Introduction
Globe rupture, globe laceration, globe perforation, or open globe injuries are forms of ocular trauma that require urgent diagnosis and treatment. Globe rupture is the common term used to describe all potential types of open globe injuries. Two primary mechanisms can disrupt the integrity of the globe: penetration, perforation, or laceration and rupture due to blunt force.
A penetrating injury is when an object penetrates the eye, but the object does not go all the way through the eye. In these cases, there can be an intraocular foreign body that remains in the eye. If there is an entrance and an exit wound, then this is considered a perforating injury.
In the United States, there are approximately 3 cases of globe rupture per 100,000 people annually.[1] Diagnosis of globe rupture is based on history and clinical ophthalmologic examination, typically consisting of the slit lamp and fundoscopic evaluation. Imaging may not be reliable to diagnose a globe rupture but should be obtained as a supplement to the workup. When there is a high index of suspicion, an immediate consultation with an ophthalmologist for evaluation is the recommended course of treatment.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
In children, sharp objects like scissors are the most likely cause of ocular globe rupture. The majority of these injuries happen at home.[2] In adults, workplace injuries, assaults, and motor vehicle accidents are common causes. In the elderly, ground-level falls are the most common causes of globe rupture.[3][4] A large study from China found that if the patient has a penetrating or perforating injury with an intraocular foreign body, it is most commonly due to an explosive in patients under 10, and more likely due to a foreign body if over ten years of age.[5] Other potential etiologies of globe rupture include gunshots, sporting injuries, stab wounds, and blast wounds.[6][7][8]
Epidemiology
Globe rupture is more common in males than in females.[9] Among males, globe rupture is nearly twice as common in those under 40 years of age compared with those over the age of 40. In adult males under 40 years of age, assault and workplace injuries are the most common causes of globe rupture. In the population over the age of 75, globe ruptures are most commonly caused by ground-level falls.[3] In indirect trauma, the most common location of rupture is at the superior nasal quadrant, close to the limbus. Globe rupture can happen at any location of penetration and along any of the meridians of the eye.[10] Substance abuse is associated with higher rates of ocular trauma.[11]
Pathophysiology
Globe rupture can either occur due to an object penetrating the ocular tissues or by blunt trauma. Blunt trauma can cause an acute rise in intraocular pressure and cause a rupture in the location where the eye is the weakest. In eyes that have not had surgery, the rupture is most commonly posterior to the extraocular muscles where the sclera is the weakest. In eyes that have had previous intraocular surgery, the rupture is often at the prior incision site. The eye also commonly ruptures at the limbus in blunt trauma. In clinical models, intraocular pressures greater than 7000 mmHg may be needed to rupture the globe.[12]
History and Physical
The history of patients presenting with globe rupture should focus on the etiology of the ocular or periocular trauma. The patient may present with sudden eye pain and vision loss after a potentially penetrating injury. Common penetrating causes of globe rupture may include glass or metal fragments, shotgun or BB pellets, and wood shavings from wood grinding. Globe rupture resulting from blunt trauma may result from mechanical falls, syncope, seizures, motor vehicle accidents with airbag deployment, or assaults with blunt objects.
The physical exam on patients with potential globe rupture requires a detailed ophthalmologic assessment. Careful evaluation of the patient’s baseline visual acuity is critical. A slit lamp examination should be performed to assess the anterior portion of the globe and the anterior chamber. It is essential to carefully assess the conjunctiva, looking for defects, visible foreign bodies, or lacerations. Particular attention should be paid to the equatorial sclera immediately posterior to the insertion of the rectus muscles, as this area is one of the most common locations for globe rupture because the sclera is thinnest at this location.[13] The pupil should be examined for reactivity and shape, taking note of any irregularities in the roundness of the pupil. No pressure should be applied to the globe during evaluation; this means tonometry and eversion of the lids should not be part of the initial assessment.
