Introduction
Heart failure (HF) is a major cause of morbidity and mortality in the United States and worldwide. It is only second to pancreatic cancer with the shortest life expectancy. It plagues millions of people every year. Currently, over 5 million people have an HF diagnosis, and that number is only expected to rise in the future. Advanced heart failure or stage D disease affects >10% of the heart failure population.[1] In the most advanced phase of heart failure, heart transplantation (HT) is the only means of improving the quality of life and survival in these patients. Unfortunately, not all patients who need a heart transplant meet criteria to receive a heart transplant. This chapter will cover in detail patient selection for a heart transplant including indications, contraindications, medical professionals required to assess patient selection, preparation, and clinical significance.
Indications
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Indications
There are several indications for a heart transplant. About 10-15% of patients currently with heart failure meet requirements for a heart transplant (HT). However, less than half of these obtain a referral for transplant evaluation. Therefore, it is essential to spread awareness of indications for a heart transplant. End-stage heart disease not amenable to other medical or surgical therapy is a class I indication for HT.[2] End-stage heart failure is described as a left ventricular ejection fraction of less than 20% and peak oxygen uptake of less than 12 mL/kg 1/min. Cardiogenic shock, which requires either continuous intravenous inotropic support or mechanical circulatory support with an intra-aortic balloon pump counterpulsation device or LVAD, is also an indication for HT. Other indications include anginal symptoms in the setting of coronary artery disease not amenable to percutaneous or surgical revascularization or medical therapy and lethal arrhythmias resistant to medical therapy, catheter ablation, or implantation of an intracardiac defibrillator.[3]
Contraindications
Eligibility for a heart transplant limited as there are several contraindications to this procedure. Absolute contraindications include a life expectancy under two years despite a heart transplant.[4] Some of the systemic illness that predict a life expectancy of less than two years include: acquired immunodeficiency syndrome with frequent opportunistic infections, a significant pulmonary disease usually identified with FEV less than 1 L/min, malignancy within the past five years, a current active systemic illness such as amyloidosis, sarcoidosis, or lupus, irreversible kidney disease, irreversible liver disease, fixed pulmonary hypertension as defined as pulmonary artery systolic pressure greater than 60 mmHg, mean transpulmonary gradient greater than 15 mmHg, or pulmonary vascular resistance greater than 6 Woods units. [5][6]
There are several more relative contraindications. Caution should be used in any patient presenting with any of the following characteristics: extremes in body mass index including morbid obesity and anorexia/cachexia, kidney dysfunction, liver dysfunction including international ratio (INR) > 1.5 off coumadin, bilirubinemia, active peptic ulcer disease, poorly controlled diabetes or hypertension, severe vascular disease including cerebrovascular or peripheral vascular disease, irreversible neurological disorder, irreversible neuromuscular disorder, heparin-induced thrombocytopenia (HIT) within 100 days, severe pulmonary disease with FEV1 less than 40% of normal, pulmonary infarct within last 2 months, active mental instability, and substance abuse including drugs, tobacco, or alcohol within the last 6 months.[7] Age greater than 72 is also a known relative contraindication, however, according to literature, this is very controversial. One study showed that patients less than 40 years of age had a 100% rate of long-term survival, and lower occurrence of complications.[8] Another study showed no difference in outcome related to age using a personalized approach.[9]
Personnel
The Heart Failure Team should include:
- Primary cardiologist
- Advanced heart failure specialist
- Advanced heart failure nurse
- Cardiovascular pharmacist
- Cardiac rehabilitation specialist
- Palliative care nurse and specialist
- Clinical psychologist
- Clinical psychiatrist
- Primary care physician
Preparation
The heart transplant (HT) process is complex and time-consuming. Preparing a patient with advanced HF for a heart transplant starts first with identifying the current or future need for a transplant. This is by far the most crucial step in the whole process. Once identified, a speedy referral should be placed to a transplant center. Before the transplant appointment, it is imperative that the patient starts on goal-directed medical therapy (GDMT).[1] Patient ideally should be on GDMT for at least 3-6 months before HT to assess therapeutic response.
