Introduction
Several ascending and descending tracts are present in the spinal cord. The three most important tracts in the spinal cord are:
- Dorsal Column Medial Lemniscus Pathway - This is an ascending sensory tract.
- Spinothalamic Tract - This is an ascending sensory tract.
- Corticospinal Tract - This is a descending motor pathway which has upper motor neurons (UMN) and lower motor neurons (LMN).
The gracile nucleus, along with the cuneate nucleus, is a part of the dorsal column medial lemniscus pathway (DCML). The gracile nucleus situates in the midline dorsal medulla at the junction of the brainstem and the spinal cord. The gracile fasciculus carries sensory input from vertebral level T6 and below and ascends into the gracile nucleus to form the gracile tubercle. The cuneate fasciculus carries information from T6 and above and ascends into the cuneate nucleus to form the cuneate tubercle. These tubercles appear as bumps on the dorsal part of the medulla.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The anatomic location of the gracile nucleus is on the floor of the fourth ventricle. The gracile nucleus gives rise to second-order neurons, which contain six different types of neurons. It is situated medially to the cuneate nucleus. Together they form the medial lemniscus. The gracile nucleus, which forms part of the dorsal column medial lemniscus pathway, is a three-order neuron system:
- First-order neurons- These are the neurons fibers that start from the ipsilateral side of the body and go through the gracile fasciculus and cuneate fasciculus, into the gracile nucleus, and into the cuneate nucleus respectively.
- Second-order neurons- These neurons are in the gracile and the cuneate nucleus. After receiving input from the fasciculi, these nuclei give rise to the internal arcuate fibers. The fibers of both the nuclei decussate and then combine to form the medial lemniscus. The medial lemniscus then travels from the nuclei into the Ventral Posterolateral nucleus of the thalamus.
- Third-order neurons- The third-order neuron fibers relay the information from the thalamus to the primary somatosensory cortex of the cerebrum.[1]
The medial lemniscus and the dorsal column pathway function to carry sensations from the body, first to the thalamus and subsequently to the brain. The sensory signals transmitted are:
- Fine touch
- Vibration
- Visceral pain
- Conscious proprioception
- 2-point discrimination
Embryology
Neuroectoderm gives rise to the neural tube. The dorsal horn of the spinal cord forms from the alar plate of the neural tube, which gives rise to the dorsal column medial lemniscus pathway and is responsible for the sensory input from the body. The ventral horn of the spinal cord forms from the basal plate of the neural tube, which is responsible for the motor control of the body.[2]
Blood Supply and Lymphatics
The blood supply of every structure in the brainstem depends on the specific location of that particular structure. The gracile nucleus is at the level of medulla, which is supplied by the posterior spinal artery dorsally.
Surgical Considerations
There are limited surgical options in the dorsal column medial lemniscus pathway. Due to the abundance of nerve fibers and tracts contained in a minimal space, surgeons must focus the surgery on the particular area without disturbing the tracts around it. Even a minute error can affect the surrounding tracts and lead to severe conditions.
The advances in modern technology have led to the development of[3]:
- DTI - Diffuse tensor imaging
- DTT - Diffusion tensor tractography
These modalities better visualize the specific tracts and pathologies. The nucleus gracilis is thought to be the center where the visceral and cutaneous information integrates.
Hong et al. suggested the use of punctate midline myelotomy for the treatment of visceral pain when compared to analgesics in the treatment of cancer-related pain.[4] Surgical candidates must be able to maintain a clinically stable medical condition apart from the visceral pain, have an expected life span of more than three months, and have pain that is refractory to oral analgesics.[5][6][7]
Clinical Significance
The disease affecting the dorsal column is typically degenerative in nature.
Bedside examination test – This test, called the Romberg test, can help to identify the location of the lesion. The patient is made to stand barefoot, with their feet together and eyes open. Then the patient is asked to close his/her eyes. If the patient sways to one side, it suggests a lesion in the dorsal column medial lemniscus. Care is necessary as the test can cause the patient potentially to fall.