Evaluation
Evaluation of the eye to assess for a globe injury after trauma is possible once an assessment of the patient's airway, breathing, and circulation has taken place. Patients will often have decreased visual acuity, which can be assessed using a Snellen chart or near card. In patients with severe visual impairment, acuity evaluation is by the patient's ability to count fingers (CF), see a moving hand (HM), or flashes of light (LP). Inspection of the eye using a slit lamp enhances the ability to detect penetrating foreign bodies, scleral or corneal lacerations, uveal prolapse, or iris abnormalities such as peaked or "tear-drop" pupils. A Seidel sign may also be present when performing fluorescein staining of the cornea and sclera as a stream of clear aqueous fluid originating from the globe wound site. However, the globe can be open even if this sign is negative.[14] Seidel testing is contraindicated in cases of obvious globe rupture.
A maxillofacial computed tomography (CT) scan can aid in managing globe rupture, although it should never replace an ophthalmic evaluation.[15][16] A CT scan is the preferred imaging technique to assess the presence of intraocular foreign bodies.[17] Magnetic resonance imaging (MRI) is contraindicated in ocular trauma with suspected ferromagnetic foreign bodies due to concern for the worsening of the injury. If CT is negative for metallic intraocular objects, but the clinician still suspects an intraocular foreign body, magnetic resonance imaging or plain film radiography are options. Ultrasound can also detect intraocular foreign bodies; however, it is relatively contraindicated as direct pressure on the globe can cause extrusion of the intraocular contents and worsen the initial injury.
Treatment / Management
Once globe rupture is suspected, urgent ophthalmologic consultation is required. The patient should first be treated for any other potentially life-threatening injuries, and food and fluids should be withheld. A Fox shield, cup, or another protective device should protect the affected eye.[18] Removal of foreign bodies should not occur until the patient is in surgery. Maneuvers that increase intraocular pressure (IOP) should be avoided (eg, tonometry, lid retraction, or ocular ultrasound).[19] In patients who are awake and alert, it is recommended to reduce stressors that may increase intraocular pressure. Antiemetics, pain control, and bed rest with elevation of the head of the bed to 30 degrees will aid in this process.
Open globe injuries are tetanus-prone wounds, and patients should receive a booster if their immunization history is uncertain or incomplete.[20] Although no specific prophylactic antibiotic regimen exists, preservative-free topical antibiotic drops before surgery can be given prophylactically to theoretically decrease the risk of endophthalmitis.[21] In unstable patients or where intubation is required, it is essential to choose systemic medications that do not raise IOP.[22] Some common anesthetic agents may increase IOP. There is evidence that ketamine raises IOP, but studies are conflicting. Succinylcholine has been found to raise IOP, although this is reducible with subsequent remifentanil administration. Rocuronium has been found not to raise IOP as much as succinylcholine and is suitable as a muscle relaxer in cases of ruptured globe.(B3)
Surgical management by an ophthalmologist should commence as soon as the patient can safely undergo surgery, as a delay in surgical intervention may lead to worse final visual outcomes and increase the risk of postoperative endophthalmitis.[23][24] Initial surgical management of a globe rupture includes microsurgical corneal or scleral wound repair. Corneal lacerations can be closed with 10-0 nylon-interrupted sutures. Corneal suture knots should be buried to prevent postoperative complications. Scleral wounds may be closed with 7-0, 8-0, or 9-0 nonabsorbable sutures, and an attempt should be made to bury or cover these suture knots as well. Before closure, incarcerated uvea must be reposited or excised, and prolapsed vitreous should be excised from the wound. The anterior chamber should also be reformed and repressurized to an appropriate IOP. Following wound repair, intravitreal or intracameral antibiotics are necessary, as they have been shown to decrease the risk of endophthalmitis following a traumatic globe rupture.[25][26](A1)
