Introduction
Rheumatoid arthritis (RA) is an immune-mediated multisystem inflammatory disease that predominantly affects the synovial joints. It was first described by Alfred Baring Garrod in the year 1800. The disease can lead to inflammation, joint destruction, deformity, and disability, and may also present with extra-articular manifestations. Inflammatory arthritis involving the small joints of the hands is the most common initial presentation in rheumatoid arthritis. Hand joints commonly involved are the metacarpophalangeal joints, the proximal interphalangeal joints, and the wrist joints. In RA, the arthritis is typically bilateral and symmetrical. Other joints that can be affected in RA are the knees, ankles, elbows, shoulders, metatarsophalangeal joints, the cervical spine, and the temporomandibular joints.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of rheumatoid arthritis is multifactorial. The combination of a number of genetic risk factors, environmental factors, and abnormal immune response constitutes the basis for the approved pathogenic theories. Genetic risk factors include HLA-DRB1-shared epitope, non-HLA genetic risk factors (PTPN22, TRAF1-C5, STAT4, TNFAIP3, and PADI4), epigenetic transformation, and generation of antigenic epitopes.
Non- genetic risk factors include female sex, smoking, microbiota, western diet, stress, infections, environmental and ethnic factors. Immuno-pathogenic theories in rheumatoid arthritis include the generation of new antigenic epitopes as a result of a triggering factor mostly environmental that leads to epigenetic transformation and autoimmunity.[1]
Epidemiology
Rheumatoid arthritis is one of the most common inflammatory arthritides. Data regarding the global prevalence remain insufficient, and the latest published prevalence rates range from 0.5% to 1% with regional variations. A higher incidence has been reported for Northern Europe and North America within the incidence of 24 to 36 cases per 100,000.[4] One of the main setbacks is that most of the incidence and prevalence rates have been reported using the older 1987 American College of Rheumatology classification criteria for rheumatoid arthritis, and date of using the 2010 American College of Rheumatology classification criteria for rheumatoid arthritis is scant. Peak prevalence is observed between the ages of 30 and 50 years (may occur at any age) with a later age of onset reported for males. The disease is more prevalent in females, with a female to male ratio of 2 to 1 to 3 to 1. The concordance rate for RA is 12% to 15% and 2% to 3% in monozygotic twins and fraternal twins, respectively.[5]
Pathophysiology
The complex pathogenetic pathways in rheumatoid arthritis involve both the innate and adaptive immune system activation and involvement of several cells including T-cells, B-cells, macrophages, dendritic cells, neutrophils, fibroblasts, chondrocytes, and mast cells. The exact pathophysiological mechanisms involved in rheumatoid arthritis are still not completely understood. An interplay between genetic and environmental risk factors leads to autoimmunity and altered immune system. Molecular mimicry, epigenetic transformation, and cross-reactivity are additional possible theories. Citrullination, carbamylation, and methylation are important theories in rheumatoid arthritis that lead to the production of new antigenic epitopes and autoantibodies to citrulline and rheumatoid factor in seropositive patients.[1]
The innate and adaptive immune systems react to these antigenic epitopes by activation of Toll-like receptors (TLRs). Upon exposure to an antigenic stimulus, cells of the innate system, including monocytes, macrophages, and dendritic cells, express TLRs which initiate and promote a cascade of inflammatory events. Macrophages and dendritic cells engulf and process the antigenic peptides, which is followed by migration to the peripheral lymphoid tissue where they present these antigenic epitopes to the adaptive immune system. Antigen presentation to T lymphocytes promotes T cell differentiation with resultant activation of cellular immunity and the subsequent release of proinflammatory cytokines, including the Tumor necrosis factor-alpha, transforming growth factor β, interleukin (IL)-1β, IL-6, IL-21, and IL-23. The T-B cell signaling pathways promote B lymphocyte activation with the production of autoantibodies to rheumatoid factor and citrulline that lead to the systemic and articular disease process.
The immune drive is further associated with the expression of adhesion molecules and the chemotaxis of neutrophils into the synovium, release of chemokines by the activated endothelial cells of synovial microvasculature that leads to inflammatory synovitis and synovial thickening. The thickened synovial tissue becomes hypoxic due to the proliferation of synovial cells and increased fluid volume in the synovium with a reduction of the capillary flow. This all together promotes angiogenesis and pannus formation.[6][7][8]
Histopathology
Chronic inflammation leading to joint damage and destruction is the hallmark of rheumatoid arthritis. Inflammed synovium in rheumatoid arthritis is thickened and hypertrophied, and consists of an inflammatory infiltrate consisting of T-cells, B-cells, macrophages, plasma cells, dendritic cells, and neutrophils. The histopathology may simulate a granulomatous structure rich in macrophages and plasma cells, giant cells, lymphoid follicles, and the development of areas of fibrinoid necrosis with longstanding uncontrolled disease.[9]
The classic histologic feature of rheumatoid arthritis, the pannus consisting of fibroblasts, macrophages, lymphocytes, and osteoclast-like cells, can form at the interface of bone/cartilage and synovium and is thought to play a role in bone destruction and erosions by invading the bone and cartilage. Rheumatoid nodules exhibit palisading granulomas on histopathology, with central fibrinoid necrosis surrounded by palisading histiocytes, multinucleated giant cells, lymphocytes, and fibroblasts.
History and Physical
Preclinical Disease
Several studies have demonstrated preclinical stages for rheumatoid arthritis several years before they fulfill the diagnostic criteria for rheumatoid arthritis. In patients with genetic risk factors, rheumatoid arthritis specific autoantibodies become positive 10-15 years before a patient develops clinical features of rheumatoid arthritis during which the patient is asymptomatic.[10][11][6]
This asymptomatic seropositive preclinical stage may then be followed by many years of symptoms such as palindromic rheumatism or arthralgia before a patient fulfills the diagnostic criteria for rheumatoid arthritis. There is ongoing research involving individuals in the preclinical stages of rheumatoid arthritis who are at higher risk of future development of the clinically apparent disease.
Disease Patterns
The hallmark of RA is chronic bilateral symmetric inflammatory arthritis (synovitis) involving the small joints of the hands and feet. More than 50% of the cases of RA have an insidious onset of the disease, while abrupt onset can be seen in up to 25% cases. Monoarticular joint involvement, especially that of larger joints such as knee or shoulder that eventually progresses to polyarticular involvement, has been seen. In the elderly population, the onset of RA may mimic symptoms of polymyalgia rheumatica with arthralgias, myalgias, and stiffness of the shoulders and hip girdles with elevated ESR and constitutional symptoms such as fever and fatigue.[12] Rarely, extra-articular manifestations, especially rheumatoid nodulosis or interstitial lung disease in addition to seropositivity, can be the initial presenting feature of RA.
Regardless of the pattern of onset, most patients experience gradual progression of the disease if left untreated, although some patients may experience episodic/palindromic pattern or a brief self-remitting pattern. Although the severity of RA may fluctuate over time, spontaneous remission in RA is uncommon, especially if left untreated after the first 3-6 months.[13][14][15]
RA tends to involve small joints of bilateral upper and lower extremities. In the hands, the most commonly involved joints are the metacarpophalangeal (MCP) joints and the proximal interphalangeal (PIP) joints, especially the 2nd and 3rd MCP and PIP joints. Distal interphalangeal (DIP) joints are usually spared, and involvement of the 1st carpometacarpal joint is less common. In the feet, the most commonly involved joints are the metatarsophalangeal (MTP) joints. The involvement of the wrist, elbow, shoulder, the knee has, and hip joints are also frequent. Axial involvement includes C1-C2 synovitis, erosion, and subluxation, although the rest of the spine and sacroiliac joints are spared.