At the transplant center, an initial evaluation will be done to assess the severity of HF. Then an assessment for possible reversible factors will be made along with an assessment of the effectiveness of current medical therapy. Specific workup should be done on a patient's with valvular or ischemic heart disease. This subset should undergo an assessment with myocardial viability testing as well as percutaneous transcatheter or surgical valve evaluation. Those with arrhythmias should be treated appropriately. For example, patients diagnosed with atrial fibrillation/flutter should be placed on rate controlling agents, and/or rhythm control with medication or cardioversion. Arrhythmia originating from the ventricular chambers should be treated with antiarrhythmic therapy, ablation, and/or implantable defibrillator/pacemaker. Biventricular pacing should be considered for prolonged QRS.[6]
Patients should be instructed to refrain entirely from persistent alcohol intake, illicit drug use, or salt-retaining medications, as well as avoiding NSAIDs.[10] One study found that there is no association between the presence of anxiety and depression and the outcome of heart transplantation. [3] However, many times patients are selected or not selected on this basis. Literature suggests that patients should not be withheld from HT with the presence of mild psychiatric illness. So regardless of the presence of anxiety or depression, if no reversible causes are diagnosed and the patient has been on several months of GDMT in the presence of class IIIB/IV symptoms, then the transplant evaluation process will commence.
If on referral the patient is in cardiogenic shock or on parenteral inotropic agents and cannot be tapered because of hypotension, end-organ dysfunction, or symptoms, then the options for this patient are limited to cardiac transplantation, mechanical device support, or palliative care versus hospice. Evaluation of patients who are not inotrope dependent requires the collection of crucial prognostic factors to estimate patient prognosis and need for transplant listing. Also, one study found that there is no association between the presence of anxiety and depression and the outcome of heart transplantation. [3] However, many times patients are selected or not selected on this basis.
Clinical Significance
Heart transplantation can prolong survival for up to 10 years or more.[2] Having such a positive impact on survival makes the patient selection process for a heart transplant an important focus in today heart failure talks. Understanding the patient selection criteria for a heart transplant is crucial to clinical decision-making and making sure all patients indicated for HT are captured and referred appropriately. It is imperative that physicians treating HF (cardiologist and primary care) to be able to recognize when a heart transplant is needed. Early identification is the key to a successful and speedy heart transplant evaluation and list placement.
Enhancing Healthcare Team Outcomes
An interprofessional team that provides a patient-centered, integrated approach to evaluate patient's for a heart transplant is essential to achieve the best possible outcomes. Furthermore, several studies have shown that the outcome of heart transplantation depends on several other factors outside of meeting clinical criteria such as demographic, psychosocial, and behavioral factors. It is imperative to have an interprofessional team including a cardiologist, thoracic surgeon, anesthetist, clinical psychologist and psychiatrist, pharmacists, and specialty trained nurses.[11] [level 1] In particular, the nurses should assist the team with patient selection, education and monitoring; the clinicians should provide direct care and evaluation for the procedure; the pharmacist should assist in avoiding dangerous drug-drug interactions that may affect the outcome of the procedure; and the behavioralist should assist with helping the patient and family to cope with a challenging procedure fraut with potential complications and delays. [Level 5]