If a perforating injury affects that eye posteriorly, further surgical intervention may be necessary. Although anterior wounds require suturing, the surgeon may leave the posterior wound unrepaired so that extrusion of vitreous or retinal disruption during attempted closure is avoidable. Fibrous proliferation occurs along the damaged vitreous between the entrance and exit wounds, often closing the wounds within a week following the trauma. This fibroblastic proliferation can lead to retinal detachments, epiretinal membranes, and proliferative vitreoretinopathy, leading to vision loss. Indications for a vitrectomy include signs of developing transvitreal detachment, the presence of moderate to severe vitreous hemorrhage, phacoanaphylactic uveitis, and damage to other tissue requiring repair. If there is an intraocular foreign body, removal with culture is often necessary, especially if the material is toxic to the eye over time.[27][28](B3)
Following surgical repair, patients will start on topical antibiotics covering the most common pathogens for endophthalmitis following globe rupture: Bacillus cereus and Gram-negative organisms.[29] Patients may also be started on systemic antibiotics for additional prevention against endophthalmitis. Oral levofloxacin (500 mg once a day for 7 to 10 days) covers many of the most common causative organisms except pseudomonas and has some intravitreal penetration.[30] Fungal coverage is also an option in patients with an appropriate history. As recommendations for antibiotic selection can differ depending on the mechanism of injury and changes in the microbiological spectrum, consult recent references of an infectious disease specialist.
Differential Diagnosis
Globe rupture should be a consideration whenever a patient presents with blunt or penetrating facial trauma. An open globe should also be suspected whenever a patient presents with pain or vision loss after injury. The differential diagnosis for globe rupture should include:[3]
- Subconjunctival hemorrhage
- Orbital wall or floor fracture
- Corneal abrasion
- Orbital hemorrhage
- Corneal ulceration
- Glaucoma
- Traumatic iritis
Prognosis
The most important factor influencing the patient's final visual acuity following globe rupture is the patient's presenting visual acuity.[27][31] Other factors leading to a worse final visual acuity include posterior globe involvement of the injury, the existence of a relative afferent pupillary defect, vitreous prolapse through the wound, longer wound length, vitreous hemorrhage, hyphema, endophthalmitis, and retinal detachment.[32][33][34][35] For providers wanting to predict the functional outcome following a serious eye injury, the Ocular Trauma Score was created in 2002 for prognostic purposes.[36]
Complications
Globe rupture may result in a variety of complications, including permanent blindness, endophthalmitis, and chronic pain. Delayed complications of a penetrating injury include cyclitic membrane formation, tractional retinal detachment, choroidal rupture, and phthisis bulbi.[37][38] Sympathetic ophthalmia is another devastating complication where there is diffuse bilateral granulomatous panuveitis following immune system sensitization to the intraocular contents of the traumatized eye. To decrease the risk of sympathetic ophthalmia, several sources recommend enucleation or evisceration within 2 weeks of an open globe injury if the visual prognosis is poor.[39]
Retained intraocular foreign bodies can cause chronic disease in the eyes. Copper foreign body toxicity is called chalcosis and causes the complications of a sunflower cataract, chronic uveitis, vitreous opacification, and copper deposition in the macula. Iron toxicity from a retained intraocular foreign body is called siderosis bulbi and causes the complications of retinal degeneration, iris heterochromia, loss of accommodation, nyctalopia, and loss of visual field.[40]
Consultations
An ophthalmology consult is required when there is any suspicion of a globe rupture.[41] If there is involvement of the eye posteriorly, a retinal specialist will need to be involved in patient evaluation and management.[42] A radiologist should evaluate any imaging for the presence of intraocular foreign bodies. Anesthesia will be needed if the patient needs to go to the operating room.