History
The patients present with history typical for that of inflammatory arthritides, including joint pain, joint swelling, decreased strength, limited range of motion, and stiffness of the affected joints. The swelling is typically noted by the patients along with the metacarpophalangeal joint areas in the hands. The morning stiffness (gelling phenomenon) is usually experienced after prolonged periods of sleep (morning stiffness) or rest and lasts for more than 1 hour. The involvement of the small joints of the hands leads to an inability to perform daily activities such as opening a jar or wringing a washcloth. Due to the decreased strength, patients may report symptoms such as “frequently dropping a coffee mug.” Patients may experience difficulty in performing usual activities of daily living, such as taking a shower, combing hair, dressing, or using handgrips to unlock doors.
Patients usually experience constitutional symptoms such as fatigue and malaise. Weight loss and low-grade fevers may also accompany the onset of rheumatoid arthritis and flares of rheumatoid arthritis. A Positive family history of inflammatory joint disease or other autoimmune collagen vascular disease is usually present in up to 50% of cases, especially among first-degree relatives.
Physical Examination
The most commonly involved hand joints in RA are the MCP and PIP joints. The DIP joints are usually spared. Wrist joint involvement is also very common.
Synovitis
The key clinical finding in RA is that of palpable synovial hypertrophy or synovitis. On inspection, the joints appear swollen with fusiform /spindle-shaped appearance of the PIP joints. The range of motion can be evaluated by the assessment of handgrip and hand curl, which is usually compromised due to synovitis. Grip strength may be reduced, and a sphygmomanometer can be used to objectively measure the strength. Contrary to the hard bony feeling of osteoarthritic changes, the RA synovitis has a soft “doughy” feeling. Other changes of inflammation such as erythema and warmth may or may not be present, although tenderness is usually present.
In the wrist joints, synovitis can easily be palpable using the two thumb technique by applying pressure at the radiocarpal joint line, which is about 1 cm distal to the lister’s topical. The range of motion of the wrist joint can be evaluated by flexion/extension and pronation/supination of the wrists.
Tenosynovitis
The flexor tendons of the hands are frequently involved by the tenosynovitis leading to swelling and thickening of these tendons. This can cause triggering and locking of the fingers. The tendons may be nodular and thickened on palpation. The presence of flexor tenosynovitis suggests a poor prognosis.
A common feature of rheumatoid arthritis involving the wrist joints includes the presence of tenosynovitis involving the extensor tendons. Extensor carpi ulnaris is frequently involved, and synovial proliferation around the ulnar styloid can be associated with erosions of the ulnar styloid. Extensor tendon compartment tenosynovitis can lead to swelling extending up to the metacarpal joints, which gets accentuated with the extension of the fingers. Tenosynovitis and tenosynovial effusions of the flexor tendons at the wrist joint can lead to compression of the median nerve at the carpal tunnel leading to symptoms of carpal tunnel syndrome.
Hand and Wrist Deformities
Irreversible damage is the sequelae of ongoing synovitis. Several deformities have been described as secondary to rheumatoid arthritis.
Boutonnière deformity: There is hyperflexion of the PIP joint and hyperextension of the DIP joint, occurring due to damage to the central extensor tendon due to tenosynovitis. The weakening of the extensor tendon leads to dorsal displacement of the PIP joint, which causes the lateral and volar displacement of the lateral bands of the extensor tendon. The shortening of the lateral bands leads to hyperextension of the DIP joint.
Swan-neck deformity: There is hyperextension of PIP and hyperflexion of the DIP joint, secondary to dorsal subluxation of the lateral bands of the central extensor tendon along with volar displacement of the PIP joint and dorsal displacement of the DIP joint. As with the Boutonnière deformity, the shortening of the tendon leads to hyperextension of the PIP joint and hyperflexion of the DIP joint.
Subluxation of the MCPs: Dorsal displacement of the head of the metacarpal and volar and proximal displacement of the proximal head of the proximal phalanx gives an appearance of chronically swollen MCP joints. This happens due to the contraction of the flexors (intrinsic muscles) of the MCPs, with flexion contracture of the corresponding MCP joint.
Ulnar drift or ulnar deviation: this deformity develops as a complication to weakening with laxity or erosion of the extensor carpi ulnaris tendon overlying the ulnar styloid process. This promotes the antagonist muscle on the radial side to take the upper hand with radial deviation at the wrist and ulnar deviation of the fingers supported by gravity.
Hitchhiker thumb or the Z deformity: Hyperextension of the interphalangeal joint of the thumb with flexion of the MCP along with exaggerated adduction of the 1st metacarpal leads to a flail thumb with the inability to flex the interphalangeal joint leading to inability to pinch using the thumb.
Piano key sign or floating ulnar styloid: Damage to the radioulnar ligament leads to this deformity where the ulnar styloid moves up and down on applying pressure.
Subluxation of the wrist: Erosions and chronic synovitis can lead to the volar subluxation of the distal wrist.
Vaughan-Jackson deformity: Extensor tendon rupture involving the 3rd, 4th, and 5th digits leads to the inability to extend these fingers. Chronically tenosynovial inflammation at the wrist joint and chronic rubbing of these tendons, along with the damaged ulnar styloid, needs to their rupture at the wrist. This is considered a surgical emergency.
Subcutaneous Nodules
Usually seen in seropositive RA, subcutaneous rheumatoid nodules, which are an extra-articular manifestation of RA, developed most commonly on pressure areas such as the dorsal aspect of the finger joints. They can be seen in the wrists, more commonly along the dorsal and medial aspect. On palpation, they are firm, contender, and not freely mobile. They may or may not regress with treatment for RA. On the contrary, methotrexate-induced accelerated rheumatoid nodulosis has been well described. The presence of subcutaneous rheumatoid nodules early in the course of the disease is a poor prognostic marker and is considered a higher risk for the development of other extra-articular manifestations of RA.
Evaluation
In a suspected case of rheumatoid arthritis in addition to proper history taking and clinical examination, it is of utmost importance to confirm the diagnosis and evaluate the patient by laboratory and radiographic investigations.
Laboratory
Markers of Inflammation
- An abnormally high level of erythrocyte sedimentation rate (ESR) and/or C reactive protein (CRP) are associated with disease activity and progression.[16][17]
Hematologic Changes
- Anemia of chronic disease is one of the most common extra-articular manifestations of RA. Leukopenia and thrombocytopenia can be seen in RA secondary to the development of Felty syndrome. Mild leukocytosis and/or thrombocytosis may be associated with disease activity.
- Patients with RA are also at a high risk of non-Hodgkin lymphoma, which may manifest as the presence of lymphocytosis, thrombocytopenia, and atypical lymphocytes.
