Introduction
Non-alcoholic Fatty Liver Disease (NAFLD) or "Fatty Liver" corresponds to the presence of macrovesicular changes without inflammation (steatosis) and lobular inflammation in the absence of significant alcohol use. It can be divided into two subgroups: NAFL (Non-Alcoholic Fatty Liver) or simply Steatosis and NASH (Non-Alcoholic Steatohepatitis). NAFL is defined as the presence of hepatic steatosis with no evidence of hepatocellular injury in the form of ballooning of the hepatocytes. NASH is defined as the presence of hepatic steatosis and inflammation with hepatocyte injury (ballooning), Malloryhyaline, and mixed lymphocytic and neutrophilic inflammatory infiltrate in perivenular areas with or without fibrosis.[1] It is important to note that NAFL is a spectrum, with NAFL being the mildest form and NASH and cirrhosis being at the other end of the spectrum. NAFL (Non-Alcoholic Fatty Liver) or simply Steatosis and NASH (Non-Alcoholic Steatohepatitis) could only be distingueshed with histology and liver biopsy.[2].
NAFLD is commonly associated with Metabolic Syndrome, obesity, diabetes, and hyperlipidemia. Nearly 80% of patients with Metabolic Syndrome have NAFLD.[3][4][5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Fat accumulates in the liver for several reasons. Most commonly, it involves increased delivery of free fatty acids (FFAs) to the liver, increased synthesis of fatty acids in the liver, decreased oxidation of FFA, or decreased synthesis or secretion of very-low-density lipoprotein (VLDL).[6][7]
Oxidative stress in the hepatocytes can activate stellate cells and lead to the production of collagen and inflammation.
Other factors that may contribute to fatty liver include:
- The use of medications (e.g., tamoxifen, amiodarone, methotrexate)
- Metabolic abnormalities (e.g., glycogen storage disorders, homocystinuria)
- Alcohol
- Nutritional status (e.g., total parenteral nutrition, severe malnutrition, overnutrition, or a starvation diet)
- Other health issues like Wilson disease and celiac sprue.
Epidemiology
The prevalence of NAFLD varies dramatically depending on the population being studied. It is estimated that the prevalence of NAFLD is in the range of 20% in the United States population and between 11.5% and 46% in the general population. By contrast, the prevalence of NASH is in the range of 2% and 3%. The prevalence is higher in white men than white women but therare are no differences between hispanic and African-American people[8]. Mean age at diagnosis is 50 years (range 16-80). It is more common in Hispanics when compared to Whites and more common in Whites than in Blacks.
Obesity is a well-known risk factor for NAFLD. In patients with severe obesity undergoing bariatric surgery, up to 90% are found to have NAFLD and some even have cirrhosis. The same study also concluded that insulin resistance was the main predictor for NASH.[9]
Pathophysiology
Current concepts point to insulin resistance as the primary metabolic defect leading to NAFLD. Insulin resistance leads to an increased influx of free fatty acids (FFA) into the liver. This happens due to the failure of insulin to suppress the hormone-sensitive lipase, causing more FFA to be released from the adipose tissue. Also, elevated insulin levels and insulin resistance promote continuous synthesis of triglycerides in the liver. These two sources of triglycerides result in accumulation of lipids in the hepatocytes causing macrovesicular hepatic steatosis (see Image. Liver Biopsy, Hepatic Steatosis).[6][10]
Lipid accumulation in non adipose tissue is a key factor for the progression of insulin resistance, DM(Diabetes mellitus) and cardiovascular disease.[11]
The current hypothesis is that NASH is an evolution from NAFLD caused by a second "hit." The evidence behind this second insult in not conclusive, but the most acceptable theories involve oxidative stress, specific cytokines, plus lipopolysaccharides. Free fatty acids and hyperinsulinemia potentiate lipid peroxidation and the release of hydroxy-free radicals, directly injuring the hepatocytes by recruiting neuroinflammatory mediators. Chronic liver injury over time will lead to activation of stellate cells, creating a potential for hepatic fibrosis.
The diagnosis of NASH can only be established with liver biopsy.
Biopsy findings can reveal the following.