Localization - Research has established that the dorsal column medial lemniscus pathway decussates in the closed dorsal medulla and starts as the medial lemniscus from that side. If the patient presents with sensation loss contralaterally, that is, on one side of the face and the other side of the body, we can localize the lesion to the brainstem. Further, if the patient presents with just the sensation loss in the legs and the trunk, this suggests that the lesion is either below the T6 vertebra or is specifically targeting the gracile nucleus medially.
Certain diseases and conditions disrupt the dorsal column medial lemniscus pathway, all-cause loss of vibration, conscious proprioception, 2- point discrimination, and fine touch. It is difficult to have an isolated lesion of the gracile nucleus and the fasciculus. Any condition that involves the gracile nucleus usually involves the other tracts of the dorsal column medial lemniscus pathway as well.[8] These conditions are:
- Medial Medullary Syndrome - The result of occlusion of the paramedian branches of the anterior spinal artery. It presents with different features on the type of tract that is involved.
- Tabes Dorsalis- This is a manifestation of tertiary syphilis. It involves the dorsal column and the dorsal roots.
- Posterior Cord Syndrome - This is a very rare condition that results from the involvement of the posterior spinal artery; this is the only condition that involves the dorsal part of the spinal cord as the posterior spinal artery supplies it. The anterior spinal artery supplies the ventral portion of the spinal cord.[9]
- Vitamin B12 deficiency - A deficiency of vitamin B12 causes deficits in the spinocerebellar, the corticospinal, and the dorsal column pathway. [10]
- Paramedian artery occlusion - This rare condition can result from the occlusion of the paramedian arteries which supply the medial basal pons, the pontine nuclei, corticospinal fibers, and the medial lemniscus as they ascend through the brainstem. Any lesion here will cause a disturbance in these structures.
- Raymond Cestan Syndrome - This condition is also known as an upper dorsal pontine syndrome. It is the result of occlusion of the long circumferential branches of the basilar artery.
- Dorsal Midbrain Syndrome - Can be the result of occlusion of the paramedian branches of the basilar artery. It can involve the medial lemniscus if the occlusion has a lateral extension.
- Thalamic Strokes - The thalamus contains the third-order neurons of the dorsal column medial lemniscus pathway, and any lesion to the posterior cerebral artery can cause a problem with the thalamus.
Media
