Introduction
Breast fat necrosis is nonviable adipose cells from injured or ischemic breast tissue that is replaced with scar tissue and presents as a palpable nodule. Breast fat necrosis has various etiologies and implications; therefore, a careful patient history is imperative to properly evaluate the patient. The most common etiology of fat necrosis is recent breast surgery; however, in non-operative patients, cancer or mechanical trauma to the breast tissue is often the culprit. Breast fat necrosis can be confusing on breast imaging with malignancy (it can mimic malignancy on radiologic studies, as well as clinical presentation). It can also be cosmetically undesirable. In this article, we will focus on breast fat necrosis in the surgical patient.
Anatomy
Three structures comprise the breast: skin, subcutaneous tissue, and breast tissue. The breast tissue contains both epithelial and stromal elements, the latter being both adipose and fibrous connective tissue. Stromal elements are responsible for the majority of breast volume during the non-lactating state.
The majority of the blood supply to the breast comes from the internal mammary artery perforators and the minority from the lateral thoracic artery perforators. This factor is essential, especially during breast reduction and/or reconstruction, where transection of vessels and subsequent relative ischemia can lead to breast fat necrosis.
Lymphatic drainage follows a unidirectional flow, from deep subcutaneous and intramammary vessels, towards axillary and internal mammary lymph nodes. Although the majority of the blood supply comes from the internal mammary artery, only 4% lymph flows go to internal mammary nodes, with the majority (97 percent) of the lymph flows to the axillary nodes.
Presentation
Fat necrosis can be diagnosed clinically or radiographically in the majority of cases, without the need for biopsy. In surgical patients who have recently undergone a breast surgical procedure such as breast reduction, reconstruction, implant removal, or fat grafting after primary reconstruction, the most common presentation is the finding of a palpable mass or lump under the breast skin. There is a predilection for the subareolar and periareolar regions, but it can occur anywhere. Detection through imaging without an obvious source, such as recent surgery or trauma, or when associated with findings such as lymphadenopathy or skin change, requires exclusion of malignancy.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Fat necrosis is most commonly the result of breast trauma (21 to 70%), fine needle aspiration or biopsy, anticoagulation treatment, radiation, and breast infection.[1] Individual patient factors such as smoking, obesity, and older age, as well as treatment associated with breast cancer (radiation, chemotherapy, and mastectomy), are specifically associated with an increase in breast fat necrosis.[2] Breast fat necrosis can have an association with any breast surgical procedure; however, it becomes the prime concern after mastectomy/reconstruction as fat necrosis can cause breast deformity or concern for cancer recurrence.
Free Flap
The free flap has gained favor for breast reconstruction after mastectomy over the past several decades. A flap a transfer of tissue with its blood supply from one part of the body to another. After a partial or total mastectomy, this process is autologous breast reconstruction, and this can be by pedicled or free tissue transfer. In pedicled tissue transfer, the blood supply is kept intact, and the tissue flap is tunneled or rotated to the recipient site. In a free flap, the vessels get disconnected during the transfer, thus making it "free," and then reconnected microsurgically to a new artery and vein at or near the recipient site. Deep inferior epigastric perforator flap (DIEP) is the current mainstream choice for breast free flap.
The creation of a flap is complex and requires a substantial level of training, planning, and surgical expertise. Many factors lead to fat necrosis in flap reconstruction. However, the cause of the problem is ischemia - either inadequate arterial inflow or poor venous outflow can cause ischemia and subsequent fat necrosis of the flap itself. Many studies have demonstrated the association of breast fat necrosis in free flap reconstruction with the number of perforators and flap weight.[3][4][5] This outcome is intuitive - as the ratio of blood supply to surface area increases, there is more perfusion to fat tissue and less chance of ischemia. Additionally, suggestions are that a greater amount of venous outflow with additional venous anastomoses decreases the incidence of breast fat necrosis.[6] Other factors shown to increase the incidence of breast fat necrosis in free flaps include smoking, pedicle caliber, type of flap, radiation, and surgeon's experience.[7][8][9][10][11] Many surgeons require patients to quit smoking 8 weeks prior to surgery.