- Type 1: fatty liver alone; macrovesicular steatosis
- Type 2: fatty accumulation and lobar inflammation
- Type 3: fat accumulation and ballooning degeneration
- Type 4: fat accumulation, ballooning degeneration and either Mallory hyaline of fibrosis.
Type 3 and Type 4 are NASH by definition.
Histopathology
Histologically, the fatty liver will reveal fat accumulation chiefly in the pericentral (centrilobular) zone. Universally one will note the presence of macrovesicular steatosis with the liver cells containing several large fat droplets which displace the nucleus. Sometimes the lipid deposits may be released due to rupture of the overtly distended liver cells and produce lipogranulomas, which are composed chiefly of macrophages and occasional lymphocytes.[12] See Image. Fatty Liver Disease.
History and Physical
Patients are usually asymptomatic, and "fatty liver" is usually an incidental finding on imaging done for other purposes. When patients do have symptoms, they are usually nonspecific, constitutional or right upper quadrant discomfort.
It is important to obtain detailed alcohol use, review past medical history, family history, current and past prescription medications, and use of over-the-counter drugs or supplements. The history should include diet, physical activity, change in weight ( weight gain more than 18 kg in 2-3 years) and evaluation for associated conditions like obesity, hyperlipidemia, and diabetes ).[13]
Evaluation
Laboratory studies lack specificity and cannot distinguish NASH from NAFLD; however, initial evaluation should include an assessment of a complete hepatic panel, lipid panel, and iron. Lab tests may be used to evaluate insuline resistane which include Homeostasis Model Assessment (normal value<3.99)[14] and The Quantitative Insulin Sensitivity Check Index [15]. labtests to rule out viral hepatitis and Hemochromatosis should be ordered. If the patient has elevated liver enzymes chronically or has family history of cirrohsis, additional tests should be considered like antinuclear antibody, smooth muscle antibody,a1-antitrypsin, ceruloplasmin and thyroid-stimulating hormone levels.[16][13]
patients with alcoholic-liver disease may have or have not elevated serum aminotransferase levels. The absolute level of liver enzyme elevation does not related to the severity of alcohol liver disease but the pattern of elevation in liver enzymes is helpful in making a diagnosis alcoholic liver disease. AST level is typically two to three times greater than ALT in alcoholic liver injury. Also, these patients have an elevated serum gamma-glutamyltranspeptidase (GGT).[17]
Imaging studies play a key role in the diagnosis of NAFLD. The mainstay is ultrasonography; it is least invasive, and relatively inexpensive. The sensitivity for an ultrasound to detect NAFLD is in the range of 60% to 90% with a specificity around 90%. Unenhanced abdominal computed tomography and magnetic resonance are alternatives but are more costly and are not significantly superior to ultrasonography.[18][3][19]
Diagnosis of NASH requires a liver biopsy; however, not all patients with NAFLD require a liver biopsy. The decision to proceed with histological examination depends on risk factors, laboratory workup, and disease severity. According to the 2012 guidelines from American Association for the Study of Liver Disease (AASLD), liver biopsy should be reserved for subjects who will 'benefit,' for subjects with potentially competing diagnosis, and for children with either an unclear diagnosis or in whom consideration is being given for medication.
Liver biopsy has moderate risk of complicationsand is invasive, subject to sampling error and is expensive.[20]
Treatment / Management
Lifestyle modifications and weight loss are the mainstays of the treatment. Treatment also involves glycemic and lipid control. For patients with significant obesity, gastric bypass or other weight loss surgical modalities should be considered. Weight loss is proven to reduce hepatic steatosis. Evidence available suggests that loss of 3% to 5% of body weight is necessary to notice an improvement in steatosis, but a greater loss (up to 10%) is necessary to improve necroinflammation. [21][22][23](A1)
Patients should abstain from alcohol or hepatotoxic drugs.
