Introduction
A fistula-in-ano is an epithelial-lined tract connecting the anal canal to the perianal skin. Anal fistulas can have many causes but are most commonly the result of an anorectal abscess. Classification of the fistula is determined in relation to the anal sphincters. Although benign, the condition can cause significant distress and embarrassment to the patient. Treatment focuses on control of the infection and maintaining fecal continence. Many treatment options are available, and novel treatments are steadily proposed and tested. This article will review the fundamental principles of fistula-in-ano diagnosis and treatment.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Fistula-in-ano often occurs following anorectal abscess. An anorectal abscess occurs when an anal gland becomes obstructed, resulting in infection and abscess formation. The infection is located near the sphincter complex, and therefore the fistula can traverse the sphincters. One-third of patients undergoing incision and drainage of an anorectal abscess will later develop a fistula.[1] Thirty to 70% of patients diagnosed with an anorectal abscess will already have a fistula present on exam.[2]
Epidemiology
Fistula-in-ano is one of the most common anorectal diseases. The prevalence is greater in men than women, with a rate of 12.3 cases per 100,000 and 5.6 cases per 100,000, respectively.[3] The average age at diagnosis is 38 years, with most occurring between 20 to 40 years of age.[4] Risk factors for fistula development include obesity, diabetes, smoking, hyperlipidemia, and a sedentary lifestyle.[5]
Pathophysiology
Simple anal fistulas are thought to be due to glandular obstruction resulting in an anorectal abscess and, ultimately, a fistula. Characteristics of a simple fistula include a single tract, subcutaneous tract, and those that involve less than 30% of the external sphincter. A simple fistula is the easiest to treat and has the lowest recurrence and complication rates.
Complex fistulas include those that involve more than 30% of the external sphincter, fistulas with multiple tracts, recurrent fistulas, and those associated with other predisposing factors, including Crohn disease and radiation treatment.[6] Due to the large involvement of the external sphincter, a simple fistulotomy should not be performed due to the risk of postoperative fecal incontinence. Complex repair or staged repair is preferred to preserve sphincter function.
History and Physical
Patients presenting with an anorectal abscess often experience significant perineal pain and occasionally drainage. Systemic signs, such as fever, are rare in immunocompetent patients. The pain experienced is often exquisite, preventing a patient from sitting or tolerating a physical exam. Deeper abscesses may cause low back pain or pressure.
A thorough history and physical examination are necessary to classify the fistula and create a treatment plan appropriately. Previous diagnoses of inflammatory bowel disease, rectal or anal neoplasm, previous anorectal disease, and prior surgeries are important in diagnosis and treatment planning. Baseline fecal continence should be assessed and documented. In the presence of multiple fistulas or ongoing recurrence, a diagnosis of inflammatory bowel disease should be considered.
Evaluation
A complete rectal exam is essential for the accurate diagnosis of fistula-in-ano. It is important to rule out other anorectal pathology and confirm the diagnosis of a fistula. Due to patient discomfort, this exam is often performed under anesthesia in the operating room. This allows for a complete examination as well as treatment in the same setting. The rectal exam should include inspection of the perianal skin and any external openings. A digital rectal exam should be performed to evaluate for any masses as well as sphincter tone. The internal opening may also be palpable within the anal canal. Anoscopy may be used to locate and evaluate the internal opening. Fistula probes help identify the tract in most cases, but if unsuccessful, injection of hydrogen peroxide may lead to the identification of the internal opening.
Classification of anal fistulas is based on anatomy, specifically in relation to the sphincter complex. In 1976, Dr. Parks published a paper describing a classification system for anal fistulas that is still widely used today. Four types were described: intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric.[7] Appropriate classification is essential for adequate treatment and conservation of the external anal sphincter to preserve fecal continence.
- Intersphincteric (45%) – The fistula penetrates through the internal sphincter but spares the external sphincter.
- Transphincteric (30%) – The fistula passes through both the internal and external sphincters.
- Suprasphincteric (20%) – The fistula penetrates through the internal sphincter and then extends superiorly in the plane between the sphincters to pass above the external sphincter before extending to the perineum. This classification includes horseshoe abscesses.
- Extrasphincteric (5%) – This fistula is very rare. It forms a connection from the rectum to the perineum that extends laterally to the internal and external sphincter. These can be the most difficult to treat due to the need to preserve the sphincter complex.