Immunologic Parameters
- Rheumatoid Factor (RF)
RF is an immunoglobulin (Ig) autoantibody directed against the Fcγ chains of IgG. The most commonly tested immunoglobulin subclasses of RF are IgM and IgA, although IgG and rarely, IgD and IgE subclasses of RF can be seen in some cases. In RA, RF is present in approximately 60-90% of patients and can be present several years before the clinical onset of RA.[18] RF is not specific for RA as 20% to 30% of patients with RA are negative for RF, although higher titers of RF increase its specificity for RA. A high titer of RF carries a prognostic value and is associated with more erosive joint disease, extra-articular manifestations, and greater functional disability. The presence of RF predicts radiographic progression of bone erosions, independent of disease activity.[16][17] Titers of RF may decline with the treatment of RA, specifically with B-cell directed therapies such as rituximab.
RF can be seen in other autoimmune connective tissue diseases such as Sjogren syndrome, systemic lupus erythematosus, mixed connective tissue disease, cryoglobulinemic vasculitis, and polyarticular juvenile idiopathic arthritis. Chronic inflammatory/infectious conditions such as tuberculosis, chronic osteomyelitis, hepatitis B and C, bacterial endocarditis, fibrosing alveolitis, and silicosis can also be associated with the production of RF. Further, 5% to 8% of healthy individuals can have RF positivity.
- Antibodies to citrullinated protein and peptide antigens (ACPAs)
The process of deimination of arginine residues in the proteins such as fibrin, vimentin, filaggrin by deiminase enzymes produced during inflammation is termed citrullination. Autoantibodies against these citrullinated proteins and peptides (ACPAs) can be detected in RA patients using ELISA and immunoblotting methods. Anti-cyclic citrullinated peptides autoantibodies (anti-CCP) are the most commonly available, although other autoantibodies such as antibodies against citrullinated vimentin and mutated citrullinated vimentin (anti-MCV) can also be present in RA.
Like RF, ACPAs can be present up to 10 years before the clinical onset of RA.[18] They have less sensitive compared to RF and are positive in 50% to 60% of patients with early RA, although sensitivity can increase to up to 80% in late disease. They are more specific than RF with a specificity of more than 90%. Up to 25% of patients with RA who are negative for RF are positive for ACPAs. Smoking has shown to have a positive correlation with positive ACPAs.[19] ACPA-positive patients may have a more erosive RA disease course than ACPA-negative patients.[16][17]
- Antinuclear antibodies (ANA)
ANAs may be present in approximately 40% of patients with RA, although other anti-extractable nuclear antibodies to most nuclear antigen subsets are usually negative. Patients who have secondary Sjogren syndrome associated with RA may have more specific antinuclear antibodies such as Anti-SSA and Anti-SSB.
- Antineutrophil cytoplasmic antibodies (ANCAs)
Up to 25% of patients with RA can have positive ANCA, more commonly P-ANCA.[20][21] The Presence of P- ANCA in RA has been associated with more lung involvement.
Imaging
Plain Radiographs
Plain radiographic findings in the hands of patients with RA may take months to develop. An early finding on x-rays is that of periarticular osteopenia, which may later be followed by more diffuse osteopenia. Soft tissue swelling due to joint effusions and synovitis can be seen early as well. The Hallmark radiographic finding of RA is that of periarticular erosions.Bone erosions typically develop on the radial aspect of the bone surface the so called bare areas of the bone where the synovium directly ovelries the bone surface. [22] Hands are one of the earliest sites to develop these radiographic changes in RA, with earliest erosions usually developing in the 2nd MCP joint and in the carpus, especially near the ulnar styloid. The erosions are usually subtle to start but maybe frankly visible on radiographs as the disease progresses. With disease progression, symmetric joint space loss due to cartilage destruction, alignment, and deformities occur. Joint ankylosis, especially of the carpus, can be seen in later stages of the disease as well.
Magnetic Resonance Imaging (MRI)
MRI provides a more accurate estimate of articular involvement, especially early and may show up to 40% more erosions than conventional radiography. Radiographic diagnosis should apply only in the presence of clinical features of joint inflammation as MRI may reveal erosive changes in 2-9% of healthy individuals with osteoarthritis.
Musculoskeletal Ultrasound (MSK US)
MSK US is recently used as a useful bedside imaging modality for early diagnosis of synovitis and monitoring disease activity in RA. A synovial hypertrophy score ≥ 2 by greyscale (GS) and a power Doppler (PD) score ≥ 1 may be a sign of inflammatory activity. US can help to detect early cortical erosions that are difficult to diagnose early using plain radiography.[23][24][25][16][25]
Classification Criteria
The initial classification criteria for RA were designed by the American College of Rheumatology in 1987, which had a sensitivity of 77% to 95% and a specificity of 85% to 98%.[26][27] With the recent advancements in the diagnosis and management of RA, the American College of Rheumatology and European League Against Rheumatism (ACR/EULAR) proposed new classification criteria in 2010 with the goal of early disease detection.[28] Variation studies comparing both these criteria have demonstrated similar specificity and sensitivity of the 2010 ACR/EULAR classification criteria, with the ability to classify more patients with the early disease with the 2010 ACR/EULAR criteria.[29][30]
2010 ACR/EULAR classification criteria for Rheumatoid Arthritis[28]
Target Population
- Newly presenting patients who have at least one joint with synovitis/swelling, AND there is no other existing explanation of the joint synovitis/swelling.
Definition Used
- Joint involved: any swollen or tender joint (excluding the distal interphalangeal joints of hands and feet, the first metatarsophalangeal joints, and the first carpometacarpal joints) on clinical examination; additional evidence from MRI or ultrasonography may be used to identify additional joints.
- Large joints: shoulder, elbow, hip, knee, or ankle.
- Small joints: metacarpophalangeal joint, proximal interphalangeal joint, 2 to 5th metatarsophalangeal joints, interphalangeal joint of the thumb and wrist.
- Other joints: temporomandibular joint, sternoclavicular joint, acromioclavicular joint, and others, as reasonably expected in RA
- Symptom duration: The patient’s self-reported maximum duration of signs and symptoms of synovitis of any joint that is clinically involved at the time of assessment
- Negative serology: Value less than or equal to the upper limit of the normal reference range for the laboratory assay
- Low positive serology: Value more than 1–3 times the upper limit of the normal reference range for the laboratory assay
- High positive serology: Value more than three times the upper limit of the normal reference range for the laboratory assay
- At least one serological assay result is needed for classification.
- Normal/abnormal acute phase reactants: C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) values as determined by the local laboratory reference.
- At least one acute phase reactant result is needed for classification.
Interpretation
A score of ≥6 points is required for classification as definite rheumatoid arthritis (RA).[28]
Joint Involvement and Distribution: 0–5 points
- 1 large joint: 0 points
- 2–10 large joints: 1 point
- 1–3 small joints (with or without large joints): 2 points
- 4–10 small joints (with or without large joints): 3 points
- >10 joints (of which ≥1 is a small joint, rest can be small/large/other joints): 5 points
Symptom Duration: 0–1 Points
- <6 weeks: 0 points
- ≥6 weeks: 1 point
Serology: 0–3 Points
- Negative for RF and negative for ACPA: 0 points
- Low-positive for RF or low-positive for ACPA: 2 points
- High-positive for RF or high-positive for ACPA: 3 points
Acute-phase Reactants: 0–1 Point
- Normal CRP and ESR levels: 0 points
- Abnormal CRP levels or abnormal ESR: 1 point
Disease Activity Assessment
Disease activity and physical function assessment is an important step in the management of RA. Over the past several years, there have been significant advancements in improving disease activity indices.