Breast Reduction/ Lumpectomy
There are many techniques described to reduce breast size, based on incision and pedicle types. Breast reduction is also possible by liposuction alone, but that is mainly reserved for young women with high expected skin elasticity. The pedicle is the area of the adipose tissue supplied by one or many arterial perforators which branch into smaller capillaries. If blood supply is disrupted significantly, especially in distal areas of the pedicle and overlying skin, then fat necrosis can occur. The amount of breast tissue excised directly correlates to the complication rate.[12][13] The incidence of fat necrosis in breast reduction is found to be between 1 to 9%.[14][15][16] Tobacco smoking is a known independent factor in the increased risk for fat necrosis and other complications after breast reduction.[15]
Fat Grafting
Fat grafting is done by harvesting fat using liposuction from one part of the body and injecting it to another. Fat grafting can be especially useful in the management of contour deformity in breast reconstruction, known as a "step-off deformity," or the point where the breast reconstruction (implant or flap) transitions to the native chest wall. Additionally, fat grafting can improve surrounding skin quality after radiation or skin-sparing mastectomy, decrease implant visibility in a patient with minimal subcutaneous fat or minimal native breast tissue, and fill in defects caused by the excision of previous breast fat necrosis.
Fat necrosis is a commonly seen result after fat grafting, as the blood supply to fat grafted is random and acquired from surrounding tissues by diffusion and neovascularization. Although multiple fat grafting techniques have undergone evaluation, there is no consensus on superiority amongst them.[17][18] Regardless of the techniques, the reported rates of fat necrosis after fat grafting is between 2% and 18%.[19][20][21] No one variable such as age, body mass index, stage of malignancy, smoking, radiation, harvest site or technical variables (fat/tumescent volume, syringe aspiration vs. liposuction pump, cannula type or size) was found to predict the development of fat necrosis.[22][23] However, studies do show adipocyte destruction directly correlates with time spent ex vivo; therefore, lipotransfer should occur as promptly as possible after fat harvest.[24][22]
Mastectomy
Breast fat necrosis after mastectomy often occurs due to small amounts of adipose tissue without blood supply being left behind, causing ischemia-related necrosis. The mass is often palpable, and the differential diagnosis includes fat necrosis, fibrocystic disease, hematoma or seroma, suture or dermal calcifications, scar tissue, edema, abscess, and, more concerning, recurrent or new breast cancer.[25] Timing is important in the evaluation of these patients as local recurrence of malignancy tends to occur in the first 1 to 5 years after surgery, whereas most of these changes of fat necrosis happen within weeks to months after surgery.
Radiation Therapy
Flaps experience a higher rate of fat necrosis when irradiated. The rate of symptomatic fat necrosis in brachytherapy and now accelerated partial breast irradiation is found to be 1 to 50%.[26][27][28] The incidence is related to volume encompassed by the given dose of radiation or how much tissue was irradiated by the maximum strength of radiation prescribed.[29][30] There is some evidence that interstitial brachytherapy may cause additional trauma due to the implanted needle, causing an increased incidence of fat necrosis.[29] Studies have also shown an increase in breast fat necrosis with brachytherapy in populations who also received treatment with adriamycin-based chemotherapy.[30]
Epidemiology
The incidence of breast fat necrosis overall is roughly 0.6%, representing 2.75% of all benign lesions.[31] Fat necrosis presents in 0.8% of breast tumors and 1 to 9% of breast reduction surgery cases. Most at risk are middle-aged women, with an average age of 50 years, and women with pendulous breasts.[1]
Pathophysiology
Fat necrosis is a sterile, inflammatory process which results from aseptic saponification of fat employing blood and tissue lipase.[1] Lipase is an enzyme that releases fatty acids from triglycerides. These fatty acids form a complex with calcium to form saponification. The age of the lesion in fat necrosis dictates its appearance both grossly and microscopically.
Fat necrosis first appears as an area of hemorrhage in fat, which manifests as induration and firmness on gross pathology. Subsequently saponification occurs, where the lesion may become yellow, then calcification, which presents as a chalky white lesion, and lastly fibrosis, a yellow-gray mass. Scar formation is the result of reactive inflammatory components eventually replaced by fibrosis. Additionally, some adipose cells will release their contents instead of forming scars as a result of injury, and this is known as cystic degeneration. Calcifications frequently develop around the outer lining of the cyst. Fibrosis can surround degenerated fat or oil (known as "oil cyst"), which may persist for months or years.