The classification of the fistula is often diagnosed during an exam under anesthesia in the setting of a simple fistula. Evaluation of complex fistulas, including recurrent disease and fistulas in the setting of perianal Crohn disease, may benefit from pre-operative imaging. MRI, endoanal ultrasound, fistulography, and CT are all proven to contribute to an accurate diagnosis, with MRI being the most sensitive (>90%). A combination of two imaging modalities increases the diagnostic accuracy to 100%.[2]
Treatment / Management
The treatment of an anal fistula depends on the location of the fistula as well as precipitating factors. Most fistulas are treated surgically, through a variety of different procedures depending on external and internal sphincter involvement. Complex fistulas, particularly those caused by Crohn disease, are treated medically. The most common options will be discussed in detail.
- Fistulotomy – Fistulotomy entails opening the fistula tract and possibly dividing sphincter muscle. This surgical treatment is very effective for simple fistulas with minimal sphincter involvement resulting in healing in 90% of properly selected patients.[8] Marsupialization of the fistulotomy edges has proven to decrease bleeding and improve post-operative pain control.[9] (A1)
- Endorectal advancement flap – This procedure is technically more challenging than fistulotomy. The endorectal advancement flap procedure involves closure of the internal opening of the tract, debridement of the tract, and mobilization of anorectal mucosa to cover the defect. The sphincter is not divided during this procedure but can be compromised during the flap with reports of incontinence up to 35%.[10] The results of healing vary significantly between studies but are reported between 66% to 87%.[8][1] Failure is associated with Crohn disease, malignancies, and a history of previous repair attempts.[11][12] (B2)
- Seton placement – Seton drain placement is often reserved for complex fistulas and used in a two-stage technique. Initial placement is used to gain source control, while the second stage often includes fistulotomy. Setons can be classified as ‘draining’ or ‘cutting.’ A draining seton is placed through the fistula tract and tied loosely in place to maintain long term drainage. Many materials can be used, including vessel loops, sutures, or newly available drain devices. A cutting seton is tied tightly around the fistula tract to slowly divide the sphincter complex as it can be tightened over time. This allows for the slow division of the sphincter with decreased risk of incontinence. A completion fistulotomy would then be performed. This two-staged technique will allow for complete healing of the fistula in 94% of patients.[13] The rate of fecal incontinence following seton placement varies but has been documented as high as 12%.[14] (A1)
- LIFT – The ligation of intersphincteric fistula tract (LIFT) procedure can be used for the treatment of simple and complex fistulas with an average success rate of 71%.[15] The procedure involves identification of the internal opening with suture ligation of the intersphincteric portion of the fistula. The tract and infected gland are then excised and the wound debrided with curettage. No portion of the external sphincter is divided, so fecal incontinence is rare. The LIFT procedure can be performed following seton placement as part of a two-stage technique.[2] (A1)
- Fibrin plug and glue – A fibrin plug is a treatment option that involves a collagen matrix used to block or plug the internal opening of the fistula tract. The treatment is appealing as it does not involve dissection or division of the sphincter complex and therefore, should not contribute to incontinence. Unfortunately, the treatment is less than 50% successful in the treatment of fistula-in-ano.[16] Similarly, fibrin glue has also been trialed to promote the healing of fistula tracts. This also preserves sphincter function but has low success rates varying from 14% to 69%.[17][18] Both have been initially discarded as ineffective, but more recent studies have involved a combination of surgical fistula treatment in combination with fibrin plugs and fibrin glue, which may develop into a viable treatment option following more research.[2] (A1)
- Medical management – Antibiotics are often unnecessary in the setting of an uncomplicated and drained rectal abscess. Instead, antibiotics are reserved for immunocompromised patients, those with systemic signs of illness and the presence of cellulitis at the abscess. HIV patients may benefit from wound cultures and antibiotics.[2] Medical management should also be considered in Crohn patients. Infliximab, a TNFa monoclonal antibody, has demonstrated a fistula closure rate of 36% following 54 weeks of treatment.[19] If medical treatment is unsuccessful, a staged fistulotomy may be necessary. (A1)
Differential Diagnosis
- Acute proctitis
- Anal carcinoma
- Anorectal abscess
- Constipation
- Diverticulitis
- Hidradenitis suppurativa
- Inflammatory bowel disease
- Pilonidal cyst
- Pilonidal sinus
Prognosis
Fistula-in-ano is not a life-threatening condition but can have a significant impact on a patient’s quality of life. Treatment is focused on the destruction of the fistula tract with the preservation of the sphincter complex. Complications of treatment can be life-altering for a patient and include fecal incontinence, fistula recurrence, and anal stenosis. The risk of recurrence varies between 3% to 57% depending on the anatomic classification of the fistula and treatment modality.[20]
Complications
The greatest risk of surgical treatment involves disruption of the external sphincter resulting in fecal incontinence. The preoperative evaluation must include the patient’s preoperative continence status and, if possible, documentation of sphincter tone prior to anesthesia and paralysis. The anatomic classification of the fistula, as well as the surgical approach, are the most important factors when determining the risk of post-operative fecal incontinence. For this reason, the surgical approach depends on the anatomic considerations to reduce the risk of incontinence. Complex fistulas, including suprasphincteric and extrasphincteric fistulas, have a higher risk of incontinence due to sphincter involvement.