Markers of Inflammation
- ESR and CRP are the most commonly used markers of inflammation, and while they add objectivity to disease activity assessment and tend to correlate with swollen joint counts (especially CRP), they lack sensitivity and specificity, and may be abnormal due to non-RA related reasons, or maybe normal despite active RA in some cases.
Patient-Reported Outcomes
- Health Assessment Questionnaire (HAQ): Physical function assessment is one of the most important tools that correlate well with long term prognosis in RA. This includes multiple questions about patients’ ability/inability to perform activities of daily living. Multiple tools have been proposed for physical function assessment, including Arthritis Impact Measurement Scale (AIMS), clinical HAQ (CLINHAQ), Euro-QoL 5-D (EQ-5D), and several modifications have been made to the HAQ tool. The modified HAQ (HAQ-II) is the most widely used tool.
- Pain: Pain level assessment can be performed using a horizontal visual analog scale (VAS) ranging from 0 to 100mm or 0 to 10cm.
- Fatigue: Similar to pain level, fatigue assessment can be performed using a horizontal VAS ranging from 0 to 100mm or 0 to 10cm.
- Patient global assessment of disease activity (PGA): This is a subjective evaluation of their disease activity by the patient-rated on a horizontal VAS ranging from 0 to 100mm or 0 to 10cm.
- Routine Assessment of Patient Index Data 3 (Rapid3): This is the total of patient-reported HAQ, Pain-VAS, and PGA-VAS. Rapid3 has been validated and has reported correlating well with other RA-composite indices.
Physician Reported Outcomes
- Tender joint count (TJC) and swollen joint count (SJC): Many joint count assessments have been described in the literature, each with limitations. The 28-joint count assessment for TJC and SJC is the most widely performed and validated. This count is a total number of joints tender (TJC) and swollen (SJC) on examination, and includes the most commonly involved joints by RA including MCPs, PIPs, wrists, elbows, shoulders, and knees. A drawback is the exclusion of feet/ankles, which are frequently involved in RA as well.
- Physician (MD or evaluator) global assessment of disease activity (MDGA or EGA): This is an objective evaluation of the disease activity by the physician/evaluator rated on a horizontal VAS ranging from 0 to 100mm or 0 to 10cm.
Composite Indices
Keeping in mind the limitations of and disparities between the patient-reported and physician-reported measures, several composite indices have been proposed and validated. These can be rapidly performed in the clinic and can serve as good measures for point of care disease activity assessment, as well as longitudinal disease activity assessment to evaluate improvement or worsening in disease activity.
- Disease Activity Score (DAS)-ESR
- Disease Activity Score (DAS)-CRP
- Disease Activity Score (DAS)28-ESR
- Disease Activity Score (DAS)28-CRP
- Simplified Disease Activity Index (SDAI)
- Clinical Disease Activity Index (CDAI)
- Rapid Assessment of Disease Activity in Rheumatology (RADAR)
- Rheumatoid Arthritis Disease Activity Index (RADAI)
Treatment / Management
Pharmacological Management
Although there is no cure, over the past two decades, there have been remarkable improvements in treatment and management strategies for rheumatoid arthritis, especially with the advent of the biological disease-modifying anti-rheumatic drugs (DMARDs). American College of Rheumatology recommends a treat-to-target strategy, with the goal to achieve and maintain complete remission. Prevention of radiographic progression and joint deformities and prevention and early management of the extra-articular disease are important goals as well.[31]
There are several medications available for the management of RA; however, to date, there is no clinical, laboratory, or radiographic parameter that can predict a favorable response to any particular therapy. Decision making shall consider RA disease activity, patient comorbidities, and patient preference. Several treatment strategies including sequential monotherapy, step-up therapy, and step-down therapy have been evaluated. While step-up therapy is the most commonly used, recent studies favor the use of aggressive therapy early in the disease with step down once remission is achieved.[32][33][34] Further, while monotherapy can be used in patients with low disease activity during initiation of therapy, several studies have shown the superiority of combination therapy in RA in preventing progression.(A1)
With the recent advancements in the available treatment options with the introduction of highly specific and effective biological DMARDs, the use of older therapeutic agents such as gold, penicillamine, minocycline, doxycycline is no longer encouraged. Non-steroidal anti-inflammatory agents (NSAIDs) can provide short term symptom relief but are not associated with the prevention of disease progression, and their adverse effect profile with long term use prohibits their use as long-term management options for RA.[35] Similarly, long-term use of corticosteroids, especially moderate-high doses shall be discouraged.[36][37][38] (B3)
ACR recommends using corticosteroids only during the early management phase and in the lowest possible dose for the shortest possible duration. Other immunosuppressive agents such as azathioprine and cyclosporine are no longer the treatments of choice for RA given the availability of more effective and safer alternatives, although these may be used in special circumstances (such as azathioprine in interstitial lung disease).
Available DMARDs can be classified into conventional synthetic DMARDs (cs-DMARDs) and biologic DMARDs (b-DMARDs).
The cs-DMARDs include Methotrexate (MTX), Leflunomide (LFN), Sulfasalazine (SSZ), and Hydroxychloroquine (HCQ). Methotrexate is the preferred c-DMARD given the significant data on its efficacy. These cs-DMARDs can take weeks to months to show clinical efficacy.[39][40][41][42] Each one of the above DMARDs induces its’ effect via drug-specific immune modulatory effect. They can be used as monotherapy (most commonly, monotherapy with MTX), in combination with other cs-DMARDs (eg. Triple therapy involving HCQ, MTX, and SSZ) or in combination with b-DMARDs. The cs-DMARDs can be associated with several adverse effects, and frequently require close laboratory monitoring during the course of management.[43][44][45](A1)
The b-DMARDs are highly specific genetically engineered drugs that target specific pathways of the immune system. B-DMARDs can be used as first-line therapy or after the failure of cs-DMARDs therapy in case of ongoing disease activity with evidence of clinical or radiographic disease progression. B-DMARDs can be used as monotherapy or in combination with other cs- DMARDs for better control of disease activity but cannot be used in combination with other b-DMARDs due to lack of additional efficacy and more adverse effects. Targeted synthetic DMARDs are non biological small molecules that have been developed to address cytokine functions at the transcrptional level via inhibition of the Janus Kinases therby interrupting intracellular cytokine signalling pathways.
B-DMARDs include:
- Tumor necrosis factor (TNF-alpha) inhibitors[46]
- Infliximab
- Etanercept
- Adalimumab
- Certolizumab
- Golimumab
- Interleukin-6 inhibitors
- Tocilizumab
- Sarilumab
- B-cell depleting therapies
- Rituximab
- T-cell co-stimulation inhibition
- Abatacept
- Interleukin-1 inhibitors
- Anakinra
Targeted Synthetic DMARDs- Janus Kinase inhibitors include: [47][48][49]
- Tofacitinib
- Upadacitinib
- Baricitinib
TNF-α inhibitors are among the first prescribed b-DMARDs.[46] As with cs-DMARDs, choice of b-DMARDs takes into account patient comorbidities and contraindications to specific b-DMARDs, and patient preference of the route of administration. Patients planning to initiate therapy with b-DMARD shall be screened for tuberculosis and hepatitis B/C and other infections due to increased infection risk posed by these agents including bacterial, fungal, and viral infections. Rare events include bone marrow suppression and hepatotoxicity and close laboratory monitoring is recommended during the course of treatment. Other investigational therapies include gene therapy, stem cell, and bone marrow transplant therapy although more data is needed regarding their potential application for the management of RA.