Histopathology
Microscopic findings in breast fat necrosis are dependent on the age of the lesion. A newly insulted adipose cell will first lose its nucleus, which is then replaced by foamy histiocytes or macrophages filled with dead adipose cells in the process of debridement. Hemosiderin-laden macrophages may present as morphologic evidence of remote hemorrhage. Degranulation of histocytes activate interstitial infiltration of plasma cells, and eventually lymphocytes. Immunostaining may be used to rule out carcinoma, looking for the presence of CD68 and the absence of pan-cytokeratin, which confirms cells to be foamy histiocytes, diagnosing fat necrosis.
At lower magnification, necrotic material appears wrapped by a zone of fibrous tissue. Fibrosis, in turn, may lead to the formation of an irregular spiculated mass due to the retraction of nearby vascularized tissue within 2 to 4 weeks after breast surgery. Calcification surrounding these lesions may be noted in masses 6 to 12 months old. Areas of significant fibrosis may be associated with dysmorphic calcification, and these lesions may need further assessment to rule out malignancy.
History and Physical
History
A careful history is paramount to the diagnosis of breast fat necrosis. Although malignancy should always be in the differential, efforts should be made to spare the patient from the unnecessary emotional and financial burden of unnecessary procedures. Additionally, invasive work-up such as core biopsy can be detrimental to some patient populations such as those with irradiated breast, where a non-healing wound may develop.
- History of trauma (i.e., MVC in a person restrained by a seatbelt)
- History of breast surgery/reconstruction
- History of breast implant removal
- History of breast radiation
- Obesity with very large breasts
- Pendulous breasts
Physical Exam
Features associated with breast fat necrosis include an irregular breast mass, usually fixed to the dermis, with possible skin tethering and/or nipple retraction as a result of fibrotic bands between necrotic tissue and skin. These same characteristics can also be hallmark findings of malignancy, thus making it essential to consider all patient factors.
Evaluation
Once the surgeon finds a breat mass, he may reassure the patient or perform further evaluation. Essentially, the goal of the workup is to rule out breast cancer. The extent of the evaluation required to accomplish this goal varies based on the chief complaint, patient's age, and risk factors. Workup is as follows:
- A thorough breast examination
- A mammogram, +/-ultrasound, +/-MRI
- Fine needle aspiration or core biopsy or excisional biopsy
Mammographic Features
At mammography, fat necrosis may demonstrate the typical appearance of a cyst, which has a typical appearance of a smooth-bordered lucent mass. However, it is possible, based on the level of fibrosis, that fat necrosis will manifest as a cluster of pleomorphic microcalcifications, with areas of abnormal opacity, making it hard to differentiate from malignancy.[32]
Sonographic Features
Fat necrosis or oil cyst, when seen on ultrasound is a cystic lesion with echogenic internal bands, and its orientation is affected by the patient's body position. In non-cystic lesions including fat necrosis, common features include increased echogenicity of subcutaneous tissue (27%), anechoic cyst with posterior acoustic enhancement (17%), hypoechoic mass with posterior acoustic shadowing (16%), solid mass (14%), or normal appearance (11%).[1] Doppler ultrasound can also help make the diagnosis of fat necrosis and rule out malignancy by failing to demonstrate internal vascularity to the mass in question. Overall, ultrasound is less specific, and therefore, mammography is preferred when making the radiologic diagnosis of fat necrosis. However, it can still be a useful tool in ruling out malignancy.
MRI
MRI is used to differentiate breast fat necrosis from carcinoma when there is prnounced fibrosis, and the lesion presents as a spiculated infiltrative mass with or without microcalcification. MRI has been reported to have a negative predictive value approaching 100% in patients with a history of breast surgery.[33] Fat necrosis usually looks identical to adjacent fat on MRI, and there is no enhancement after IV contrast. The exception to that is enhancement seen up to 6 months from surgery in fresh granulation tissue, making MRI slightly less reliable. If that occurs, the use of fat suppression can aid in the differentiation from a tumor. Other MRI findings are signal void in areas of calcifications and architectural distortion in tissue fibrosis. The most common MRI finding in fat necrosis is a round or oval hypointense mass on T1-weighted signal on fat saturation images, confirming the presence of an oil cyst.