Pharmacological options include Metformin, Vitamin E, fish oil, Orlistat (an inhibitor of gastric and pancreatic lipase), and Sibutramine. It is important to notice that the evidence behind these pharmacological modalities is weak. Three Cochrane reviews found insufficient evidence to support the use of bile acids (ursodeoxycholic acid) antioxidant supplements, metformin or thiazolidinedione in the absence of diabetes in patients with non alcoholic fatty liver disease. [24][25]Studies have shown that metformin has no significant effect on liver histology; therefore, its use is only recommended if there is another indication for it. Vitamin E is currently only recommended for non-diabetic patients with biopsy-proven NASH. Pioglitazone can be used to treat patients with biopsy-proven steatohepatitis, but its long-term effects are not known. A randomized controlled trial of 247 adults with nonalcoholic steatohepatitis found improvement in AST and ALT levels with the use of vitamin E and pioglitazone but no improvement in fibrosis.[26](A1)
For patients with advanced disease and cirrhosis, liver transplantation might have to be considered.
Differential Diagnosis
- Viral Hepatitis
- Alcoholic hepatitis
- Alpha1 Antitrypsin Deficiency
- Primary sclerosing cholangitis
- Wilson disease
- Primary biliary cholangitis
- Cirrhosis
Prognosis
patients with NAFL (Non-alcoholic fatty liver disease )have 26 % higher health care cost in five year follow up.[27]
Complications
- Cirrhosis
- Ascites
- Esophageal varices
- Liver failure
- Liver cancer
- Type 2 diabetes
Postoperative and Rehabilitation Care
- Patients should be tested for other causes of liver injury like hepatitis B and offer vaccination
- All drugs that affect the liver must be discontinued
- The disease progression should be monitored for signs of liver dysfunction like ascites, palmar erythema, decreasing levels of albumin and elevated levels of INR.
- Levels of blood alcohol should be checked regularly to check for abstinence from alcohol.
- Patients with end-stage liver disease should be screened for liver cancer and gastroesophageal varices.
Consultations
- General and bariatric surgeon
- Radiologist for TIPS
- Gastroenterologist
Deterrence and Patient Education
- The patient should refrain from alcohol