A summary of the keypoints provided by the updated American College of Rheumatology 2021 therapeutic recommendtaions for the management of Rheumatoid arthritis: [50]
- Target is remission.
- Attaining at least low disease activity can be conditionally recommended over remission.
- The addition /switching to DMARDs is conditionally recommended over continuation of oral and/or intraarticular glucocorticoids in RA patients who require glucocorticoids to remain at target.
- Methotrexate is strongly recommended as a monotherapy over other conventional DMARDs and leflunomide monotherapy for DMARDs-naive RA patients with moderate- to- high disease activity.
- Methotrexate is strongly recommended as a monotherapy over biologic DMARDs (bDMARDs) or targeted synthetic DMARDs (tsDMARDs) monotherapy for DMARDs- naive RA patients with moderate- to- high disease activity.
- Methotrexate as a monotherapy is conditionally recommended over dual or triple conventional synthetic DMARDs in DMARDs- naive RA patients with moderate- to- high disease activity.
- Methotrexate as a monotherapy is conditionally recommended over the use of methotrexate with a tumor necrosis factor (TNF) inhibitor in DMARDs- naive RA patients with moderate- to- high disease activity.
- Methotrexate as a monotherapy is strongly recommended over methotrexate with a non– TNF inhibitor biologic DMARD or targeted synthetic DMARD for DMARDs- naive RA patients with moderate- to- high disease activity.
- The initiation of a csDMARD without the addition of short- term (<3 months) glucocorticoids is conditionally recommended over the addition of a short- term glucocorticoids for DMARD- naive RA patients with moderate- to- high disease activity.
- The initiation of a csDMARD without the additional use of longer-term (≥3 months) glucocorticoids is strongly recommended over the additional use of longer- term glucocorticoids for DMARD- naive RA patients with moderate- to- high disease activity.
- In DMARD-naive RA patients with low disease activity, methotrexate is conditionally recommended over leflunomide, sulfasalazine is conditionally recommended over methotrexate and hydroxychloroquine (antimalarial csDMARDs) is conditionally recommended over other conventional synthetic DMARDs.
- In RA patients moderate- to- high disease activity previously treated with csDMARDs, excluding methotrexate, Methotrexate monotherapy is conditionally recommended over the combination of methotrexate with a biologic or targeted synthetic DMARD.
- The use of oral methotrexate is conditionally recommended over the subcutaneous route for patients initiating methotrexate.
- Initiation/titration of methotrexate to at least 15 mg as a weekly dose within 4 to 6 weeks is conditionally recommended over initiation/titration to <15 mg weekly dose.
- For patients not tolerating oral weekly methotrexate a split oral dose of over 24 hours or weekly subcutaneous dose, and/or increasing the dose of folic/folinic acid, is conditionally recommended over switching other DMARDs.
- The treat-to-target approach is strongly recommended over traditional therapies in RA patients naieve to bDMARDs or tsDMARDs.
- In patients taking a maximum tolerated dose of methotrexate and didn't acheive target, adding on bDMARD or tsDMARD is conditionally recommended over the use of triple therapy approach (i.e., the addition of sulfasalazine and hydroxychloroquine).
- - In RA patients taking a bDMARD or tsDMARD without reaching goal of remission or low disease activity shifting to a bDMARD or tsDMARD of another different class is conditionally recommended over switching to the same class.
- The recommendations have also addressed the treatment modifications in the presence of specific situations or comorbidities. [50]
Non-pharmacological Management
A structured exercise program comprises an integral part of disease management protocols in RA. Patient education and support programs, physical therapy (thermo-therapy either heat or cold), transcutaneous electrical nerve stimulation (TENS), and rest during flare must be implemented and explained in RA. Physical exercises reduce fatigue scores and improve cardiovascular performance in stable RA patients. They exert a positive impact on cognition in RA patients. A structured exercise program should be an integral part of chronic disease management protocols for patients with RA. Occupational therapy can help to improve performance and maximize the quality of life including training of motor function, instructions for joint protection, the usage of assistive devices such as therapy gloves, splints, hand or wrists orthoses, electric jar, and can openers.
Occupational therapy to improve performance and maximize the quality of life including training of motor function, instructions for joint protection, the usage of assistive devices such as therapy gloves, splints, hand or wrists orthoses, electric jar, and can openers.[51][52](A1)
Surgical Interventions
With the recent advancements in the therapeutics, surgical intervention is rarely needed.
- For refractory cases, surgical interventions such as synovectomy, tenosynovectomy, tendon realignment, tendon transfer, joint replacement (arthroplasty), and joint fusion (arthrodesis) can be considered.
- Vaughan-Jackson deformity is considered a surgical emergency, with timely surgical intervention resulting in better outcomes and prevention of long-term disability.
- Removal of subcutaneous nodules is not routinely recommended due to increased risk of recurrence of nodules, and surgical complications such as infections and poor healing. However, nodules interfering with lifestyle such as on dominant hand interfering with fine motor function can be considered for removal.