(Click Image to Enlarge)
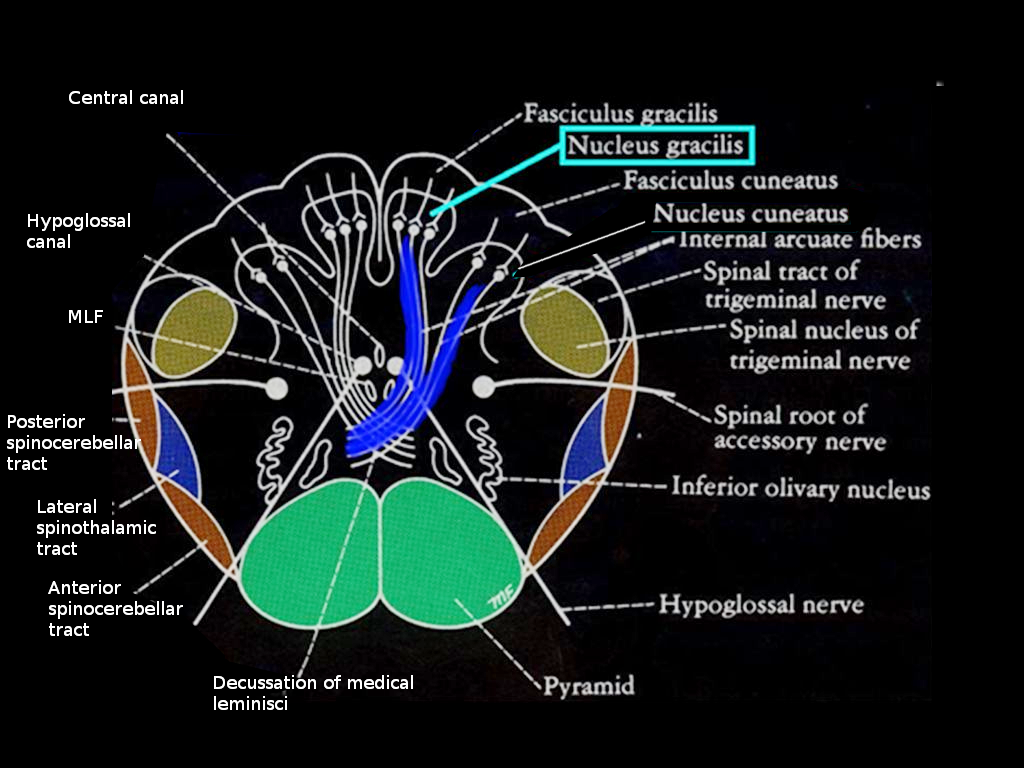
Nucleus gracilus Image courtesy O.Chaigasame
References
Romanowski CA, Hutton M, Rowe J, Yianni J, Warren D, Bigley J, Wilkinson ID. The Anatomy of the Medial Lemniscus within the Brainstem Demonstrated at 3 Tesla with High Resolution Fat Suppressed T1-Weighted Images and Diffusion Tensor Imaging. The neuroradiology journal. 2011 May 15:24(2):171-6 [PubMed PMID: 24059604]
Kubota C, Nagano T, Baba H, Sato M. Netrin-1 is crucial for the establishment of the dorsal column-medial lemniscal system. Journal of neurochemistry. 2004 Jun:89(6):1547-54 [PubMed PMID: 15189358]
Level 3 (low-level) evidenceLi D, Jiao YM, Wang L, Lin FX, Wu J, Tong XZ, Wang S, Cao Y. Surgical outcome of motor deficits and neurological status in brainstem cavernous malformations based on preoperative diffusion tensor imaging: a prospective randomized clinical trial. Journal of neurosurgery. 2018 Mar 16:130(1):286-301. doi: 10.3171/2017.8.JNS17854. Epub [PubMed PMID: 29547081]
Level 1 (high-level) evidenceWillis WD Jr, Westlund KN. The role of the dorsal column pathway in visceral nociception. Current pain and headache reports. 2001 Feb:5(1):20-6 [PubMed PMID: 11252134]
Level 3 (low-level) evidenceHong D, Andrén-Sandberg A. Punctate midline myelotomy: a minimally invasive procedure for the treatment of pain in inextirpable abdominal and pelvic cancer. Journal of pain and symptom management. 2007 Jan:33(1):99-109 [PubMed PMID: 17196911]
Campero M, Hughes R, Orellana P, Bevilacqua JA, Guiloff RJ. Spinal cord infarction with ipsilateral segmental neuropathic pain and flaccid paralysis. A functional role for human afferent ventral root small sensory fibres. Journal of the neurological sciences. 2018 Dec 15:395():84-87. doi: 10.1016/j.jns.2018.09.037. Epub 2018 Oct 1 [PubMed PMID: 30300819]
Grundy L, Erickson A, Brierley SM. Visceral Pain. Annual review of physiology. 2019 Feb 10:81():261-284. doi: 10.1146/annurev-physiol-020518-114525. Epub 2018 Oct 31 [PubMed PMID: 30379615]
Al-Chalabi M, Reddy V, Alsalman I. Neuroanatomy, Posterior Column (Dorsal Column). StatPearls. 2023 Jan:(): [PubMed PMID: 29939665]
Cochrane M, Hess M, Sajkowicz N. Posterior cord syndrome associated with postoperative seroma: The case to perform a complete neurologic exam. The journal of spinal cord medicine. 2020 Nov:43(6):892-894. doi: 10.1080/10790268.2018.1550598. Epub 2018 Dec 14 [PubMed PMID: 30547736]
Level 3 (low-level) evidenceDobson R, Alvares D. The difficulties with vitamin B12. Practical neurology. 2016 Aug:16(4):308-11. doi: 10.1136/practneurol-2015-001344. Epub 2016 Mar 23 [PubMed PMID: 27009308]