Recurrence of fistula-in-ano is higher in obese patients, smokers, and those with a history of anal surgery. Anatomical factors including multiple fistula tracts, high transphincteric fistula, inability to determine an internal opening, seton placement, and horseshoe abscesses were also associated with a higher rate of recurrence.[20] Recurrence of the fistula often occurs within the first year of treatment.[21]
Enhancing Healthcare Team Outcomes
A diagnosis of fistula-in-ano should be considered for any patient with purulent or feculent anal drainage, especially with a history of an anorectal abscess, Crohn’s disease, or prior radiation. Diagnosis is often confirmed on physical exam, but more complex fistulas may require imaging for identification. Classification of the fistula is based on anatomy, which is best assessed during the exam. Due to high levels of pain with the exam, an exam under anesthesia may be necessary for an accurate diagnosis.
The treatment options for fistula-in-ano vary widely depending on external sphincter involvement. The development of new and novel treatments aimed at sphincter conservation continues. Although medical treatment is appropriate for some cases, most fistulas require a surgical procedure. Diagnosis or suspicion of an anal fistula should be followed by surgical consult. In the setting of a complex fistula, colorectal surgical consult may be necessary.
Media
(Click Image to Enlarge)
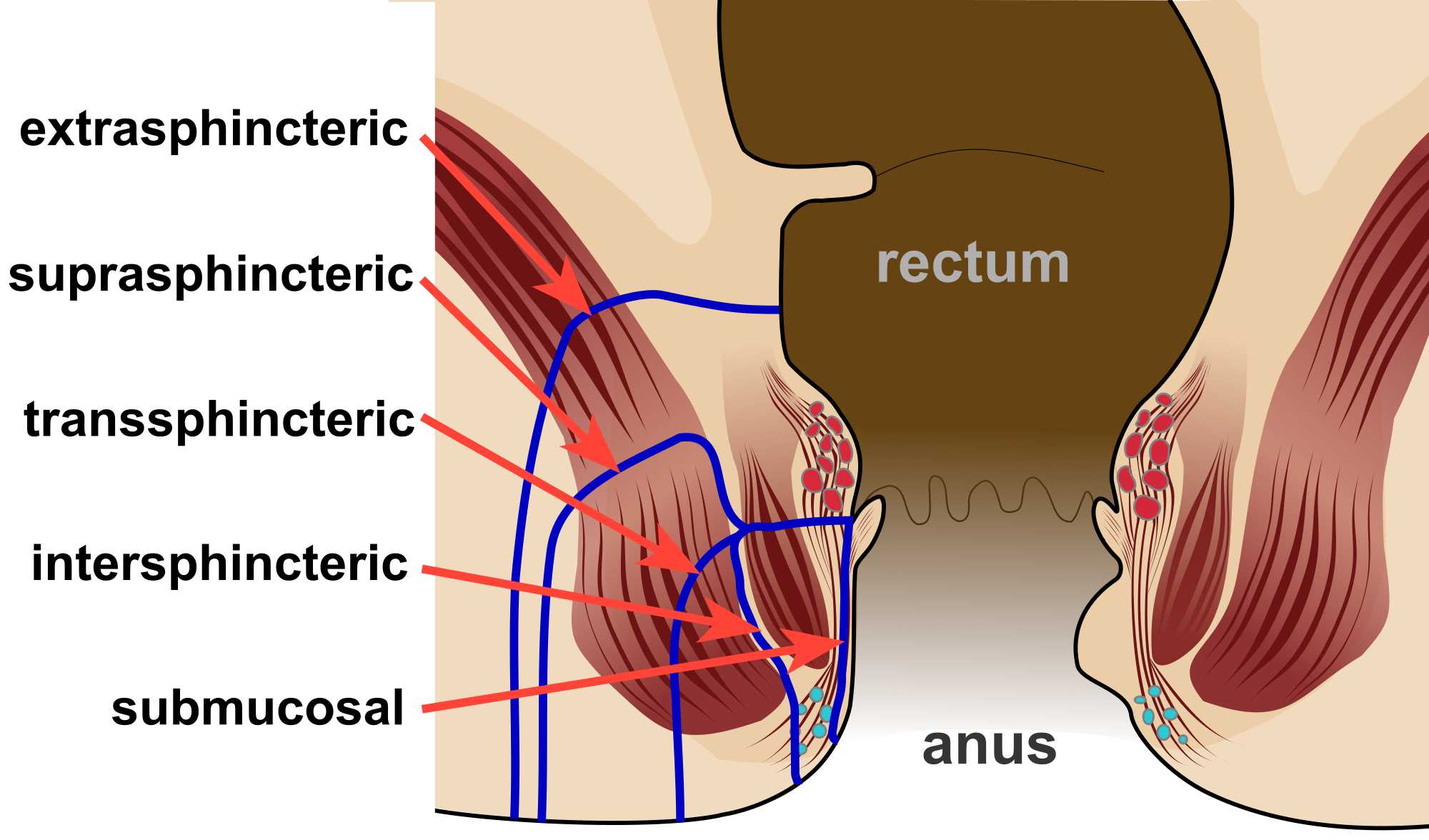
Different types of anal fistula Contributed by Wikimedia Commons, Mcort NGHH (CC by 4.0) https://creativecommons.org/licenses/by/4.0/
References
Abbas MA, Lemus-Rangel R, Hamadani A. Long-term outcome of endorectal advancement flap for complex anorectal fistulae. The American surgeon. 2008 Oct:74(10):921-4 [PubMed PMID: 18942614]
Level 2 (mid-level) evidenceVogel JD, Johnson EK, Morris AM, Paquette IM, Saclarides TJ, Feingold DL, Steele SR. Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula. Diseases of the colon and rectum. 2016 Dec:59(12):1117-1133 [PubMed PMID: 27824697]
Level 1 (high-level) evidenceSainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Annales chirurgiae et gynaecologiae. 1984:73(4):219-24 [PubMed PMID: 6508203]
Level 2 (mid-level) evidenceRead DR, Abcarian H. A prospective survey of 474 patients with anorectal abscess. Diseases of the colon and rectum. 1979 Nov-Dec:22(8):566-8 [PubMed PMID: 527452]