- Carpal tunnel syndrome in RA, especially early in the disease course, usually responds to treatment of RA and resolution of wrist synovitis with rare cases needing surgical intervention.[53]
Differential Diagnosis
There is no single test that can diagnose rheumatoid arthritis with 100% certainty, and the diagnosis of RA shall be made clinically, taking into consideration the patient’s clinical presentation, laboratory/serological findings, and radiographic findings. Several diseases as mentioned below can mimic RA, although with history and physical examination along with laboratory and radiographic findings can help exclude the mimics.[54]
Infections
- Hepatitis B, hepatitis C, parvovirus B19, HIV
- Lyme disease
- Disseminated bacterial infections/septic arthritis
- Subacute bacterial endocarditis
Osteoarthritis
- Nodal osteoarthritis of the hands
- Erosive/inflammatory osteoarthritis of the hand
Seronegative Spondyloarthropathies
- Psoriatic arthritis
- Reactive arthritis
- Peripheral inflammatory arthritis associated with inflammatory bowel disease
- Ankylosing spondylitis with peripheral involvement
Crystalline Arthropathies
- Polyarticular gout
- CPPD arthropathy/pseudogout
Other Autoimmune Connective Tissue Diseases
- Systemic lupus erythematosus
- Sjogren syndrome
- Systemic sclerosis
- Mixed connective tissue disease
- Behçet’s disease
Other Diseases
- Hemochromatosis
- Relapsing polychondritis
- Sarcoidosis
- Hypertrophic osteoarthropathy
- Amyloid arthropathy
- Hemoglobinopathies (sickle cell disease)
- Hyperlipoproteinemias (types II, IV)
- Rheumatic fever[55]
- Langerhans cell histiocytosis
- Paraneoplastic inflammatory arthritis
- Inflammatory arthritis associated with immune checkpoint inhibitors
Prognosis
Factors that contribute to poor prognosis in rheumatoid arthritis include; a persistent elevation of inflammatory biomarkers including ESR and CRP, seropositivity to rheumatoid factor and ACPA particularly with high titers, Failure to respond with two or more of the disease-modifying drugs, erosive disease or persistent inflammation by radio imaging studies, strong family history, cigarette smoking, starting treatment late, high disease activity indices.[56]
Complications
Early intervention in rheumatoid arthritis may result in successful control of disease activity and improved functional performance. The major roadblock to an effective response to therapy might arise from disease-related or treatment-related multisystem complications such as cardiovascular, gastrointestinal diseases, osteoporosis, pulmonary involvement, recurrent infections, neoplastic disorders, renal and psychological complications. These comorbidities in addition to side effects of medications affect response to treatment, drug tolerability, and patient survival.[57]
Deterrence and Patient Education
A well-structured program in chronic disease that incorporated patient education, support programs, self-assessment indices, all with proper follow-up and recording comprises an integral part of chronic disease management protocols for patients with RA.[51][52]
Enhancing Healthcare Team Outcomes
RA contributes to significant comorbidity and disability in the affected individuals. A multidisciplinary management team composed of the rheumatologist, patient’s primary care physician, physiotherapist, and possibly other specialties, including nursing and pharmacists, shall work together to achieve a better outcome for patient safety and disease control. Patient education and self-management programs are of utmost importance. Regular patient assessment with the careful recording of medical data is also crucial to successful intervention and management.[52]
Media
(Click Image to Enlarge)
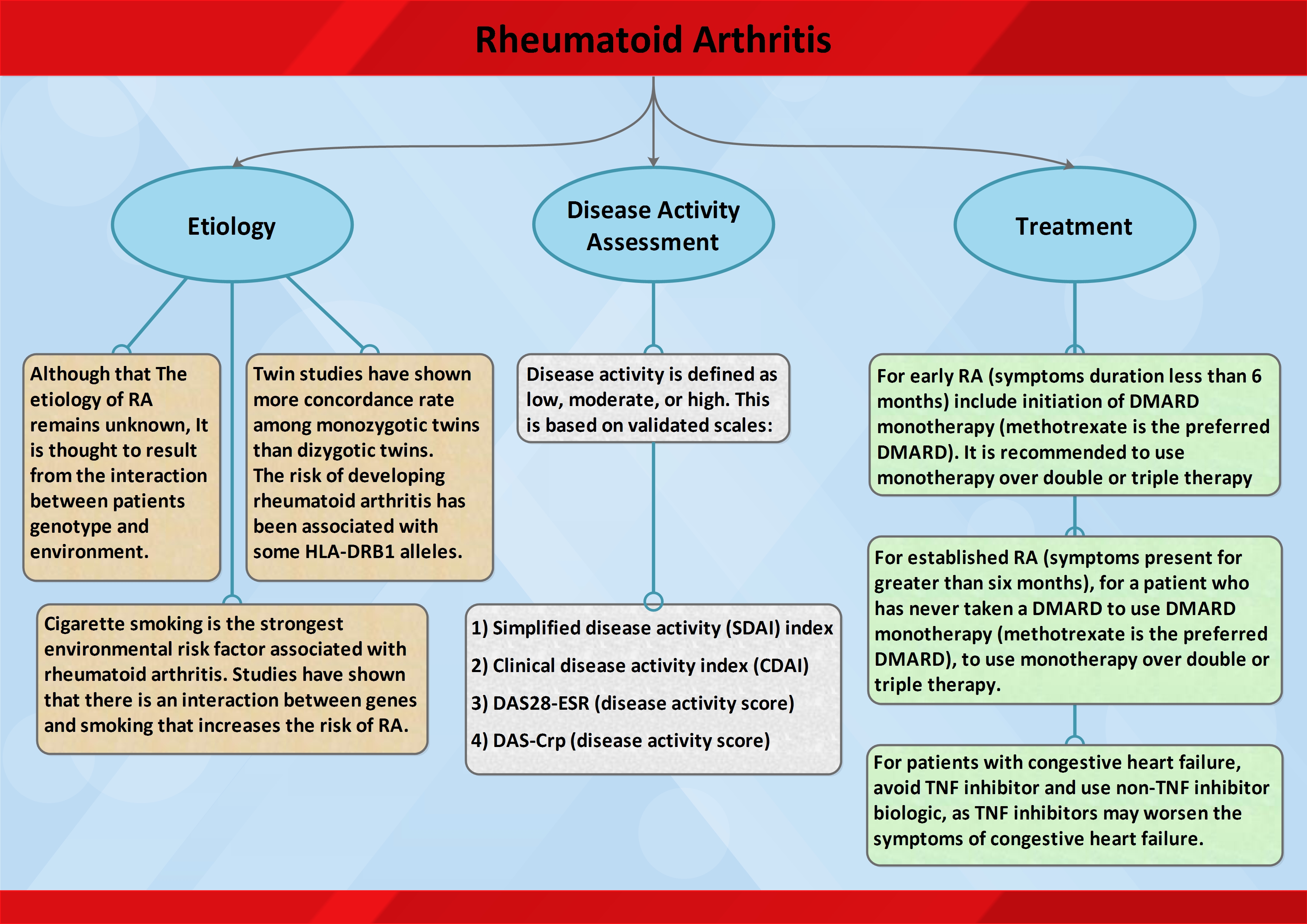
Summary keynotes on Rheumatoid Arthritis Contributed by StatPearls
(Click Image to Enlarge)

Ultrasound image of the thumb in a patient with a history of Rheumatoid Arthritis shows an abnormal amount of fluid within the flexor pollicus longus tendon sheath, consistent with an inflammatory tenosynovitis. Contributed by Mike Tall, MD
References
Guo Q,Wang Y,Xu D,Nossent J,Pavlos NJ,Xu J, Rheumatoid arthritis: pathological mechanisms and modern pharmacologic therapies. Bone research. 2018; [PubMed PMID: 29736302]
Cai Q,Xin Z,Zuo L,Li F,Liu B, Alzheimer's Disease and Rheumatoid Arthritis: A Mendelian Randomization Study. Frontiers in neuroscience. 2018; [PubMed PMID: 30258348]
Carbone F,Bonaventura A,Liberale L,Paolino S,Torre F,Dallegri F,Montecucco F,Cutolo M, Atherosclerosis in Rheumatoid Arthritis: Promoters and Opponents. Clinical reviews in allergy [PubMed PMID: 30259381]
Alamanos Y,Voulgari PV,Drosos AA, Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Seminars in arthritis and rheumatism. 2006 Dec [PubMed PMID: 17045630]
Level 1 (high-level) evidenceSilman AJ,Pearson JE, Epidemiology and genetics of rheumatoid arthritis. Arthritis research. 2002; [PubMed PMID: 12110146]
Nielen MM,van Schaardenburg D,Reesink HW,van de Stadt RJ,van der Horst-Bruinsma IE,de Koning MH,Habibuw MR,Vandenbroucke JP,Dijkmans BA, Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis and rheumatism. 2004 Feb [PubMed PMID: 14872479]
Level 2 (mid-level) evidenceLund-Olesen K, Oxygen tension in synovial fluids. Arthritis and rheumatism. 1970 Nov-Dec [PubMed PMID: 5495389]
Paleolog EM, Angiogenesis in rheumatoid arthritis. Arthritis research. 2002 [PubMed PMID: 12110126]