Deterrence and Patient Education
The patient should receive education on proper eye protection and avoidance of potentially harmful lifestyle choices that may increase their chances of ocular injury. Patients should also understand that they have a higher risk of globe rupture following a penetrating keratoplasty and thus should not partake in any strenuous activities if they undergo that procedure.[43][44]
Enhancing Healthcare Team Outcomes
Management of globe rupture is a surgical emergency until proven otherwise. Patients with this condition typically present to the emergency department, and it is important that the triage team recognize the emergent nature of this presentation and immediately activate a trauma assessment. The patient must be placed in a room and promptly evaluated. Prompt history, physical exam, and visual acuity will give the physician some initial guidance and direction before consulting ophthalmology or considering CT imaging. Some evidence suggests that earlier surgical repair reduces the risk of endophthalmitis.[23][24][45] Thus, repair of open globe injuries should be undertaken within 24 hours if at all possible.
Once globe rupture is safely ruled out, other potential causes of acute ocular pain, including corneal abrasions or ulcerations, can be evaluated, and the patient is appropriately treated. Management of acute ocular pain requires a coordinated interprofessional effort between nursing staff, emergency department clinicians, pharmacists, and ophthalmologic specialists to coordinate an accurate and prompt diagnosis that will result in appropriately directed management and treatment.
Nursing will assist during the evaluation period and any operative procedures, providing clinician support, administering medications, and answering patient questions. If antimicrobial therapy is necessary, an infectious disease board-certified pharmacist can be invaluable, assisting with agent selection based on the latest antibiogram data available. This type of interprofessional teamwork is necessary to guide patients to the best possible outcomes for globe rupture injuries.
Media
(Click Image to Enlarge)
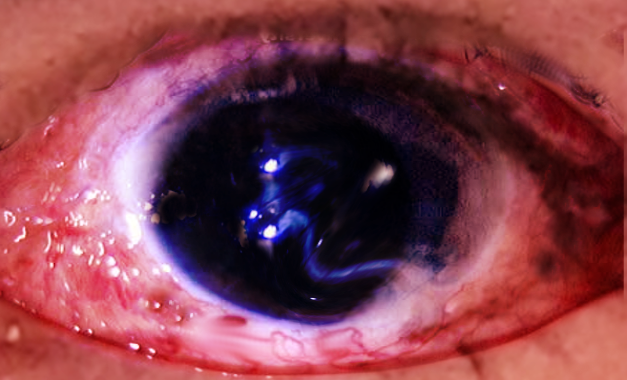
Globe rupture Image courtesy S Bhimji MD
(Click Image to Enlarge)
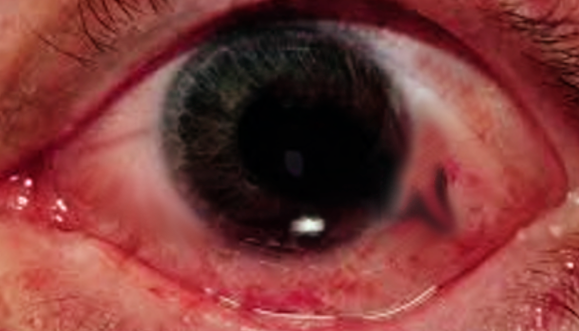
Traumatic globe rupture Image courtesy S Bhimji MD
(Click Image to Enlarge)
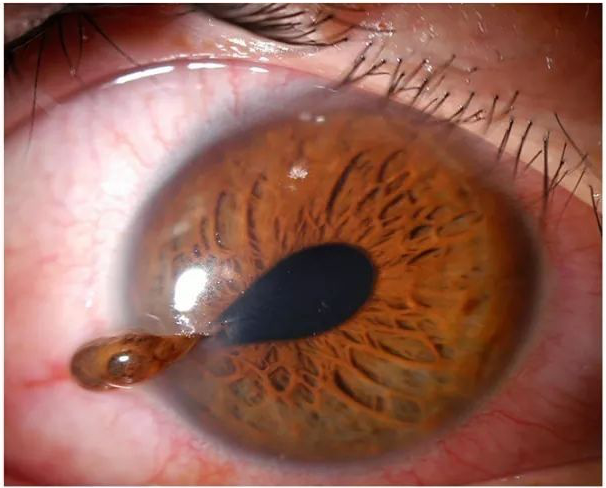
Teardrop pupil with vitreous extrusion in globe rupture. Contributed with Permission by Michael Mohseni, MD
(Click Image to Enlarge)
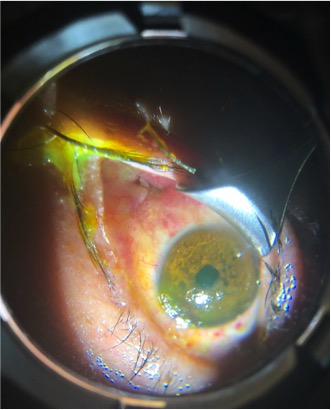
Image of a globe rupture just posterior to the lateral rectus muscle insertion site. The overlying conjunctiva has self-sealed, but remains hyperemic. Contributed by Tatiana S Zanganeh, MD.