The presentations of breast necrosis vary on mammography, ultrasound, and MRI. In one study, however, it was found that diangosis of calcifications was best by mammography, oil cysts by ultrasound, and fibrotic fat necrosis by MRI.[34] Knowledge of the possibility of sonographic findings, along with mammographic features, may aid the clinician in determining whether further investigation is necessary.
Fine Needle Aspiration (FNA)
FNA has high sensitivity and specificity in diagnosing fat necrosis, offering an alternative to biopsy.[35] The cytology ranges from clumped fat lobules with opaque cytoplasm to necrotic aspirate with dispersed fat cells with opaque cytoplasm, foamy macrophages, multinucleated giant cells, lymphocytes, and neutrophils. However, sampling error and incomplete biopsy can be a problem, leading to repeat attempts. In combination with a reliable history such as trauma or recent surgery and close clinical follow-up, FNA is a good option.
Core biopsy
Core biopsy is more sensitive than FNA, and the accuracy of a large-bore core biopsy is said to be comparable to excisional biopsy for diagnosis of fat necrosis in low-risk patients.[36] However, if the radiologic findings strongly support fat necrosis, then the biopsy can be avoided altogether. Core biopsy has been shown to have a slightly higher rate of false negative results in high-risk patients, and excisional biopsy may be needed to confirm fat necrosis.
Excisional Biopsy
If suspicion for malignancy is high, and core biopsy is negative, excisional biopsy is the next diagnostic step.
Treatment / Management
Palpable areas of fat necrosis may enlarge, remain unchanged, regress, or resolve. It usually does not necessitate any surgical treatment, and clinical follow-up is sufficient in the patient population in which pain is not present, and cosmesis is not the primary concern. However, if fat necrosis is confirmed, and it does not resolve and/or it causes pain or distortion in the breast shape, surgical removal is an option. As far as mammography is concerned, a lesion classified as "benign" by mammogram may undergo yearly surveillance. A finding of "most likely benign" can be followed up in 6 months with a mammogram, and a biopsy is a next step if "malignancy suspected."
If the fat necrosis contains oily fluid, it may need to be aspirated using a needle to relieve any patient discomfort. In the case of a solid mass and/or breast distortion, treatment options depend on the size of the anticipated defect after excision. A small defect may be addressed with either excision alone or excision with fat grafting and/or local tissue rearrangement. For a large defect such as those due to partial flap loss after reconstruction, a more significant tissue debridement and reconstruction may be necessary. In those cases, the patient may opt for a secondary free flap or other tissue transfer, convert to tissue expanders or breast implants to increase volume, or undergo a contralateral symmetry procedure to achieve symmetry.
Differential Diagnosis
The following conditions can be mistaken for breast fat necrosis:
- Breast carcinoma
- Tuberculosis of breast
- Fibroadenoma
- Phyllodes tumor
- Breast cyst
Breast fat necrosis can closely mimic breast cancer in both physical examination and imaging. Therefore, it is crucial to take a detailed history, assess risk factors, and consider the age of the patient. In high-risk patients, namely, those whose primary surgery was oncologic, patients older than 40 years of age, and those with very delayed presentation of fat necrosis, a more extensive workup is necessary. It is important not to assume the diagnosis of fat necrosis when history includes breast trauma, as trauma could mask or distract from a pre-existing breast mass.
Prognosis
The main concern associated with the diagnosis of breast fat necrosis is the similarity in presentation, both clinical and radiologic, to malignancy. Fortunately, breast fat necrosis is a benign process with an excellent prognosis. It does not increase the risk of future breast cancer development in any way.
Complications
Breast fat necrosis can occur early in the post-operative period or have a delayed presentation. Complications related to breast fat necrosis include pain, infection, need for multiple operations, and breast deformity. These complications can exert a profound effect on the patient, both physically and emotionally. Therefore, these are risks that should be discussed with the patient pre-operatively. There is no known risk for transformation to malignancy.