Level 3 (low-level) evidenceSmeets TJ,Dolhain RJ,Breedveld FC,Tak PP, Analysis of the cellular infiltrates and expression of cytokines in synovial tissue from patients with rheumatoid arthritis and reactive arthritis. The Journal of pathology. 1998 Sep [PubMed PMID: 9875143]
Deane KD,Norris JM,Holers VM, Preclinical rheumatoid arthritis: identification, evaluation, and future directions for investigation. Rheumatic diseases clinics of North America. 2010 May [PubMed PMID: 20510231]
Level 3 (low-level) evidenceGerlag DM,Raza K,van Baarsen LG,Brouwer E,Buckley CD,Burmester GR,Gabay C,Catrina AI,Cope AP,Cornelis F,Dahlqvist SR,Emery P,Eyre S,Finckh A,Gay S,Hazes JM,van der Helm-van Mil A,Huizinga TW,Klareskog L,Kvien TK,Lewis C,Machold KP,Rönnelid J,van Schaardenburg D,Schett G,Smolen JS,Thomas S,Worthington J,Tak PP, EULAR recommendations for terminology and research in individuals at risk of rheumatoid arthritis: report from the Study Group for Risk Factors for Rheumatoid Arthritis. Annals of the rheumatic diseases. 2012 May [PubMed PMID: 22387728]
Fleming A,Crown JM,Corbett M, Early rheumatoid disease. I. Onset. Annals of the rheumatic diseases. 1976 Aug [PubMed PMID: 970994]
Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet (London, England). 2016 Oct 22:388(10055):2023-2038. doi: 10.1016/S0140-6736(16)30173-8. Epub 2016 May 3 [PubMed PMID: 27156434]
Firestein GS, The disease formerly known as rheumatoid arthritis. Arthritis research [PubMed PMID: 25167330]
Smolen JS,Aletaha D,Barton A,Burmester GR,Emery P,Firestein GS,Kavanaugh A,McInnes IB,Solomon DH,Strand V,Yamamoto K, Rheumatoid arthritis. Nature reviews. Disease primers. 2018 Feb 8; [PubMed PMID: 29417936]
Marinou I,Maxwell JR,Wilson AG, Genetic influences modulating the radiological severity of rheumatoid arthritis. Annals of the rheumatic diseases. 2010 Mar; [PubMed PMID: 20124360]
van Leeuwen MA,van Rijswijk MH,van der Heijde DM,Te Meerman GJ,van Riel PL,Houtman PM,van De Putte LB,Limburg PC, The acute-phase response in relation to radiographic progression in early rheumatoid arthritis: a prospective study during the first three years of the disease. British journal of rheumatology. 1993 Jun; [PubMed PMID: 8508266]
Rantapää-Dahlqvist S,de Jong BA,Berglin E,Hallmans G,Wadell G,Stenlund H,Sundin U,van Venrooij WJ, Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis and rheumatism. 2003 Oct [PubMed PMID: 14558078]
Level 2 (mid-level) evidenceKlareskog L,Stolt P,Lundberg K,Källberg H,Bengtsson C,Grunewald J,Rönnelid J,Harris HE,Ulfgren AK,Rantapää-Dahlqvist S,Eklund A,Padyukov L,Alfredsson L, A new model for an etiology of rheumatoid arthritis: smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis and rheumatism. 2006 Jan [PubMed PMID: 16385494]
Level 2 (mid-level) evidenceCambridge G,Williams M,Leaker B,Corbett M,Smith CR, Anti-myeloperoxidase antibodies in patients with rheumatoid arthritis: prevalence, clinical correlates, and IgG subclass. Annals of the rheumatic diseases. 1994 Jan [PubMed PMID: 8311550]
Tur BS,Süldür N,Ataman S,Tutkak H,Atay MB,Düzgün N, Anti-neutrophil cytoplasmic antibodies in patients with rheumatoid arthritis: clinical, biological, and radiological correlations. Joint bone spine. 2004 May [PubMed PMID: 15182790]
Schett G,Gravallese E, Bone erosion in rheumatoid arthritis: mechanisms, diagnosis and treatment. Nature reviews. Rheumatology. 2012 Nov; [PubMed PMID: 23007741]
Level 3 (low-level) evidenceSahatçiu-Meka V,Rexhepi S,Manxhuka-Kërliu S,Rexhepi M, Radiographic estimation in seropositive and seronegative rheumatoid arthritis. Bosnian journal of basic medical sciences. 2011 Aug; [PubMed PMID: 21875421]
Level 2 (mid-level) evidenceRenner WR,Weinstein AS, Early changes of rheumatoid arthritis in the hand and wrist. Radiologic clinics of North America. 1988 Nov; [PubMed PMID: 3051092]
Narváez JA,Narváez J,De Lama E,De Albert M, MR imaging of early rheumatoid arthritis. Radiographics : a review publication of the Radiological Society of North America, Inc. 2010 Jan; [PubMed PMID: 20083591]
Arnett FC,Edworthy SM,Bloch DA,McShane DJ,Fries JF,Cooper NS,Healey LA,Kaplan SR,Liang MH,Luthra HS, The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis and rheumatism. 1988 Mar [PubMed PMID: 3358796]
Nelson PT,Saper CB, Ultrastructure of neurofibrillary tangles in the cerebral cortex of sheep. Neurobiology of aging. 1995 May-Jun [PubMed PMID: 7566341]
Level 3 (low-level) evidenceAletaha D,Neogi T,Silman AJ,Funovits J,Felson DT,Bingham CO 3rd,Birnbaum NS,Burmester GR,Bykerk VP,Cohen MD,Combe B,Costenbader KH,Dougados M,Emery P,Ferraccioli G,Hazes JM,Hobbs K,Huizinga TW,Kavanaugh A,Kay J,Kvien TK,Laing T,Mease P,Ménard HA,Moreland LW,Naden RL,Pincus T,Smolen JS,Stanislawska-Biernat E,Symmons D,Tak PP,Upchurch KS,Vencovský J,Wolfe F,Hawker G, 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis and rheumatism. 2010 Sep [PubMed PMID: 20872595]
Britsemmer K,Ursum J,Gerritsen M,van Tuyl LH,van Schaardenburg D, Validation of the 2010 ACR/EULAR classification criteria for rheumatoid arthritis: slight improvement over the 1987 ACR criteria. Annals of the rheumatic diseases. 2011 Aug [PubMed PMID: 21586440]
Level 1 (high-level) evidencevan der Linden MP,Knevel R,Huizinga TW,van der Helm-van Mil AH, Classification of rheumatoid arthritis: comparison of the 1987 American College of Rheumatology criteria and the 2010 American College of Rheumatology/European League Against Rheumatism criteria. Arthritis and rheumatism. 2011 Jan [PubMed PMID: 20967854]
Chauhan K,Jandu JS,Goyal A,Bansal P,Al-Dhahir MA, Rheumatoid Arthritis . 2020 Jan [PubMed PMID: 28723028]