Media
(Click Image to Enlarge)
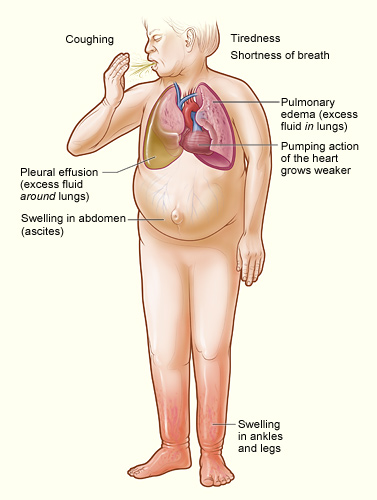
The illustration shows the major signs and symptoms of heart failure. Contributed by National Heart, Lung, and Blood Institute, National Institutes of Health (NIH)
(Click Image to Enlarge)
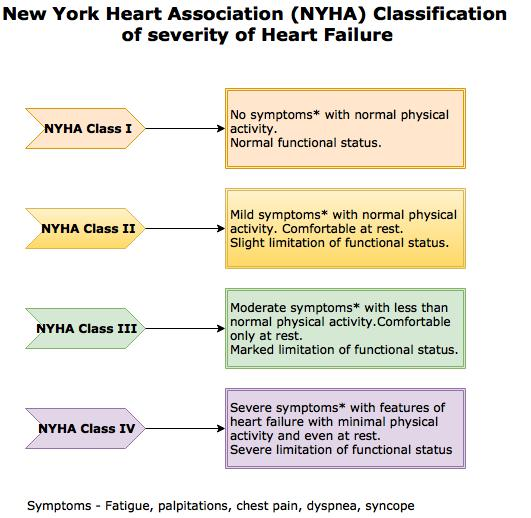
NYHA Classification - Heart failure Contributed by the New York Health Association (NYHA)
References
Ural D, Çavuşoğlu Y, Eren M, Karaüzüm K, Temizhan A, Yılmaz MB, Zoghi M, Ramassubu K, Bozkurt B. Diagnosis and management of acute heart failure. Anatolian journal of cardiology. 2015 Nov:15(11):860-89. doi: 10.5152/AnatolJCardiol.2015.6567. Epub [PubMed PMID: 26574757]
Harris C, Cao C, Croce B, Munkholm-Larsen S. Heart transplantation. Annals of cardiothoracic surgery. 2018 Jan:7(1):172. doi: 10.21037/acs.2018.01.11. Epub [PubMed PMID: 29492396]
Tecson KM, Bass K, Felius J, Hall SA, Jamil AK, Carey SA. Patient "Activation" of Patients Referred for Advanced Heart Failure Therapy. The American journal of cardiology. 2019 Feb 15:123(4):627-631. doi: 10.1016/j.amjcard.2018.11.013. Epub 2018 Nov 24 [PubMed PMID: 30527769]
Kirklin JK. Terminal heart failure: who should be transplanted and who should have mechanical circulatory support? Current opinion in organ transplantation. 2014 Oct:19(5):486-93. doi: 10.1097/MOT.0000000000000120. Epub [PubMed PMID: 25186823]
Level 3 (low-level) evidenceFreeman R, Koerner E, Clark C, Halabicky K. The Path From Heart Failure to Cardiac Transplant. Critical care nursing quarterly. 2016 Jul-Sep:39(3):207-13. doi: 10.1097/CNQ.0000000000000114. Epub [PubMed PMID: 27254637]
Prieto D, Correia P, Antunes P, Batista M, Antunes MJ. Results of heart transplantation in the urgent recipient--who should be transplanted? Revista brasileira de cirurgia cardiovascular : orgao oficial da Sociedade Brasileira de Cirurgia Cardiovascular. 2014 Jul-Sep:29(3):379-87 [PubMed PMID: 25372913]
Cimato TR, Jessup M. Recipient selection in cardiac transplantation: contraindications and risk factors for mortality. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation. 2002 Nov:21(11):1161-73 [PubMed PMID: 12431490]
Prieto D, Correia P, Batista M, Antunes Mde J. Heart Transplantation in Patients Older than 65 Years: Worthwhile or Wastage of Organs? The Thoracic and cardiovascular surgeon. 2015 Dec:63(8):684-91. doi: 10.1055/s-0034-1393959. Epub 2014 Nov 21 [PubMed PMID: 25415627]
Sponga S, Deroma L, Sappa R, Piani D, Lechiancole A, Spagna E, Tursi V, Nalli C, Livi U. Recipient age impact on outcome after cardiac transplantation: should it still be considered in organ allocation? Interactive cardiovascular and thoracic surgery. 2016 Oct:23(4):573-9. doi: 10.1093/icvts/ivw184. Epub 2016 Jun 16 [PubMed PMID: 27316658]
Kalter-Leibovici O, Freimark D, Freedman LS, Kaufman G, Ziv A, Murad H, Benderly M, Silverman BG, Friedman N, Cukierman-Yaffe T, Asher E, Grupper A, Goldman D, Amitai M, Matetzky S, Shani M, Silber H, Israel Heart Failure Disease Management Study (IHF-DMS) investigators. Disease management in the treatment of patients with chronic heart failure who have universal access to health care: a randomized controlled trial. BMC medicine. 2017 May 1:15(1):90. doi: 10.1186/s12916-017-0855-z. Epub 2017 May 1 [PubMed PMID: 28457231]
Level 1 (high-level) evidenceFarmer SA, Grady KL, Wang E, McGee EC Jr, Cotts WG, McCarthy PM. Demographic, psychosocial, and behavioral factors associated with survival after heart transplantation. The Annals of thoracic surgery. 2013 Mar:95(3):876-83. doi: 10.1016/j.athoracsur.2012.11.041. Epub 2013 Jan 29 [PubMed PMID: 23374446]
Bart NK,Macdonald PS, Understanding Tricuspid Regurgitation Post Cardiac Transplantation; Why "Anatomical" and "Functional" Just Won [PubMed PMID: 37578343]
Level 3 (low-level) evidence