 Anatomy, Abdomen and Pelvis: Falciform Ligament
Anatomy, Abdomen and Pelvis: Falciform Ligament
Introduction
The falciform ligament is the thin, sickle-shaped, fibrous structure that connects the anterior part of the liver to the ventral wall of the abdomen. It can be seen drooping from the liver hilum when looking inside the abdomen during surgery. The falciform ligament attaches to the liver between the right and left lobes as well as attaching to the inferior diaphragmatic surface. The free, inferior border of the falciform ligament contains the paraumbilical veins and the round ligament of the liver (aka, ligamentum teres hepatis) which courses along a fissure situated between the inferior surface of the right and left lobes. Paraumbilical veins become prominent and more patent during portal hypertension when the portal vein, draining the gastrointestinal system, becomes engorged with blood which is unable to fully enter the liver. If the portal hypertension is severe enough, the paraumbilical veins will form a caput medusa of engorged blood vessels surrounding the umbilicus. The presence of a caput medusa is a stigmata of portal hypertension and severe liver dysfunction as seen in end-stage liver disease. (Note: When using the shorthand term of “round ligament” vs. “round ligament of the liver,” the term must not be confused with the round ligament of the uterus.)
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The falciform ligament is a double-layered extension of parietal peritoneum that sweeps off the anterior abdominal wall to divide the liver into the asymmetric left and right lobes. When looking at the ligament from a coronal view, the most distal aspect of the falciform ligament ends in a free edge containing the round ligament of the liver and the paraumbilical veins. The proximal portion will diverge to merge with the right and left coronary ligaments which surround the bare liver area which superimposes against the inferior diaphragmatic surface. The round ligament of the liver is the fetal remnant of the umbilical vein, which once traveled from the placenta to the fetal liver to deliver oxygenated blood.[1]
Embryology
The falciform ligament derives from the ventral mesentery, which is a part of the embryological foregut and forms a connection between the ventral abdominal wall and the liver. The umbilical vein, which is within the umbilical cord, carries oxygen-rich blood from the placenta to the fetal liver. Once the child is born, the umbilical vein degenerates because maternal-fetal circulation is no longer needed to sustain fetal life as the placenta is no longer intact. After birth, the umbilical vein remnant forms the round ligament of the liver, which in adults, contains paraumbilical veins.
Blood Supply and Lymphatics
The blood supply to the falciform ligament is variable but is generally supplied by the left inferior phrenic and/or middle hepatic arteries. The left inferior phrenic vein drains the falciform ligament. The superficial lymphatics of the liver drain the lymph from the falciform ligament. Because of its close association with the liver, it is possible to have infections and malignancies spread to the falciform ligament via its blood supply and/or lymphatics. The porta hepatis, which carries the neurovascular bundle containing the common hepatic duct, proper hepatic artery, hepatic portal vein, and autonomic axons into the liver, is located in a fissure on the inferior aspect of the far left side of the right lobe. Because of the proximity of the porta hepatis to the round ligament of the liver, infections or carcinomas in the porta hepatis can travel to the falciform ligament.[2] Additionally, the superficial lymphatics of the liver can carry infections or malignancies from surrounding structures and seed the falciform ligament.[3]
Nerves
No clinically important nerves have associations with the falciform ligament. However, like any vascular structure, postsynaptic sympathetic nerve fibers may be present.
Muscles
The falciform ligament contains no skeletal or smooth muscle fibers. However, it does share associations with surrounding skeletal musculature. The ligament is connected to the inferior surface of the thoracic diaphragm and runs along the posterior sheath of the right rectus abdominis muscle where it can reach as far caudally as the umbilicus.
Physiologic Variants
Physiologic variants of the falciform ligament are very rare. There have been a few case reports of obliteration of the falciform ligament where the liver appeared to lack the fissure the ligament usually creates. There have also been anatomic variants pertaining to structures carried in the falciform ligament, e.g., paraumbilical veins. However, most variants are not clinically significant and would most often be incidental findings during surgery or imaging used to help diagnose another condition.