(Click Image to Enlarge)

Axial computed tomography of the orbits demonstrating an abnormal posterior globe contour and loss of globe volume, consistent with a posterior globe rupture. Contributed by Diane Wang, MD
References
Li X, Zarbin MA, Bhagat N. Pediatric open globe injury: A review of the literature. Journal of emergencies, trauma, and shock. 2015 Oct-Dec:8(4):216-23. doi: 10.4103/0974-2700.166663. Epub [PubMed PMID: 26604528]
Thompson CG, Kumar N, Billson FA, Martin F. The aetiology of perforating ocular injuries in children. The British journal of ophthalmology. 2002 Aug:86(8):920-2 [PubMed PMID: 12140216]
Hughes E, Fahy G. A 24-month review of globe rupture in a tertiary referral hospital. Irish journal of medical science. 2020 May:189(2):723-726. doi: 10.1007/s11845-019-02097-2. Epub 2019 Sep 13 [PubMed PMID: 31520281]
Andreoli MT, Andreoli CM. Geriatric traumatic open globe injuries. Ophthalmology. 2011 Jan:118(1):156-9. doi: 10.1016/j.ophtha.2010.04.034. Epub 2010 Aug 14 [PubMed PMID: 20709403]
Level 2 (mid-level) evidenceLi L, Lu H, Ma K, Li YY, Wang HY, Liu NP. Etiologic Causes and Epidemiological Characteristics of Patients with Intraocular Foreign Bodies: Retrospective Analysis of 1340 Cases over Ten Years. Journal of ophthalmology. 2018:2018():6309638. doi: 10.1155/2018/6309638. Epub 2018 Jan 31 [PubMed PMID: 29651344]
Level 2 (mid-level) evidenceBen Simon GJ, Moisseiev J, Rosen N, Alhalel A. Gunshot wound to the eye and orbit: a descriptive case series and literature review. The Journal of trauma. 2011 Sep:71(3):771-8; discussion 778. doi: 10.1097/TA.0b013e3182255315. Epub [PubMed PMID: 21909007]
Level 3 (low-level) evidenceCass SP. Ocular injuries in sports. Current sports medicine reports. 2012 Jan-Feb:11(1):11-5. doi: 10.1249/JSR.0b013e318240dc06. Epub [PubMed PMID: 22236819]
Born CT. Blast trauma: the fourth weapon of mass destruction. Scandinavian journal of surgery : SJS : official organ for the Finnish Surgical Society and the Scandinavian Surgical Society. 2005:94(4):279-85 [PubMed PMID: 16425623]
Koo L, Kapadia MK, Singh RP, Sheridan R, Hatton MP. Gender differences in etiology and outcome of open globe injuries. The Journal of trauma. 2005 Jul:59(1):175-8 [PubMed PMID: 16096559]
Level 2 (mid-level) evidenceKumar K, Figurasin R, Kumar S, Waseem M. An Uncommon Meridional Globe Rupture due to Blunt Eye Trauma. Case reports in emergency medicine. 2018:2018():1808509. doi: 10.1155/2018/1808509. Epub 2018 Sep 18 [PubMed PMID: 30319823]
Level 3 (low-level) evidenceWong TY, Klein BE, Klein R. The prevalence and 5-year incidence of ocular trauma. The Beaver Dam Eye Study. Ophthalmology. 2000 Dec:107(12):2196-202 [PubMed PMID: 11097595]
