 Anatomy, Bony Pelvis and Lower Limb, Gluteus Minimus Muscle
Anatomy, Bony Pelvis and Lower Limb, Gluteus Minimus Muscle
Introduction
Gluteus minimus is the smallest muscle of the glutei. It shares many similar characteristics with the gluteus medius, including structure and function, blood supply, and innervation. It is located just beneath the gluteus medius muscle. The gluteus minimus predominantly acts as a hip stabilizer and abductor of the hip. The muscle’s blood supply and innervation are from the superior gluteal artery and superior gluteal nerve, respectively. Damage to the nerve or muscle may result in sagging of the pelvis, also known as the Trendelenburg sign. A total hip arthroplasty (THA) may indirectly or directly affect the gluteus minimus by damage to the superior gluteal nerve or by heterotopic ossification (HO). Other clinically significant conditions include greater trochanteric pain syndrome (GTPS), characterized by tendinopathy of the gluteus minimus. Patients will usually present with tenderness along the greater trochanter on the affected side.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The proximal attachment of the gluteus minimus is on the external surface of the ilium. This attachment lies between the anterior and inferior gluteal lines. The anterior gluteal line begins near the iliac crest taking a curved path posteriorly and inferiorly towards the greater sciatic notch. The inferior gluteal line follows a similar path but is shorter and less curved. The gluteus minimus is fan-shaped and is attached distally to the femur at the anterior border of the greater trochanter.[1]
The gluteus minimus is predominantly a hip stabilizer. Its main action is to abduct the hip. It starts to work when the individual is standing on one limb and works in conjunction with the gluteus medius and tensor fascia lata.[2] The gluteus minimus is engaged on the supported side, which allows the pelvis to remain level during the swing phase of gait. The anterior portion of the gluteus minimus also acts as a medial rotator of the thigh.[3][4]
Embryology
Like other limb muscles, the gluteus minimus arises from myoblasts that surround the developing bone. The myoblasts are formed due to tissues nearby that release molecular signals that allow somites to differentiate into myoblasts.[5] Myoblasts then coalesce together to form myotubes characterized by their long, tubular, and multinucleated structure. As the myotubes develop, they begin to form layers that will separate the muscle from neighboring connective tissue.[6]
The lower limb buds start to form around the end of the fourth week, slightly delayed when compared to the upper limb buds. Additionally, the lower limb will rotate medially as the upper limb rotates laterally.