- Malnutrition is common in these patients and a dietary consult should be obtained. A low-fat diet and weight loss is recommended.
- Participating in a regular exercise program is highly recommended.
Pearls and Other Issues
Although the overall risk of cirrhosis due to NAFLD is modest, certain groups are at particular risk. Important risk factors for NASH are obesity, diabetes, and advanced age.
Enhancing Healthcare Team Outcomes
Fatty liver is on the rise in the US primarily because of an increase in obesity, type 2 diabetes, and consumption of alcohol. The condition can be reversed if detected early but it requires an interprofessional approach.
Education of the patient is vital to ensure that there is complete abstinence from alcohol. For those who do not remain compliant, end-stage liver disease can develop which carries a high morbidity and mortality.
The nurse should also emphasize the importance of lifestyle changes and a healthy diet. Exercise and a healthy weight can help reverse the disorder and markedly improve the quality of life.
The pharmacist must be closely involved in the management of these patients because several studies show that the use of oral hypoglycemics and lipid-lowering agents may be helpful by lowering the risk of heart disease.
For patients who are not able to lose weight with conservative measures, a bariatric surgery consult may be helpful. There is evidence showing that appropriate weight loss surgery can significantly lower the risk of diabetes and heart disease.[21][28] (Level II)
Outcomes
Several studies show that if there is early intervention before the onset of fibrosis, the prognosis is excellent. However, if the treatment is delayed, and end-stage liver disease develops, the prognosis is poor. In order to reduce the morbidity of fatty liver, evidence suggests that one should adopt an aggressive an interprofessional strategy for managing obesity, diabetes, and the metabolic syndrome.[29][12][30] (Level V)
Media
(Click Image to Enlarge)
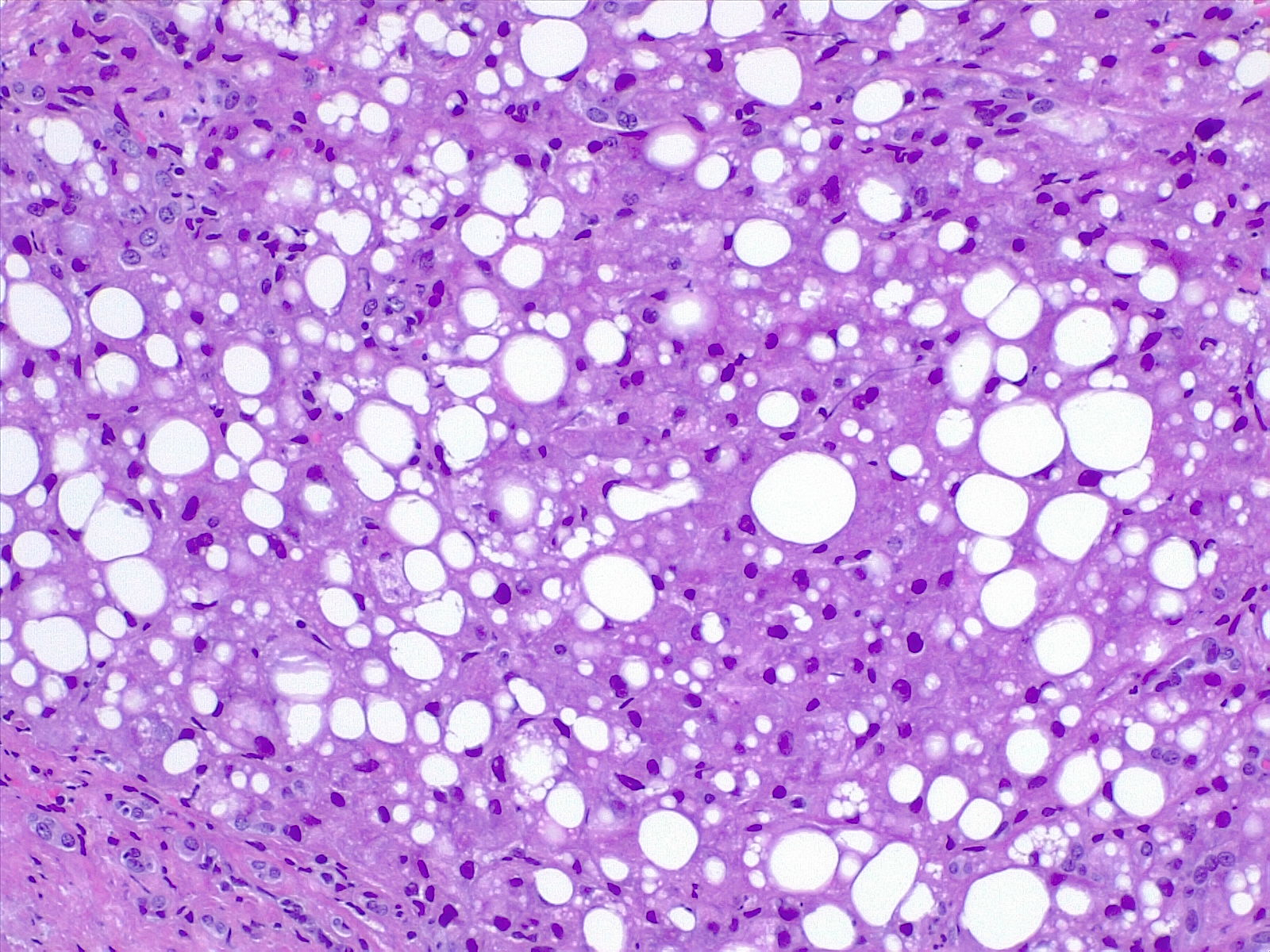
Fatty Liver Disease. Steatosis seen histologically as lipidic droplets (microvescicular) or a large intracytoplasmic vacuole (macrovescicular). Steatosis is quantified as a percentage of altered hepatocytes in all fields.