Deterrence and Patient Education
Education involving patients and the public in general, as well as health care providers, is necessary not only to provide the best patient outcomes according to evidence-based medicine but also to assure that patients have realistic expectations. These resources may include:
1. The American Society of Plastic Surgeons website
2. American College of Surgeons website
3. BreastCancer.org: Fat Necrosis in the Tissue Flap
Enhancing Healthcare Team Outcomes
An interprofessional team that provides a holistic and integrated approach to postoperative care can help achieve the best possible outcomes in the inpatient and outpatient setting. It is essential to train the care team how to detect signs and symptoms of flap ischemia in the immediate postoperative period and how to relay this message. A prompt return to the operating room might prevent breast fat necrosis and possible total flap loss. The patient can also present with delayed flap ischemia, and that is often due to a lack of understanding of physical activity restrictions post-operatively. Educational handouts and various teaching strategies are useful in an attempt to educate patients and families about the post-operative period. However, changes can often be made to improve compliance. Collaboration, shared decision making, and communication are key elements for a good outcome in this patient population, as restrictions given a patient such as "do not pick up your toddler" or "stop smoking" may not be a realistic option. Health care providers must listen to their patients and provide them with an option with which they might be able to comply, enhancing patient-centered care, and also improving outcomes.
Breast fat necrosis can be found immediately in the postoperative period or months after surgery or breast trauma. With inpatients, it is important to not only treat the symptoms of the patient but to keep in mind the emotional burden that a flap loss or breast deformity might cause. Such complications can require a patient to have multiple trips to the operating room. In the outpatient setting, it is important for all providers in the care team to recognize risk factors and address the patient's concerns. Reassurance and close clinical follow-up are necessary when caring for the patient with breast fat necrosis.
Most importantly, a thorough informed consent should be part of the pre-operative visit. This discussion would include the general risks associated with any surgery, but it should also encompass possible outcomes and complications specific to breast surgery. A patient's recollection and understanding of informed consent can often be lacking, particularly with the anxiety and emotion associated with breast surgery. Therefore, with breast surgery, it is essential to consider adding to the informed consent a discussion of the risk of fat necrosis, hypertrophic scar formation, asymmetry, loss of sensitivity/numbness, cosmetic deformity, skin necrosis, and/or and flap loss, all which could result to a return to the operating room. Additionally, it is essential to mention how the healthcare team will address these complications; this not only makes for a more complete informed consent, but it also may result in better ultimate patient satisfaction and experience with these outcomes.
Media
(Click Image to Enlarge)
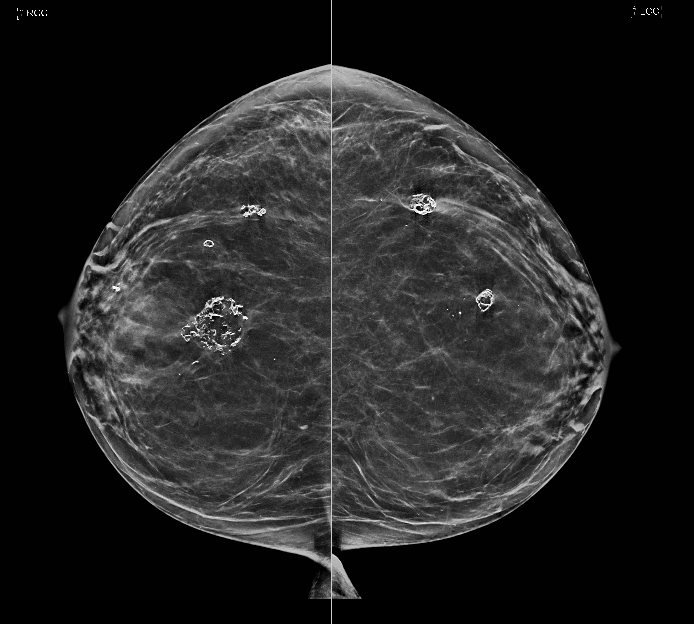