Blood Supply and Lymphatics
The blood supply to the gluteus minimus is supplied by the superior gluteal artery, which arises from the posterior division of the internal iliac artery. As the superior gluteal artery leaves the pelvis through the greater sciatic foramen above the piriformis, it passes posteriorly between the S1 nerve and lumbosacral trunk, dividing into the superficial and deep branches. The deep branch of the superior gluteal artery supplies the gluteus minimus. Following the superior gluteal artery to its most distal point, it then anastomoses with the medial circumflex femoral arteries.[7]
Nerves
The superior gluteal nerve innervates the gluteus minimus. It is a branch of the lumbosacral plexus with nerve root origins of L4, L5, and S1. The nerve runs between the gluteus minimus and medius alongside the superior gluteal artery’s deep branch. It then splits off into a superior branch and an inferior branch. It is the inferior branch that supplies the gluteus minimus.[8][9] Injury to this nerve results in weakness with hip abduction and may result in a Trendelenburg gait.[10]
Muscles
The gluteus minimus is a medial rotator and abductor of the hip. The gluteus minimus also works in conjunction with the gluteus medius and tensor fasciae latae to stabilize the hip by engaging in the abduction of the weight-bearing leg during the swing phase of gait.[2][3][4]
Physiologic Variants
In some people, the gluteus minimus may have two divisions, the anterior and posterior segments. It may also send muscle fibers to the superior gemellus and/or the piriformis.[2]
Surgical Considerations
Nerve injury may occur in one to two percent of cases of a total hip arthroplasty (THA). Injury to the superior gluteal nerve may result in weakness with hip abduction and a Trendelenburg gait. Surgical exploration is indicated if the damage is due to compression of a large hematoma or direct laceration of the nerve.[11]
Another potential complication clinicians must consider following a THA is heterotopic ossification (HO) of the gluteus minimus. Heterotopic ossification characteristically demonstrates ectopic bone forming in extraskeletal tissues. Patients typically present with stiffness and pain of the hip approximately a few months following the surgery. Surgical resection is the recommended treatment if there is a severe loss of range of motion.[12]
Clinical Significance