Wolfe F,Rehman Q,Lane NE,Kremer J, Starting a disease modifying antirheumatic drug or a biologic agent in rheumatoid arthritis: standards of practice for RA treatment. The Journal of rheumatology. 2001 Jul [PubMed PMID: 11469485]
Korpela M,Laasonen L,Hannonen P,Kautiainen H,Leirisalo-Repo M,Hakala M,Paimela L,Blåfield H,Puolakka K,Möttönen T, Retardation of joint damage in patients with early rheumatoid arthritis by initial aggressive treatment with disease-modifying antirheumatic drugs: five-year experience from the FIN-RACo study. Arthritis and rheumatism. 2004 Jul [PubMed PMID: 15248204]
Level 1 (high-level) evidenceBoers M,Verhoeven AC,Markusse HM,van de Laar MA,Westhovens R,van Denderen JC,van Zeben D,Dijkmans BA,Peeters AJ,Jacobs P,van den Brink HR,Schouten HJ,van der Heijde DM,Boonen A,van der Linden S, Randomised comparison of combined step-down prednisolone, methotrexate and sulphasalazine with sulphasalazine alone in early rheumatoid arthritis. Lancet (London, England). 1997 Aug 2 [PubMed PMID: 9251634]
Level 1 (high-level) evidenceFurst DE, Meloxicam: selective COX-2 inhibition in clinical practice. Seminars in arthritis and rheumatism. 1997 Jun; [PubMed PMID: 9219316]
Level 3 (low-level) evidenceQuan L,Zhang Y,Crielaard BJ,Dusad A,Lele SM,Rijcken CJF,Metselaar JM,Kostková H,Etrych T,Ulbrich K,Kiessling F,Mikuls TR,Hennink WE,Storm G,Lammers T,Wang D, Nanomedicines for inflammatory arthritis: head-to-head comparison of glucocorticoid-containing polymers, micelles, and liposomes. ACS nano. 2014 Jan 28; [PubMed PMID: 24341611]
Level 3 (low-level) evidenceCombe B, Early rheumatoid arthritis: strategies for prevention and management. Best practice [PubMed PMID: 17350542]
Yasir M,Goyal A,Bansal P,Sonthalia S, Corticosteroid Adverse Effects . 2020 Jan [PubMed PMID: 30285357]
Deighton C,Criswell LA, Recent advances in the genetics of rheumatoid arthritis. Current rheumatology reports. 2006 Oct; [PubMed PMID: 16973114]
Level 3 (low-level) evidenceGregori D,Giacovelli G,Minto C,Barbetta B,Gualtieri F,Azzolina D,Vaghi P,Rovati LC, Association of Pharmacological Treatments With Long-term Pain Control in Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis. JAMA. 2018 Dec 25; [PubMed PMID: 30575881]
Level 1 (high-level) evidenceLyseng-Williamson KA, Anakinra in Still's disease: a profile of its use. Drugs [PubMed PMID: 30546251]
Abbasi M,Mousavi MJ,Jamalzehi S,Alimohammadi R,Bezvan MH,Mohammadi H,Aslani S, Strategies toward rheumatoid arthritis therapy; the old and the new. Journal of cellular physiology. 2019 Jul; [PubMed PMID: 30536757]
Hegde VS,Nagalli S, Leucovorin 2020 Jan; [PubMed PMID: 31971754]
Lian BS,Busmanis I,Lee HY, Relapsing Course of Sulfasalazine-Induced Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Complicated by Alopecia Universalis and Vitiligo. Annals of the Academy of Medicine, Singapore. 2018 Nov; [PubMed PMID: 30578426]
Benjamin O,Bansal P,Goyal A,Lappin SL, Disease Modifying Anti-Rheumatic Drugs (DMARD) . 2020 Jan [PubMed PMID: 29939640]
Gerriets V,Bansal P,Goyal A,Khaddour K, Tumor Necrosis Factor (TNF) Inhibitors . 2020 Jan [PubMed PMID: 29494032]
Aletaha D,Smolen JS, Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA. 2018 Oct 2; [PubMed PMID: 30285183]
Köhler BM,Günther J,Kaudewitz D,Lorenz HM, Current Therapeutic Options in the Treatment of Rheumatoid Arthritis. Journal of clinical medicine. 2019 Jun 28; [PubMed PMID: 31261785]
Breedveld FC,Dayer JM, Leflunomide: mode of action in the treatment of rheumatoid arthritis. Annals of the rheumatic diseases. 2000 Nov; [PubMed PMID: 11053058]
Fraenkel L,Bathon JM,England BR,St Clair EW,Arayssi T,Carandang K,Deane KD,Genovese M,Huston KK,Kerr G,Kremer J,Nakamura MC,Russell LA,Singh JA,Smith BJ,Sparks JA,Venkatachalam S,Weinblatt ME,Al-Gibbawi M,Baker JF,Barbour KE,Barton JL,Cappelli L,Chamseddine F,George M,Johnson SR,Kahale L,Karam BS,Khamis AM,Navarro-Millán I,Mirza R,Schwab P,Singh N,Turgunbaev M,Turner AS,Yaacoub S,Akl EA, 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis [PubMed PMID: 34101376]
Azeez M,Clancy C,O'Dwyer T,Lahiff C,Wilson F,Cunnane G, Benefits of exercise in patients with rheumatoid arthritis: a randomized controlled trial of a patient-specific exercise programme. Clinical rheumatology. 2020 Feb 8; [PubMed PMID: 32036584]
Level 1 (high-level) evidenceHernández-Hernández MV,Díaz-González F, Role of physical activity in the management and assessment of rheumatoid arthritis patients. Reumatologia clinica. 2017 Jul - Aug; [PubMed PMID: 27263964]
Dwivedi S,Testa EJ,Modest JM,Ibrahim Z,Gil JA, Surgical Management of Rheumatoid Arthritis of the Hand. Rhode Island medical journal (2013). 2020 May 1; [PubMed PMID: 32357591]
Senthelal S,Li J,Goyal A,Bansal P,Thomas MA, Arthritis . 2020 Jan [PubMed PMID: 30085534]
Bastian H,Ziegeler K,Hermann KGA,Feist E, [Rheumatoid arthritis-mimics : When appearances are deceptive]. Zeitschrift fur Rheumatologie. 2019 Feb; [PubMed PMID: 30191389]
Smolen JS,Landewé R,Breedveld FC,Buch M,Burmester G,Dougados M,Emery P,Gaujoux-Viala C,Gossec L,Nam J,Ramiro S,Winthrop K,de Wit M,Aletaha D,Betteridge N,Bijlsma JW,Boers M,Buttgereit F,Combe B,Cutolo M,Damjanov N,Hazes JM,Kouloumas M,Kvien TK,Mariette X,Pavelka K,van Riel PL,Rubbert-Roth A,Scholte-Voshaar M,Scott DL,Sokka-Isler T,Wong JB,van der Heijde D, EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Annals of the rheumatic diseases. 2014 Mar; [PubMed PMID: 24161836]
Kłodziński Ł,Wisłowska M, Comorbidities in rheumatic arthritis. Reumatologia. 2018; [PubMed PMID: 30237627]