Benign breast calcification: Dystrophic calcifications from fat necrosis are seen within both breasts. Contributed by Brooke Bell, MD
References
Tan PH, Lai LM, Carrington EV, Opaluwa AS, Ravikumar KH, Chetty N, Kaplan V, Kelley CJ, Babu ED. Fat necrosis of the breast--a review. Breast (Edinburgh, Scotland). 2006 Jun:15(3):313-8 [PubMed PMID: 16198567]
Level 1 (high-level) evidenceSelber JC, Kurichi JE, Vega SJ, Sonnad SS, Serletti JM. Risk factors and complications in free TRAM flap breast reconstruction. Annals of plastic surgery. 2006 May:56(5):492-7 [PubMed PMID: 16641623]
Level 2 (mid-level) evidenceBaumann DP, Lin HY, Chevray PM. Perforator number predicts fat necrosis in a prospective analysis of breast reconstruction with free TRAM, DIEP, and SIEA flaps. Plastic and reconstructive surgery. 2010 May:125(5):1335-1341. doi: 10.1097/PRS.0b013e3181d4fb4a. Epub [PubMed PMID: 20440154]
Sailon AM,Schachar JS,Levine JP, Free transverse rectus abdominis myocutaneous and deep inferior epigastric perforator flaps for breast reconstruction: a systematic review of flap complication rates and donor-site morbidity. Annals of plastic surgery. 2009 May; [PubMed PMID: 19387162]
Level 1 (high-level) evidenceKroll SS. Fat necrosis in free transverse rectus abdominis myocutaneous and deep inferior epigastric perforator flaps. Plastic and reconstructive surgery. 2000 Sep:106(3):576-83 [PubMed PMID: 10987463]
Ochoa O, Pisano S, Chrysopoulo M, Ledoux P, Arishita G, Nastala C. Salvage of intraoperative deep inferior epigastric perforator flap venous congestion with augmentation of venous outflow: flap morbidity and review of the literature. Plastic and reconstructive surgery. Global open. 2013 Oct:1(7):e52. doi: 10.1097/GOX.0b013e3182aa8736. Epub 2013 Nov 7 [PubMed PMID: 25289247]
Kaidar-Person O, Eblan MJ, Caster JM, Shah AR, Fried D, Marks LB, Lee CN, Jones EL. Effect of internal mammary vessels radiation dose on outcomes of free flap breast reconstruction. The breast journal. 2019 Mar:25(2):286-289. doi: 10.1111/tbj.13202. Epub 2019 Feb 8 [PubMed PMID: 30734417]
Sbitany H, Lentz R, Piper M. The "Dual-Plane" DIEP Flap: Measuring the Effects of Superficial Arterial and Venous Flow Augmentation on Clinical Outcomes. Journal of reconstructive microsurgery. 2019 Jul:35(6):411-416. doi: 10.1055/s-0038-1677013. Epub 2019 Jan 7 [PubMed PMID: 30616244]
Hembd A, Teotia SS, Zhu H, Haddock NT. Optimizing Perforator Selection: A Multivariable Analysis of Predictors for Fat Necrosis and Abdominal Morbidity in DIEP Flap Breast Reconstruction. Plastic and reconstructive surgery. 2018 Sep:142(3):583-592. doi: 10.1097/PRS.0000000000004631. Epub [PubMed PMID: 29878999]
Shechter S, Arad E, Inbal A, Friedman O, Gur E, Barnea Y. DIEP Flap Breast Reconstruction Complication Rate in Previously Irradiated Internal Mammary Nodes. Journal of reconstructive microsurgery. 2018 Jul:34(6):399-403. doi: 10.1055/s-0038-1625986. Epub 2018 Apr 19 [PubMed PMID: 29672777]
Chang EI, Chang EI, Soto-Miranda MA, Zhang H, Nosrati N, Ghali S, Chang DW. Evolution of Bilateral Free Flap Breast Reconstruction over 10 Years: Optimizing Outcomes and Comparison to Unilateral Reconstruction. Plastic and reconstructive surgery. 2015 Jun:135(6):946e-953e. doi: 10.1097/PRS.0000000000001233. Epub [PubMed PMID: 26017610]
