-level) evidenceSinghal P,Sharma KR,Singhal A, Lingual thyroid in children. Journal of the Indian Society of Pedodontics and Preventive Dentistry. 2011 Jul-Sep; [PubMed PMID: 21985888]
Level 3 (low-level) evidenceAbdallah-Matta MP, Dubarry PH, Pessey JJ, Caron P. Lingual thyroid and hyperthyroidism: a new case and review of the literature. Journal of endocrinological investigation. 2002 Mar:25(3):264-7 [PubMed PMID: 11936471]
Level 3 (low-level) evidenceJaruratanasirikul S, Piriyaphan J, Saengkaew T, Janjindamai W, Sriplung H. The etiologies and incidences of congenital hypothyroidism before and after neonatal TSH screening program implementation: a study in southern Thailand. Journal of pediatric endocrinology & metabolism : JPEM. 2018 Jun 27:31(6):609-617. doi: 10.1515/jpem-2017-0340. Epub [PubMed PMID: 29750647]
Elprana D, Manni JJ, Smals AG. Lingual thyroid. Case report and review of the literature. ORL; journal for oto-rhino-laryngology and its related specialties. 1984:46(3):147-52 [PubMed PMID: 6728436]
Level 3 (low-level) evidenceAgrawal P,Philip R,Saran S,Gutch M,Razi MS,Agroiya P,Gupta K, Congenital hypothyroidism. Indian journal of endocrinology and metabolism. 2015 Mar-Apr; [PubMed PMID: 25729683]
Swaby R. Lingual thyroid: ectopic gland in the tongue base. Archives of disease in childhood. 2019 Jan 17:():. pii: archdischild-2018-316508. doi: 10.1136/archdischild-2018-316508. Epub 2019 Jan 17 [PubMed PMID: 30655262]
Touati G, Léger J, Toublanc JE, Farriaux JP, Stuckens C, Ponte C, David M, Rochiccioli P, Porquet D, Czernichow P. A thyroxine dosage of 8 micrograms/kg per day is appropriate for the initial treatment of the majority of infants with congenital hypothyroidism. European journal of pediatrics. 1997 Feb:156(2):94-8 [PubMed PMID: 9039509]
Turri-Zanoni M, Battaglia P, Castelnuovo P. Thyroglossal Duct Cyst at the Base of Tongue: The Emerging Role of Transoral Endoscopic-Assisted Surgery. The Journal of craniofacial surgery. 2018 Mar:29(2):469-470. doi: 10.1097/SCS.0000000000004009. Epub [PubMed PMID: 29023300]
Naik K, Redefining anatomy in a case of midline subhyoid ectopic thyroid. The Indian journal of surgery. 2014 Aug; [PubMed PMID: 25278663]
Level 3 (low-level) evidenceJakibchuk K, Ali S, Samantray J. Recurrence of Graves' disease in ectopic thyroid tissue. BMJ case reports. 2018 Jan 23:2018():. pii: bcr-2017-221566. doi: 10.1136/bcr-2017-221566. Epub 2018 Jan 23 [PubMed PMID: 29367360]
Level 3 (low-level) evidenceSturniolo G, Vermiglio F, Moleti M. Thyroid cancer in lingual thyroid and thyroglossal duct cyst. Endocrinologia, diabetes y nutricion. 2017 Jan:64(1):40-43. doi: 10.1016/j.endonu.2016.07.010. Epub 2016 Nov 4 [PubMed PMID: 27825535]
Lianos G, Bali C, Tatsis V, Anastasiadi Z, Lianou E, Papathanasiou V, Messinis T. Ectopic thyroid carcinoma. Case report. Il Giornale di chirurgia. 2013 Apr:34(4):114-6 [PubMed PMID: 23660162]
Level 3 (low-level) evidenceLeung AKC,Leung AAC, Evaluation and management of the child with hypothyroidism. World journal of pediatrics : WJP. 2019 Feb 8 [PubMed PMID: 30734891]