Level 3 (low-level) evidenceWang D, Yang G, Qiu J, Song Y, Wang L, Gao J, Wang C. Risk factors for anal fistula: a case-control study. Techniques in coloproctology. 2014 Jul:18(7):635-9. doi: 10.1007/s10151-013-1111-y. Epub 2014 Jan 23 [PubMed PMID: 24452294]
Level 2 (mid-level) evidenceAkiba RT, Rodrigues FG, da Silva G. Management of Complex Perineal Fistula Disease. Clinics in colon and rectal surgery. 2016 Jun:29(2):92-100. doi: 10.1055/s-0036-1580631. Epub [PubMed PMID: 27247533]
Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. The British journal of surgery. 1976 Jan:63(1):1-12 [PubMed PMID: 1267867]
Hall JF, Bordeianou L, Hyman N, Read T, Bartus C, Schoetz D, Marcello PW. Outcomes after operations for anal fistula: results of a prospective, multicenter, regional study. Diseases of the colon and rectum. 2014 Nov:57(11):1304-8. doi: 10.1097/DCR.0000000000000216. Epub [PubMed PMID: 25285698]
Level 2 (mid-level) evidencePescatori M, Ayabaca SM, Cafaro D, Iannello A, Magrini S. Marsupialization of fistulotomy and fistulectomy wounds improves healing and decreases bleeding: a randomized controlled trial. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2006 Jan:8(1):11-4 [PubMed PMID: 16519632]
Level 1 (high-level) evidenceUribe N, Balciscueta Z, Mínguez M, Martín MC, López M, Mora F, Primo V. "Core out" or "curettage" in rectal advancement flap for cryptoglandular anal fistula. International journal of colorectal disease. 2015 May:30(5):613-9. doi: 10.1007/s00384-015-2133-x. Epub 2015 Jan 24 [PubMed PMID: 25612521]
Level 2 (mid-level) evidenceDavies M, Harris D, Lohana P, Chandra Sekaran TV, Morgan AR, Beynon J, Carr ND. The surgical management of fistula-in-ano in a specialist colorectal unit. International journal of colorectal disease. 2008 Sep:23(9):833-8. doi: 10.1007/s00384-008-0444-x. Epub 2008 Apr 22 [PubMed PMID: 18427814]
Level 2 (mid-level) evidenceGarcia-Aguilar J, Belmonte C, Wong WD, Goldberg SM, Madoff RD. Anal fistula surgery. Factors associated with recurrence and incontinence. Diseases of the colon and rectum. 1996 Jul:39(7):723-9 [PubMed PMID: 8674361]
Level 2 (mid-level) evidenceKelly ME, Heneghan HM, McDermott FD, Nason GJ, Freeman C, Martin ST, Winter DC. The role of loose seton in the management of anal fistula: a multicenter study of 200 patients. Techniques in coloproctology. 2014 Oct:18(10):915-9. doi: 10.1007/s10151-014-1186-0. Epub 2014 Jul 3 [PubMed PMID: 24989839]