Shestak KC, Davidson EH. Assessing Risk and Avoiding Complications in Breast Reduction. Clinics in plastic surgery. 2016 Apr:43(2):323-31. doi: 10.1016/j.cps.2015.12.007. Epub 2016 Feb 2 [PubMed PMID: 27012790]
Lewin R, Göransson M, Elander A, Thorarinsson A, Lundberg J, Lidén M. Risk factors for complications after breast reduction surgery. Journal of plastic surgery and hand surgery. 2014 Feb:48(1):10-4. doi: 10.3109/2000656X.2013.791625. Epub 2013 Apr 29 [PubMed PMID: 23627557]
Ogunleye AA, Leroux O, Morrison N, Preminger AB. Complications After Reduction Mammaplasty: A Comparison of Wise Pattern/Inferior Pedicle and Vertical Scar/Superomedial Pedicle. Annals of plastic surgery. 2017 Jul:79(1):13-16. doi: 10.1097/SAP.0000000000001059. Epub [PubMed PMID: 28328638]
Uslu A, Korkmaz MA, Surucu A, Karaveli A, Sahin C, Ataman MG. Breast Reduction Using the Superomedial Pedicle- and Septal Perforator-Based Technique: Our Clinical Experience. Aesthetic plastic surgery. 2019 Feb:43(1):27-35. doi: 10.1007/s00266-018-1177-z. Epub 2018 Jun 14 [PubMed PMID: 29948104]
Manahan MA, Buretta KJ, Chang D, Mithani SK, Mallalieu J, Shermak MA. An outcomes analysis of 2142 breast reduction procedures. Annals of plastic surgery. 2015 Mar:74(3):289-92. doi: 10.1097/SAP.0b013e31829d2261. Epub [PubMed PMID: 25668497]
Level 2 (mid-level) evidenceGutowski KA, ASPS Fat Graft Task Force. Current applications and safety of autologous fat grafts: a report of the ASPS fat graft task force. Plastic and reconstructive surgery. 2009 Jul:124(1):272-280. doi: 10.1097/PRS.0b013e3181a09506. Epub [PubMed PMID: 19346997]
Sinno S, Wilson S, Brownstone N, Levine SM. Current Thoughts on Fat Grafting: Using the Evidence to Determine Fact or Fiction. Plastic and reconstructive surgery. 2016 Mar:137(3):818-824. doi: 10.1097/01.prs.0000479966.52477.8b. Epub [PubMed PMID: 26910662]
Spear SL, Wilson HB, Lockwood MD. Fat injection to correct contour deformities in the reconstructed breast. Plastic and reconstructive surgery. 2005 Oct:116(5):1300-5 [PubMed PMID: 16217471]
Level 2 (mid-level) evidenceColeman SR, Saboeiro AP. Fat grafting to the breast revisited: safety and efficacy. Plastic and reconstructive surgery. 2007 Mar:119(3):775-85; discussion 786-7 [PubMed PMID: 17312477]
Level 3 (low-level) evidenceDelay E, Garson S, Tousson G, Sinna R. Fat injection to the breast: technique, results, and indications based on 880 procedures over 10 years. Aesthetic surgery journal. 2009 Sep-Oct:29(5):360-76. doi: 10.1016/j.asj.2009.08.010. Epub [PubMed PMID: 19825464]
Doren EL, Parikh RP, Laronga C, Hiro ME, Sun W, Lee MC, Smith PD, Fulp WJ. Sequelae of fat grafting postmastectomy: an algorithm for management of fat necrosis. Eplasty. 2012:12():e53 [PubMed PMID: 23308300]
Smith P, Adams WP Jr, Lipschitz AH, Chau B, Sorokin E, Rohrich RJ, Brown SA. Autologous human fat grafting: effect of harvesting and preparation techniques on adipocyte graft survival. Plastic and reconstructive surgery. 2006 May:117(6):1836-44 [PubMed PMID: 16651956]
Level 3 (low-level) evidenceMatsumoto D, Shigeura T, Sato K, Inoue K, Suga H, Kato H, Aoi N, Murase S, Gonda K, Yoshimura K. Influences of preservation at various temperatures on liposuction aspirates. Plastic and reconstructive surgery. 2007 Nov:120(6):1510-1517. doi: 10.1097/01.prs.0000288015.70922.e4. Epub [PubMed PMID: 18040181]