Bisplinghoff JA, McNally C, Duma SM. High-rate internal pressurization of human eyes to predict globe rupture. Archives of ophthalmology (Chicago, Ill. : 1960). 2009 Apr:127(4):520-3. doi: 10.1001/archophthalmol.2008.614. Epub [PubMed PMID: 19365034]
Mohseni M, Blair K, Gurnani B, Bragg BN. Blunt Eye Trauma. StatPearls. 2024 Jan:(): [PubMed PMID: 29261988]
Couperus K, Zabel A, Oguntoye MO. Open Globe: Corneal Laceration Injury with Negative Seidel Sign. Clinical practice and cases in emergency medicine. 2018 Aug:2(3):266-267. doi: 10.5811/cpcem.2018.4.38086. Epub 2018 Jun 12 [PubMed PMID: 30083651]
Level 3 (low-level) evidenceYuan WH, Hsu HC, Cheng HC, Guo WY, Teng MM, Chen SJ, Lin TC. CT of globe rupture: analysis and frequency of findings. AJR. American journal of roentgenology. 2014 May:202(5):1100-7. doi: 10.2214/AJR.13.11010. Epub [PubMed PMID: 24758666]
Level 2 (mid-level) evidenceChou C, Lou YT, Hanna E, Huang SH, Lee SS, Lai HT, Chang KP, Wang HM, Chen CW. Diagnostic performance of isolated orbital CT scan for assessment of globe rupture in acute blunt facial trauma. Injury. 2016 May:47(5):1035-41. doi: 10.1016/j.injury.2016.01.014. Epub 2016 Jan 25 [PubMed PMID: 26944178]
Modjtahedi BS, Rong A, Bobinski M, McGahan J, Morse LS. Imaging characteristics of intraocular foreign bodies: a comparative study of plain film X-ray, computed tomography, ultrasound, and magnetic resonance imaging. Retina (Philadelphia, Pa.). 2015 Jan:35(1):95-104. doi: 10.1097/IAE.0000000000000271. Epub [PubMed PMID: 25090044]
Level 3 (low-level) evidenceRitson JE, Welch J. The management of open globe eye injuries: a discussion of the classification, diagnosis and management of open globe eye injuries. Journal of the Royal Naval Medical Service. 2013:99(3):127-30 [PubMed PMID: 24511795]
Bord SP, Linden J. Trauma to the globe and orbit. Emergency medicine clinics of North America. 2008 Feb:26(1):97-123, vi-vii. doi: 10.1016/j.emc.2007.11.006. Epub [PubMed PMID: 18249259]
Iyer MN, Kranias G, Daun ME. Post-traumatic endophthalmitis involving Clostridium tetani and Bacillus spp. American journal of ophthalmology. 2001 Jul:132(1):116-7 [PubMed PMID: 11438069]
Level 3 (low-level) evidenceLorch A, Sobrin L. Prophylactic antibiotics in posttraumatic infectious endophthalmitis. International ophthalmology clinics. 2013 Fall:53(4):167-76. doi: 10.1097/IIO.0b013e3182a12a1b. Epub [PubMed PMID: 24088943]
Bower T, Samek DA, Mohammed A, Mohammed A, Kasner P, Camoriano D, Kasner O. Systemic medication usage in glaucoma patients. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2018 Jun:53(3):242-245. doi: 10.1016/j.jcjo.2017.10.029. Epub 2018 Feb 1 [PubMed PMID: 29784160]
Agrawal R, Rao G, Naigaonkar R, Ou X, Desai S. Prognostic factors for vision outcome after surgical repair of open globe injuries. Indian journal of ophthalmology. 2011 Nov-Dec:59(6):465-70. doi: 10.4103/0301-4738.86314. Epub [PubMed PMID: 22011491]