Contributed by F Farci, MD
(Click Image to Enlarge)
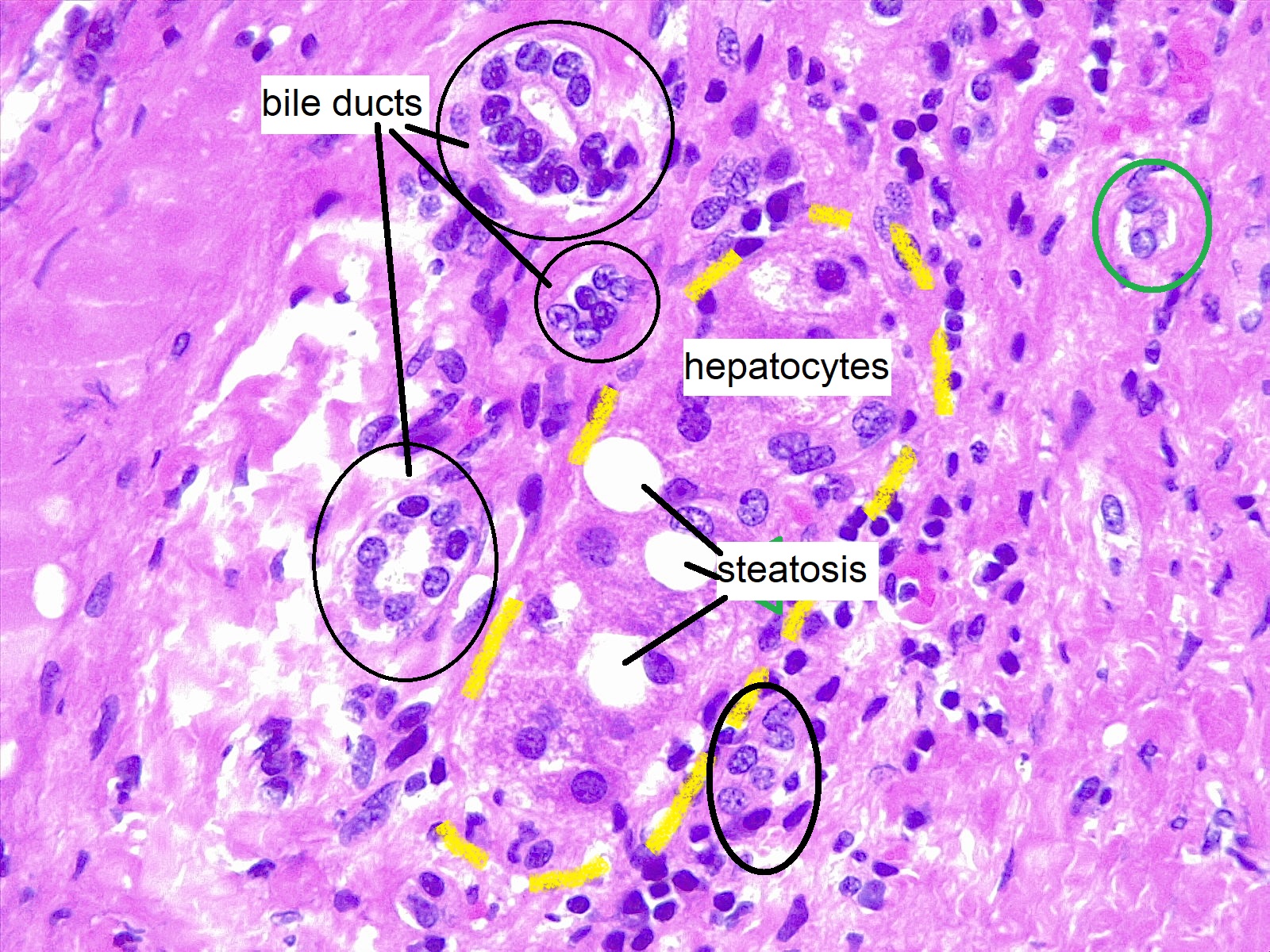
Liver Biopsy, Hepatic Steatosis. In this field, a group of hepatocytes (yellow dashes) is trapped in an altered portal tract due to long-standing hepatitis. Bile ducts are fragmented and multiple. Most of the small cells surrounding the portal tract are lymphocytes.