Damage to the gluteus minimus or the superior gluteal nerve may result in a Trendelenburg gait (gluteal gait). A positive Trendelenburg sign demonstrates pelvic sagging on an unsupported side when asked to stand on one leg; this indicates that the abductor muscles on the ipsilateral (supported) side are weak or non-functional. The gait presents as an individual leaning towards the supported side during the swing phase of the gait to compensate for an appeared longer lower extremity due to the pelvis sagging on the unsupported side. Fractures to the greater trochanter may result in a Trendelenburg gait due to the location of the distal attachments of gluteus minimus.[10]
Tendinopathy of the gluteus minimus results in a condition known as greater trochanteric pain syndrome (GTPS). GTPS is characterized by lateral hip pain. It is often confused with trochanteric bursitis, which is a misleading term due to the direct involvement of the bursae and its very rare occurrence. Greater trochanteric pain syndrome presents similarly to tendinopathy of the rotator cuff muscles in which the disorder occurs at the trochanteric enthesis. A physical examination will reveal tenderness to palpation of the greater trochanter and observation of a Trendelenburg gait.[13] Patients with suspected GTPS should have a standing anteroposterior radiograph of the pelvis to differentiate between hip osteoarthritis. Additionally, an ultrasound of the hip can help identify the offending lesion of the muscle.[14] The treatment for GTPS is supportive (nonsteroidal anti-inflammatory drugs and/or glucocorticoid injection) and activity modification targeted at relieving the stress of the gluteus minimus tendon.[15] Patients with persistent pain for two to three months should have a magnetic resonance imaging of the hip to rule out a partial or complete tear and receive a referral to an orthopedist for a surgical evaluation.[14]
Other Issues
The gluteus minimus muscle can be affected by trigger points. The most common characteristic of the gluteus minimus trigger point is a referred pain starting at the end of the lumbar spine and ending at the ankle (it is similar to the sciatic pain but without the symptoms of weakness, numbness).
Media
(Click Image to Enlarge)
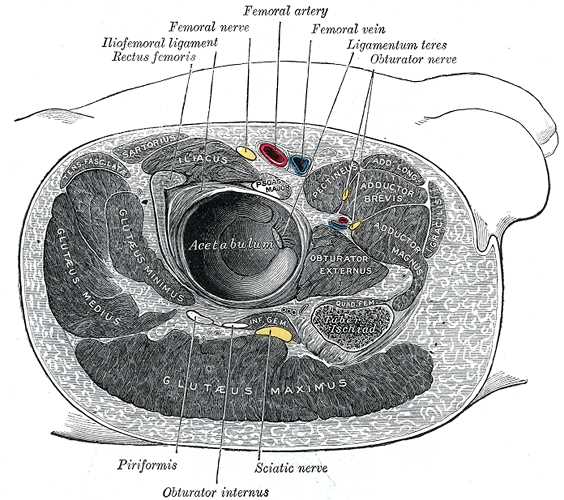
Structures Surrounding the Right Hip Joint. Structures around the right hip joint include the iliofemoral ligament, rectus femoris, femoral nerve, femoral artery, femoral vein, ligamentum teres, obturator nerve, piriformis, obturator internus, sciatic nerve, gluteus maximus, gluteus medius, gluteus minimus, acetabulum, obturator externus, iliacus, pectineus, adductor brevis, and adductor magnus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
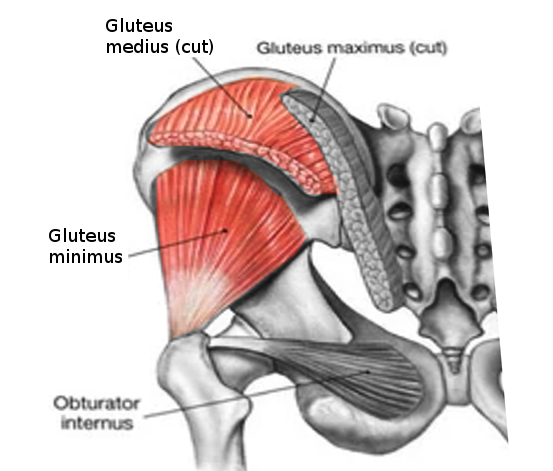
Gluteus Muscles. The Gluteus medius, minimus, maximus, and the obturator internus muscle anatomy are shown.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
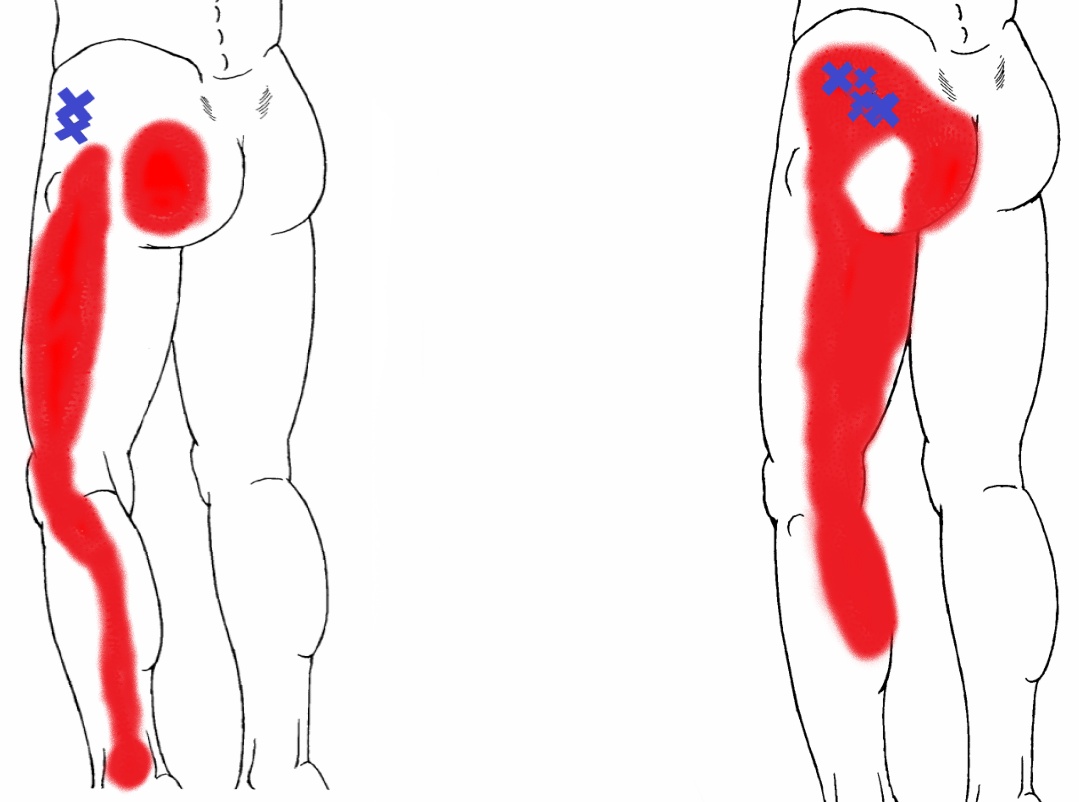
Most common Trigger Points at the Gluteus Minimus muscle. Contributed by Renato Vilella, PT.