Level 2 (mid-level) evidenceRitchie RD, Sackier JM, Hodde JP. Incontinence rates after cutting seton treatment for anal fistula. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2009 Jul:11(6):564-71. doi: 10.1111/j.1463-1318.2008.01713.x. Epub 2008 Oct 17 [PubMed PMID: 19175623]
Level 1 (high-level) evidenceHong KD, Kang S, Kalaskar S, Wexner SD. Ligation of intersphincteric fistula tract (LIFT) to treat anal fistula: systematic review and meta-analysis. Techniques in coloproctology. 2014 Aug:18(8):685-91. doi: 10.1007/s10151-014-1183-3. Epub 2014 Jun 24 [PubMed PMID: 24957361]
Level 1 (high-level) evidenceStamos MJ, Snyder M, Robb BW, Ky A, Singer M, Stewart DB, Sonoda T, Abcarian H. Prospective multicenter study of a synthetic bioabsorbable anal fistula plug to treat cryptoglandular transsphincteric anal fistulas. Diseases of the colon and rectum. 2015 Mar:58(3):344-51. doi: 10.1097/DCR.0000000000000288. Epub [PubMed PMID: 25664714]
Level 2 (mid-level) evidenceBuchanan GN, Bartram CI, Phillips RK, Gould SW, Halligan S, Rockall TA, Sibbons P, Cohen RG. Efficacy of fibrin sealant in the management of complex anal fistula: a prospective trial. Diseases of the colon and rectum. 2003 Sep:46(9):1167-74 [PubMed PMID: 12972959]
Sentovich SM. Fibrin glue for anal fistulas: long-term results. Diseases of the colon and rectum. 2003 Apr:46(4):498-502 [PubMed PMID: 12682544]
Sands BE, Anderson FH, Bernstein CN, Chey WY, Feagan BG, Fedorak RN, Kamm MA, Korzenik JR, Lashner BA, Onken JE, Rachmilewitz D, Rutgeerts P, Wild G, Wolf DC, Marsters PA, Travers SB, Blank MA, van Deventer SJ. Infliximab maintenance therapy for fistulizing Crohn's disease. The New England journal of medicine. 2004 Feb 26:350(9):876-85 [PubMed PMID: 14985485]
Level 1 (high-level) evidenceMei Z, Wang Q, Zhang Y, Liu P, Ge M, Du P, Yang W, He Y. Risk Factors for Recurrence after anal fistula surgery: A meta-analysis. International journal of surgery (London, England). 2019 Sep:69():153-164. doi: 10.1016/j.ijsu.2019.08.003. Epub 2019 Aug 7 [PubMed PMID: 31400504]
Level 1 (high-level) evidenceOrtiz H, Marzo M, de Miguel M, Ciga MA, Oteiza F, Armendariz P. Length of follow-up after fistulotomy and fistulectomy associated with endorectal advancement flap repair for fistula in ano. The British journal of surgery. 2008 Apr:95(4):484-7 [PubMed PMID: 18161890]