Contributed by F Farci, MD
References
Brunt EM, Janney CG, Di Bisceglie AM, Neuschwander-Tetri BA, Bacon BR. Nonalcoholic steatohepatitis: a proposal for grading and staging the histological lesions. The American journal of gastroenterology. 1999 Sep:94(9):2467-74 [PubMed PMID: 10484010]
Level 2 (mid-level) evidenceWilkins T, Tadkod A, Hepburn I, Schade RR. Nonalcoholic fatty liver disease: diagnosis and management. American family physician. 2013 Jul 1:88(1):35-42 [PubMed PMID: 23939604]
Leoni S, Tovoli F, Napoli L, Serio I, Ferri S, Bolondi L. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World journal of gastroenterology. 2018 Aug 14:24(30):3361-3373. doi: 10.3748/wjg.v24.i30.3361. Epub [PubMed PMID: 30122876]
Level 2 (mid-level) evidenceSchiavo L,Busetto L,Cesaretti M,Zelber-Sagi S,Deutsch L,Iannelli A, Nutritional issues in patients with obesity and cirrhosis. World journal of gastroenterology. 2018 Aug 14 [PubMed PMID: 30122874]
Seitz HK, Bataller R, Cortez-Pinto H, Gao B, Gual A, Lackner C, Mathurin P, Mueller S, Szabo G, Tsukamoto H. Alcoholic liver disease. Nature reviews. Disease primers. 2018 Aug 16:4(1):16. doi: 10.1038/s41572-018-0014-7. Epub 2018 Aug 16 [PubMed PMID: 30115921]
Cleveland E, Bandy A, VanWagner LB. Diagnostic challenges of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. Clinical liver disease. 2018 Apr:11(4):98-104. doi: 10.1002/cld.716. Epub 2018 Apr 20 [PubMed PMID: 30147867]
Misra A, Soares MJ, Mohan V, Anoop S, Abhishek V, Vaidya R, Pradeepa R. Body fat, metabolic syndrome and hyperglycemia in South Asians. Journal of diabetes and its complications. 2018 Nov:32(11):1068-1075. doi: 10.1016/j.jdiacomp.2018.08.001. Epub 2018 Aug 4 [PubMed PMID: 30115487]
Angulo P, GI epidemiology: nonalcoholic fatty liver disease. Alimentary pharmacology [PubMed PMID: 17402991]
Level 1 (high-level) evidenceTomic D, Kemp WW, Roberts SK. Nonalcoholic fatty liver disease: current concepts, epidemiology and management strategies. European journal of gastroenterology & hepatology. 2018 Oct:30(10):1103-1115. doi: 10.1097/MEG.0000000000001235. Epub [PubMed PMID: 30113367]
Sanyal AJ. Putting non-alcoholic fatty liver disease on the radar for primary care physicians: how well are we doing? BMC medicine. 2018 Aug 24:16(1):148. doi: 10.1186/s12916-018-1149-9. Epub 2018 Aug 24 [PubMed PMID: 30139362]
Farrell GC. The liver and the waistline: Fifty years of growth. Journal of gastroenterology and hepatology. 2009 Oct:24 Suppl 3():S105-18. doi: 10.1111/j.1440-1746.2009.06080.x. Epub [PubMed PMID: 19799688]
Level 3 (low-level) evidenceYoo JJ,Kim W,Kim MY,Jun DW,Kim SG,Yeon JE,Lee JW,Cho YK,Park SH,Sohn JH, Recent research trends and updates on nonalcoholic fatty liver disease. Clinical and molecular hepatology. 2018 Aug 8 [PubMed PMID: 30086613]
Loria P, Adinolfi LE, Bellentani S, Bugianesi E, Grieco A, Fargion S, Gasbarrini A, Loguercio C, Lonardo A, Marchesini G, Marra F, Persico M, Prati D, Baroni GS, NAFLD Expert Committee of the Associazione Italiana per lo studio del Fegato. Practice guidelines for the diagnosis and management of nonalcoholic fatty liver disease. A decalogue from the Italian Association for the Study of the Liver (AISF) Expert Committee. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2010 Apr:42(4):272-82. doi: 10.1016/j.dld.2010.01.021. Epub 2010 Feb 19 [PubMed PMID: 20171943]
Level 1 (high-level) evidenceMatthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985 Jul:28(7):412-9 [PubMed PMID: 3899825]
Katz A, Nambi SS, Mather K, Baron AD, Follmann DA, Sullivan G, Quon MJ. Quantitative insulin sensitivity check index: a simple, accurate method for assessing insulin sensitivity in humans. The Journal of clinical endocrinology and metabolism. 2000 Jul:85(7):2402-10 [PubMed PMID: 10902785]