Level 2 (mid-level) evidenceZhang Y, Zhang MN, Jiang CH, Yao Y, Zhang K. Endophthalmitis following open globe injury. The British journal of ophthalmology. 2010 Jan:94(1):111-4. doi: 10.1136/bjo.2009.164913. Epub 2009 Aug 18 [PubMed PMID: 19692359]
Level 2 (mid-level) evidenceThevi T, Abas AL. Role of intravitreal/intracameral antibiotics to prevent traumatic endophthalmitis - Meta-analysis. Indian journal of ophthalmology. 2017 Oct:65(10):920-925. doi: 10.4103/ijo.IJO_512_17. Epub [PubMed PMID: 29044054]
Level 1 (high-level) evidenceNarang S, Gupta V, Gupta A, Dogra MR, Pandav SS, Das S. Role of prophylactic intravitreal antibiotics in open globe injuries. Indian journal of ophthalmology. 2003 Mar:51(1):39-44 [PubMed PMID: 12701861]
Level 1 (high-level) evidenceYeh S, Colyer MH, Weichel ED. Current trends in the management of intraocular foreign bodies. Current opinion in ophthalmology. 2008 May:19(3):225-33. doi: 10.1097/ICU.0b013e3282fa75f1. Epub [PubMed PMID: 18408498]
Level 3 (low-level) evidenceLoporchio D, Mukkamala L, Gorukanti K, Zarbin M, Langer P, Bhagat N. Intraocular foreign bodies: A review. Survey of ophthalmology. 2016 Sep-Oct:61(5):582-96. doi: 10.1016/j.survophthal.2016.03.005. Epub 2016 Mar 17 [PubMed PMID: 26994871]
Level 3 (low-level) evidenceJindal A, Pathengay A, Mithal K, Jalali S, Mathai A, Pappuru RR, Narayanan R, Chhablani J, Motukupally SR, Sharma S, Das T, Flynn HW Jr. Endophthalmitis after open globe injuries: changes in microbiological spectrum and isolate susceptibility patterns over 14 years. Journal of ophthalmic inflammation and infection. 2014 Feb 18:4(1):5. doi: 10.1186/1869-5760-4-5. Epub 2014 Feb 18 [PubMed PMID: 24548669]
Ahmed Y, Schimel AM, Pathengay A, Colyer MH, Flynn HW Jr. Endophthalmitis following open-globe injuries. Eye (London, England). 2012 Feb:26(2):212-7. doi: 10.1038/eye.2011.313. Epub 2011 Dec 2 [PubMed PMID: 22134598]
Singh S, Sharma B, Kumar K, Dubey A, Ahirwar K. Epidemiology, clinical profile and factors, predicting final visual outcome of pediatric ocular trauma in a tertiary eye care center of Central India. Indian journal of ophthalmology. 2017 Nov:65(11):1192-1197. doi: 10.4103/ijo.IJO_375_17. Epub [PubMed PMID: 29133650]
Yalcin Tök O, Tok L, Eraslan E, Ozkaya D, Ornek F, Bardak Y. Prognostic factors influencing final visual acuity in open globe injuries. The Journal of trauma. 2011 Dec:71(6):1794-800. doi: 10.1097/TA.0b013e31822b46af. Epub [PubMed PMID: 22182891]
Level 2 (mid-level) evidenceMeng Y, Yan H. Prognostic Factors for Open Globe Injuries and Correlation of Ocular Trauma Score in Tianjin, China. Journal of ophthalmology. 2015:2015():345764. doi: 10.1155/2015/345764. Epub 2015 Sep 29 [PubMed PMID: 26491549]