References
Walters J, Solomons M, Davies J. Gluteus minimus: observations on its insertion. Journal of anatomy. 2001 Feb:198(Pt 2):239-42 [PubMed PMID: 11273048]
Flack NA, Nicholson HD, Woodley SJ. A review of the anatomy of the hip abductor muscles, gluteus medius, gluteus minimus, and tensor fascia lata. Clinical anatomy (New York, N.Y.). 2012 Sep:25(6):697-708. doi: 10.1002/ca.22004. Epub 2011 Nov 22 [PubMed PMID: 22109658]
Level 1 (high-level) evidenceGottschalk F, Kourosh S, Leveau B. The functional anatomy of tensor fasciae latae and gluteus medius and minimus. Journal of anatomy. 1989 Oct:166():179-89 [PubMed PMID: 2621137]
Whiler L, Fong M, Kim S, Ly A, Qin Y, Yeung E, Mathur S. Gluteus Medius and Minimus Muscle Structure, Strength, and Function in Healthy Adults: Brief Report. Physiotherapy Canada. Physiotherapie Canada. 2017:69(3):212-216. doi: 10.3138/ptc.2016-16. Epub [PubMed PMID: 30275637]
Level 2 (mid-level) evidenceBuckingham M. Muscle differentiation. Which myogenic factors make muscle? Current biology : CB. 1994 Jan 1:4(1):61-3 [PubMed PMID: 7922315]
Level 3 (low-level) evidenceTaylor MV. Muscle development: molecules of myoblast fusion. Current biology : CB. 2000 Sep 7:10(17):R646-8 [PubMed PMID: 10996092]
Level 3 (low-level) evidenceCollinge CA, Ziran NM, Coons DA. Relationship Between the Superior Gluteal Vessels and Nerve at the Greater Sciatic Notch. Orthopedics. 2015 Oct:38(10):e929-33. doi: 10.3928/01477447-20151002-62. Epub [PubMed PMID: 26488790]
Jacobs LG, Buxton RA. The course of the superior gluteal nerve in the lateral approach to the hip. The Journal of bone and joint surgery. American volume. 1989 Sep:71(8):1239-43 [PubMed PMID: 2777853]
Akita K, Sakamoto H, Sato T. Origin, course and distribution of the superior gluteal nerve. Acta anatomica. 1994:149(3):225-30 [PubMed PMID: 7976174]
Caviglia H, Cambiaggi G, Vattani N, Landro ME, Galatro G. Lesion of the hip abductor mechanism. SICOT-J. 2016:2():29. doi: 10.1051/sicotj/2016020. Epub 2016 Jul 6 [PubMed PMID: 27382925]
Eksioglu F, Uslu M, Gudemez E, Atik OS, Tekdemir I. Reliability of the safe area for the superior gluteal nerve. Clinical orthopaedics and related research. 2003 Jul:(412):111-6 [PubMed PMID: 12838060]
Rath EM, Russell GV Jr, Washington WJ, Routt ML Jr. Gluteus minimus necrotic muscle debridement diminishes heterotopic ossification after acetabular fracture fixation. Injury. 2002 Nov:33(9):751-6 [PubMed PMID: 12379382]
Chang KV, Wu WT. An Underdiagnosed Etiology of Lateral Hip Pain-Gluteus Minimus Tendinopathy. Journal of medical ultrasound. 2019 Apr-Jun:27(2):113-114. doi: 10.4103/JMU.JMU_79_18. Epub 2018 Oct 30 [PubMed PMID: 31316226]
Grimaldi A, Mellor R, Hodges P, Bennell K, Wajswelner H, Vicenzino B. Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management. Sports medicine (Auckland, N.Z.). 2015 Aug:45(8):1107-19. doi: 10.1007/s40279-015-0336-5. Epub [PubMed PMID: 25969366]
Torres A, Fernández-Fairen M, Sueiro-Fernández J. Greater trochanteric pain syndrome and gluteus medius and minimus tendinosis: nonsurgical treatment. Pain management. 2018 Jan:8(1):45-55. doi: 10.2217/pmt-2017-0033. Epub 2017 Nov 28 [PubMed PMID: 29182042]