Surgical Considerations
The falciform ligament serves as an anatomical landmark during abdominal surgery. The hepatic veins, which are hidden from view on the bare surface of the liver and drain into the inferior vena cava, are located immediately inferior to the falciform ligament. Additionally, the round ligament located in the free margin of the falciform ligament enters the umbilicus and serves as a significant landmark for the inner anterior abdominal wall. It also acts as an important landmark during gallbladder surgeries.
Clinical Significance
In patients with portal hypertension, the falciform ligament becomes recanalized with blood vessels. The venous congestion that occurs as a result of portal hypertension causes blood to shunt towards the anterior abdominal wall. Once blood starts pooling in the falciform ligament, periumbilical bruising will be evident. With increasing portal hypertension, caput medusae will present as a clinical feature resulting from engorged and distended superficial epigastric and periumbilical veins on the anterior surface of the abdomen. When one visualizes this feature, a diagnosis of portal hypertension should be suspected. Rarely, cysts may develop on the falciform ligament which may cause vague upper abdominal pain. A CT scan is the best means for assessment of falciform ligament pathology.
Other Issues
The falciform ligament is a cause of acute abdomen in select patients under various circumstances.[4] For instance, there have been case reports of falciform ligament necrosis.[5] Also, hematomas, abscesses, and lipomas have been documented.[6][7][8][9] By far, the most common issues that can occur with the falciform ligament include cysts, tumors, and engorgement due to portal hypertension from conditions such as cirrhosis, Budd-Chiari, and malignancy. Congenital defects can occur within the falciform ligament during the process of development that may predispose a person to internal hernias.[10]
Media
(Click Image to Enlarge)
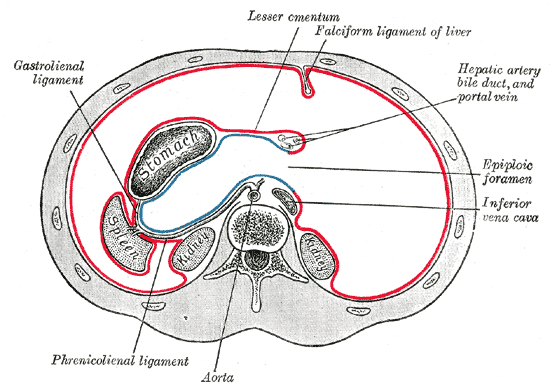
The Abdomen, Horizontal disposition of the peritoneum in the upper part of the abdomen, Phrenico Lienal ligament, Aorta, Inferior Vena cava, Epiploic foramen, Hepatic artery bile duct and portal vein, Falciform ligament of liver, Lesser omentum, Gastrolienal ligament
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
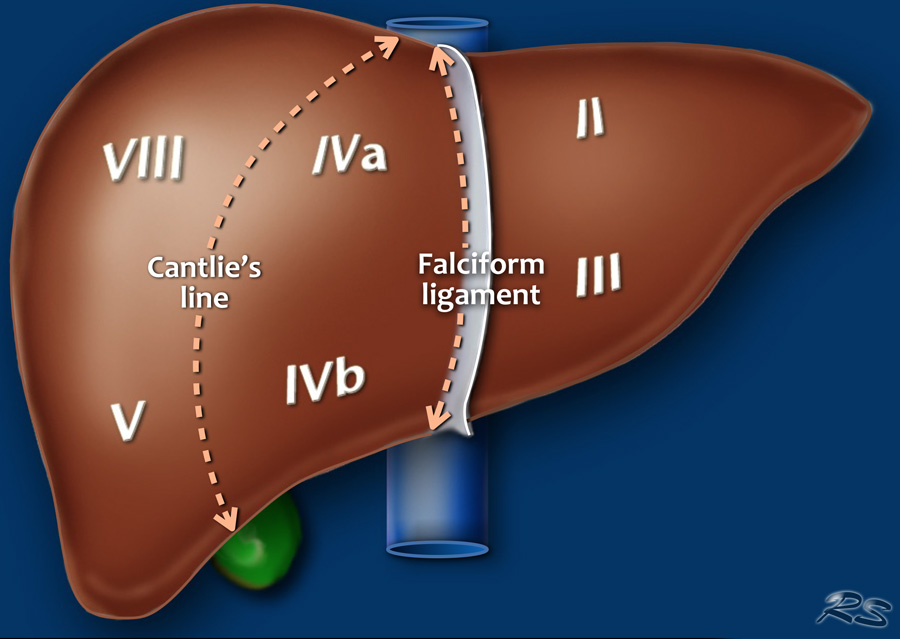