Level 1 (high-level) evidenceRatziu V,Bellentani S,Cortez-Pinto H,Day C,Marchesini G, A position statement on NAFLD/NASH based on the EASL 2009 special conference. Journal of hepatology. 2010 Aug; [PubMed PMID: 20494470]
Torruellas C,French SW,Medici V, Diagnosis of alcoholic liver disease. World journal of gastroenterology. 2014 Sep 7 [PubMed PMID: 25206273]
Kosmalski M, Mokros Ł, Kuna P, Witusik A, Pietras T. Changes in the immune system - the key to diagnostics and therapy of patients with non-alcoholic fatty liver disease. Central-European journal of immunology. 2018:43(2):231-239. doi: 10.5114/ceji.2018.77395. Epub 2018 Jun 30 [PubMed PMID: 30135638]
Agganis B, Lee D, Sepe T. Liver enzymes: No trivial elevations, even if asymptomatic. Cleveland Clinic journal of medicine. 2018 Aug:85(8):612-617. doi: 10.3949/ccjm.85a.17103. Epub [PubMed PMID: 30102591]
Ratziu V, Charlotte F, Heurtier A, Gombert S, Giral P, Bruckert E, Grimaldi A, Capron F, Poynard T, LIDO Study Group. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology. 2005 Jun:128(7):1898-906 [PubMed PMID: 15940625]
von Schönfels W,Beckmann JH,Ahrens M,Hendricks A,Röcken C,Szymczak S,Hampe J,Schafmayer C, Histologic improvement of NAFLD in patients with obesity after bariatric surgery based on standardized NAS (NAFLD activity score). Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery. 2018 Jul 24 [PubMed PMID: 30146425]
Loman BR,Hernández-Saavedra D,An R,Rector RS, Prebiotic and probiotic treatment of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Nutrition reviews. 2018 Aug 3 [PubMed PMID: 30113661]
Level 1 (high-level) evidenceAlkhouri N, Poordad F, Lawitz E. Management of nonalcoholic fatty liver disease: Lessons learned from type 2 diabetes. Hepatology communications. 2018 Jul:2(7):778-785. doi: 10.1002/hep4.1195. Epub 2018 Jun 7 [PubMed PMID: 30027137]
Lirussi F, Azzalini L, Orando S, Orlando R, Angelico F. Antioxidant supplements for non-alcoholic fatty liver disease and/or steatohepatitis. The Cochrane database of systematic reviews. 2007 Jan 24:2007(1):CD004996 [PubMed PMID: 17253535]
Level 1 (high-level) evidenceAngelico F, Burattin M, Alessandri C, Del Ben M, Lirussi F. Drugs improving insulin resistance for non-alcoholic fatty liver disease and/or non-alcoholic steatohepatitis. The Cochrane database of systematic reviews. 2007 Jan 24:(1):CD005166 [PubMed PMID: 17253544]
Level 1 (high-level) evidenceSanyal AJ,Chalasani N,Kowdley KV,McCullough A,Diehl AM,Bass NM,Neuschwander-Tetri BA,Lavine JE,Tonascia J,Unalp A,Van Natta M,Clark J,Brunt EM,Kleiner DE,Hoofnagle JH,Robuck PR, Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. The New England journal of medicine. 2010 May 6; [PubMed PMID: 20427778]
Level 1 (high-level) evidenceBaumeister SE, Völzke H, Marschall P, John U, Schmidt CO, Flessa S, Alte D. Impact of fatty liver disease on health care utilization and costs in a general population: a 5-year observation. Gastroenterology. 2008 Jan:134(1):85-94 [PubMed PMID: 18005961]
Level 2 (mid-level) evidenceEsquivel CM, Garcia M, Armando L, Ortiz G, Lascano FM, Foscarini JM. Laparoscopic Sleeve Gastrectomy Resolves NAFLD: Another Formal Indication for Bariatric Surgery? Obesity surgery. 2018 Dec:28(12):4022-4033. doi: 10.1007/s11695-018-3466-7. Epub [PubMed PMID: 30121855]
Coates AM, Hill AM, Tan SY. Nuts and Cardiovascular Disease Prevention. Current atherosclerosis reports. 2018 Aug 9:20(10):48. doi: 10.1007/s11883-018-0749-3. Epub 2018 Aug 9 [PubMed PMID: 30094487]
Sigler MA,Congdon L,Edwards KL, An Evidence-Based Review of Statin Use in Patients With Nonalcoholic Fatty Liver Disease. Clinical medicine insights. Gastroenterology. 2018 [PubMed PMID: 30013416]