Scaranelo AM, Lord B, Eiada R, Hofer SO. Imaging approaches and findings in the reconstructed breast: a pictorial essay. Canadian Association of Radiologists journal = Journal l'Association canadienne des radiologistes. 2011 Feb:62(1):60-72. doi: 10.1016/j.carj.2010.09.010. Epub 2010 Nov 10 [PubMed PMID: 21067890]
Garsa AA, Ferraro DJ, Dewees T, Margenthaler JA, Naughton M, Aft R, Gillanders WE, Eberlein T, Matesa MA, Zoberi I. Analysis of fat necrosis after adjuvant high-dose-rate interstitial brachytherapy for early stage breast cancer. Brachytherapy. 2013 Mar-Apr:12(2):99-106. doi: 10.1016/j.brachy.2012.04.005. Epub 2012 Jun 20 [PubMed PMID: 22726878]
Thomas MA, Ochoa LL, Zygmunt TM, Matesa M, Altman MB, Garcia-Ramirez JL, Esthappan J, Zoberi I. Accelerated Partial Breast Irradiation: A Safe, Effective, and Convenient Early Breast Cancer Treatment Option. Missouri medicine. 2015 Sep-Oct:112(5):379-84 [PubMed PMID: 26606820]
Russo AL, Taghian AG. Fat necrosis of the breast in the accelerated partial breast irradiation era: the need for a universal grading system. Breast cancer research and treatment. 2013 Jul:140(1):1-11 [PubMed PMID: 23797180]
Lövey K, Fodor J, Major T, Szabó E, Orosz Z, Sulyok Z, Jánváry L, Fröhlich G, Kásler M, Polgár C. Fat necrosis after partial-breast irradiation with brachytherapy or electron irradiation versus standard whole-breast radiotherapy--4-year results of a randomized trial. International journal of radiation oncology, biology, physics. 2007 Nov 1:69(3):724-31 [PubMed PMID: 17524571]
Level 1 (high-level) evidenceWazer DE, Kaufman S, Cuttino L, DiPetrillo T, Arthur DW. Accelerated partial breast irradiation: an analysis of variables associated with late toxicity and long-term cosmetic outcome after high-dose-rate interstitial brachytherapy. International journal of radiation oncology, biology, physics. 2006 Feb 1:64(2):489-95 [PubMed PMID: 16246495]
Kerridge WD, Kryvenko ON, Thompson A, Shah BA. Fat Necrosis of the Breast: A Pictorial Review of the Mammographic, Ultrasound, CT, and MRI Findings with Histopathologic Correlation. Radiology research and practice. 2015:2015():613139. doi: 10.1155/2015/613139. Epub 2015 Mar 16 [PubMed PMID: 25861475]
Hogge JP, Robinson RE, Magnant CM, Zuurbier RA. The mammographic spectrum of fat necrosis of the breast. Radiographics : a review publication of the Radiological Society of North America, Inc. 1995 Nov:15(6):1347-56 [PubMed PMID: 8577961]
Hassan HHM, El Abd AM, Abdel Bary A, Naguib NNN. Fat Necrosis of the Breast: Magnetic Resonance Imaging Characteristics and Pathologic Correlation. Academic radiology. 2018 Aug:25(8):985-992. doi: 10.1016/j.acra.2017.12.019. Epub 2018 Feb 13 [PubMed PMID: 29426684]
Shida M, Chiba A, Ohashi M, Yamakawa M. Ultrasound Diagnosis and Treatment of Breast Lumps after Breast Augmentation with Autologous Fat Grafting. Plastic and reconstructive surgery. Global open. 2017 Dec:5(12):e1603. doi: 10.1097/GOX.0000000000001603. Epub 2017 Dec 1 [PubMed PMID: 29632782]
Brown LA, Coghill SB. Fine needle aspiration cytology of the breast: factors affecting sensitivity. Cytopathology : official journal of the British Society for Clinical Cytology. 1991:2(2):67-74 [PubMed PMID: 1912363]
Parker SH, Burbank F, Jackman RJ, Aucreman CJ, Cardenosa G, Cink TM, Coscia JL Jr, Eklund GW, Evans WP 3rd, Garver PR. Percutaneous large-core breast biopsy: a multi-institutional study. Radiology. 1994 Nov:193(2):359-64 [PubMed PMID: 7972743]
Level 2 (mid-level) evidence