Couinaud system, Frontal view of the liver, the posteriorly located segments VI and VII are not visible, Cantlie's line, Falciform ligament Contribution by Robin Smithuis and the Radiology Assistant
References
Vernon H, Wehrle CJ, Alia VSK, Kasi A. Anatomy, Abdomen and Pelvis: Liver. StatPearls. 2023 Jan:(): [PubMed PMID: 29763190]
Solomon A, Rubinstein Z. Importance of the falciform ligament, ligamentum teres and splenic hilus in the spread of malignancy as demonstrated by computed tomography. Gastrointestinal radiology. 1984:9(1):53-6 [PubMed PMID: 6724241]
Warren LR, Chandrasegaram MD, Madigan DJ, Dolan PM, Neo EL, Worthley CS. Falciform ligament abscess from left sided portal pyaemia following malignant obstructive cholangitis. World journal of surgical oncology. 2012 Dec 22:10():278. doi: 10.1186/1477-7819-10-278. Epub 2012 Dec 22 [PubMed PMID: 23259725]
Level 3 (low-level) evidencePriola AM, Priola SM, Cataldi A, Marci V, Fava C. Acute abdomen as an unusual presentation of hepatic PEComa. A case report. Tumori. 2009 Jan-Feb:95(1):123-8 [PubMed PMID: 19366072]
Level 3 (low-level) evidenceSørensen J, Møller AM, Håkansson T. [Acute abdomen caused by necrosis of the falciform ligament of the liver]. Ugeskrift for laeger. 1983 Feb 21:145(8):583 [PubMed PMID: 6857822]
Level 3 (low-level) evidenceHonda H, Watanabe K, Mihara K, Hoshi H, Sakihama M. Lipoma of the hepatic falciform ligament. Journal of computer assisted tomography. 1983 Feb:7(1):170 [PubMed PMID: 6826846]
Level 3 (low-level) evidenceMoon SB, Lee HW, Park KW, Jung SE. Falciform ligament abscess after omphalitis: report of a case. Journal of Korean medical science. 2010 Jul:25(7):1090-2. doi: 10.3346/jkms.2010.25.7.1090. Epub 2010 Jun 16 [PubMed PMID: 20592906]
Level 3 (low-level) evidenceKakitsubata Y, Nakamura R, Shiba T, Sugimura H, Suzuki Y, Kakitsubata S, Watanabe K, Kawana T, Iwamura T. Lipoma of the falciform ligament: US, CT, and MRI appearances. Clinical imaging. 1993 Jan-Mar:17(1):27-9 [PubMed PMID: 8439840]
Level 3 (low-level) evidenceSari S, Ersöz F, Güneş ME, Paşaoğlu E, Arikan S. Hematoma of the falciform ligament: a rare cause of acute abdomen. The Turkish journal of gastroenterology : the official journal of Turkish Society of Gastroenterology. 2011:22(2):213-5 [PubMed PMID: 21796563]
Level 3 (low-level) evidenceSourtzis S, Canizares C, Thibeau JF, Philippart P, Damry N. An unusual case of herniation of small bowel through an iatrogenic defect of the falciform ligament. European radiology. 2002 Mar:12(3):531-3 [PubMed PMID: 11870465]
Level 3 (low-level) evidence