Agrawal R, Wei HS, Teoh S. Prognostic factors for open globe injuries and correlation of ocular trauma score at a tertiary referral eye care centre in Singapore. Indian journal of ophthalmology. 2013 Sep:61(9):502-6. doi: 10.4103/0301-4738.119436. Epub [PubMed PMID: 24104709]
Level 2 (mid-level) evidenceLieb DF, Scott IU, Flynn HW Jr, Miller D, Feuer WJ. Open globe injuries with positive intraocular cultures: factors influencing final visual acuity outcomes. Ophthalmology. 2003 Aug:110(8):1560-6 [PubMed PMID: 12917173]
Level 2 (mid-level) evidenceKuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The Ocular Trauma Score (OTS). Ophthalmology clinics of North America. 2002 Jun:15(2):163-5, vi [PubMed PMID: 12229231]
Venkatesh R, Bavaharan B, Yadav NK. Predictors for choroidal neovascular membrane formation and visual outcome following blunt ocular trauma. Therapeutic advances in ophthalmology. 2019 Jan-Dec:11():2515841419852011. doi: 10.1177/2515841419852011. Epub 2019 May 23 [PubMed PMID: 31206099]
Level 3 (low-level) evidenceSoylu M, Sizmaz S, Cayli S. Eye injury (ocular trauma) in southern Turkey: epidemiology, ocular survival, and visual outcome. International ophthalmology. 2010 Apr:30(2):143-8. doi: 10.1007/s10792-009-9300-4. Epub 2009 Feb 4 [PubMed PMID: 19190858]
Level 2 (mid-level) evidenceGürdal C, Erdener U, Irkeç M, Orhan M. Incidence of sympathetic ophthalmia after penetrating eye injury and choice of treatment. Ocular immunology and inflammation. 2002 Sep:10(3):223-7 [PubMed PMID: 12789598]
Level 2 (mid-level) evidenceHe X, Hahn P, Iacovelli J, Wong R, King C, Bhisitkul R, Massaro-Giordano M, Dunaief JL. Iron homeostasis and toxicity in retinal degeneration. Progress in retinal and eye research. 2007 Nov:26(6):649-73 [PubMed PMID: 17921041]
Level 3 (low-level) evidenceMagauran B. Conditions requiring emergency ophthalmologic consultation. Emergency medicine clinics of North America. 2008 Feb:26(1):233-8, viii. doi: 10.1016/j.emc.2007.11.008. Epub [PubMed PMID: 18249265]
Coles WH, Haik GM. Vitrectomy in intraocular trauma. Its rationale and its indications and limitations. Archives of ophthalmology (Chicago, Ill. : 1960). 1972 Jun:87(6):621-8 [PubMed PMID: 5032732]
Elder MJ, Stack RR. Globe rupture following penetrating keratoplasty: how often, why, and what can we do to prevent it? Cornea. 2004 Nov:23(8):776-80 [PubMed PMID: 15502477]
Level 2 (mid-level) evidenceKawashima M, Kawakita T, Shimmura S, Tsubota K, Shimazaki J. Characteristics of traumatic globe rupture after keratoplasty. Ophthalmology. 2009 Nov:116(11):2072-6. doi: 10.1016/j.ophtha.2009.04.047. Epub 2009 Sep 19 [PubMed PMID: 19766315]
Level 2 (mid-level) evidenceLi X, Zarbin MA, Langer PD, Bhagat N. POSTTRAUMATIC ENDOPHTHALMITIS: An 18-Year Case Series. Retina (Philadelphia, Pa.). 2018 Jan:38(1):60-71. doi: 10.1097/IAE.0000000000001511. Epub [PubMed PMID: 28590965]
Level 2 (mid-level) evidence