Introduction
Nucleus pulposus herniation is the most common cause of sciatic pain and one of the most common indications for spine surgery worldwide.[1] This condition presents as a displacement of the nucleus pulposus beyond the intervertebral disc space.
The disc anatomy consists of two main structures, the nucleus pulposus (NP) and the annulus fibrosus (AF).
The nucleus pulposus is composed of water, type II collagen, chondrocyte-like cells, and proteoglycans. This unique composite allows the NP to be elastic, flexible under stress forces and to absorb compression.[2]
The composition of the AF is mainly concentric layers of collagen type I fibers,[3] forming a fibrous tissue with helical disposition surrounding the NP, this structure is denser in the anterior part and is attached to the vertebral body by Sharpey fibers.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Disc herniation and disc degeneration are associated terms, being nucleus pulposus herniation a possible evolution from a degenerative disc. Disc degeneration is usually associated with the loss of proteoglycans.[4] Multiple factors influence the degenerative process such as genetic, mechanical, and behavioral.[5][6]
The intervertebral disc is a structure that provides flexibility and transmits loads through the spine. Mechanical load is important in maintaining a healthy IVD by generating signals to cells that regulate proper matrix homeostasis.[7][8] On the other hand, prolonged exposure to hypo- or hyper-loading correlates with disc degeneration induction.[9][10]
Epidemiology
The estimated prevalence of disc herniation is approximately 1 to 3%. The highest observed incidence is between 30 to 50 years, and it is more frequent in men than in women (ratio 2 to 1).
Pathophysiology
Disc herniation is a consequence of degenerative changes in the annulus; those changes are age-related adaptive modifications in the disc structure that encompass desiccation, fissures, disc narrowing, mucinous degeneration, intradiscal gas (vacuum), osteophytes, inflammatory changes, and subchondral sclerosis. Annulus fissures predispose to a weakness, which allows disc material to bulge or migrate outside the annulus margins.
Histopathology
Nucleus pulposus herniation results from a failure in the annulus fibrosis integrity, making the content of the nucleus to protrude into the neural canal, the intervertebral foramen (foraminal) or lateral to the foramen (extraforaminal). Nucleus pulposus protrusion is the less severe scenario of disc herniation, due to partial rupture of the annulus fibrosis (See figure 1), when the annulus structure becomes completely disrupted the nucleus content may extrude outside the disc space and in some cases a fragment of nucleus pulposus may migrate (sequestration).
Another way to differentiate protrusion from extrusion is related to the shape of the displaced material. A protrusion is when the greatest distance between the limits of the disc material outside the disc space is less than the distance between the limits of the base of that disc material outside the disc space. The base is the width of disc material at the outer margin of the disc space. Extrusion is present when, in at least one plane, the distance between the limits of the disc material beyond the disc space exceeds the distance between the limits of the base of the disc material beyond the disc space.
Another type of disc herniation is when disc material migrates in craniocaudal direction through a gap between the endplate and the disc making a space within the vertebral body (intravertebral disc herniation) better know as Schmorl nodes.[11]
The integrity of the annulus fibrosus has to be compromised to develop a nucleus pulposus herniation. The loss of annulus fibrosus integrity may be present in different forms, such as radial, transverse, or concentric fissures. These types of fissures are observable in the early stages of disc degeneration. One important kind of annulus fissure can be observed in T2-weighted MRI and is called high-intensity zone (HIZ), this changes denote the presence of liquid within an annular fissure and correlates with acute disc annular tear or fissure.[12]
History and Physical
Proper understanding of anatomical zones and vertebral levels is essential to interpret the clinical manifestations secondary to a disc herniation. Wiltse proposed these anatomical zones, based on the following landmarks: medial border of the articular facet, lateral, upper and medial borders of the pedicles, coronal and sagittal planes at the center of the disc. On the axial plane, these landmarks determine the central zone, the subarticular zone (lateral recess), foraminal, and extraforaminal zones. On the sagittal plane, the levels are termed as follows: The supra pedicular level, the pedicular level, the infrapedicular level, and the disc level. The correct knowledge of anatomy and the relationship between nerve roots and disc herniation allows the proper understanding of common clinical findings associated with this problem.
There are two main mechanisms to explain radicular pain secondary to a nucleus pulposus herniation: Mechanical compression and inflammatory reaction. Clinical symptoms may vary according to several factors such as the location of the herniation (level), neural compression, and evolution. Nucleus pulposus herniation can produce low back pain; however, the primary clinical manifestation is a radiculopathy, which is mainly manifested by radiating pain and sensitive changes that encompass nerve distribution. Additionally, reflexes assessment (decreased reflex) may help to identify the compromised nerve root.
We summarize the anatomy, motor function, sensitive distribution, and reflex of the most commons nerve roots involved in cervical and lumbosacral nucleus pulposus herniation:
Cervical:
- C5 nerve root: Exits between C4 and C5 foramina, innervates deltoids and biceps (with C6), sensory distribution: lateral arm (axillary nerve) and is assessed with biceps reflex.
- C6 nerve root: Exits between C5 and C6 foramina, innervates biceps (with C5) and wrist extensors, sensory distribution: lateral forearm (musculocutaneous nerve), assessed with brachioradialis reflex.
- C7 nerve root: Exits between C6 and C7 foramina, innervates triceps, wrist flexors, and finger extensors, sensory distribution: middle finger, assessed with triceps reflex.
- C8 nerve root: Exits between C7 and T1 foramina, innervates interosseus muscles and finger flexors, sensory distribution: ring and little fingers and distal half of the forearm (ulnar side), no reflex.
Lumbosacral:
- L1 nerve root: Exits between L1 and L2 foramina, innervates iliopsoas muscle, sensory distribution: upper third thigh, assessed with the cremasteric reflex (male).
- L2 nerve root: Exits between L2 and L3 foramina, innervates iliopsoas muscle, hip adductor, and quadriceps, sensory distribution: middle third thigh, no reflex.
- L3 nerve root: Exits between L3 and L4 foramina, innervates iliopsoas muscle, hip adductor, and quadriceps, sensory distribution: lower third thigh, no reflex.
- L4 nerve root: Exits between L4 and L5 foramina, innervates quadriceps and tibialis anterior, sensory distribution: anterior knee, medial side of the leg, assessed with patellar reflex.
- L5 nerve root: Exits between L5 and S1 foramina, innervates extensor hallucis longus, extensor digitorum longus, and brevis, and gluteus medius, sensory distribution: anterior leg, lateral leg, and dorsum of the foot, no reflex.
- S1 nerve root: Exits between S1 and S2 foramina, innervates gastrocnemius, soleus, and gluteus maximus, sensitive distribution: posterior thigh, plantar region, assessed with Achilles reflex.
Cervical and thoracic disc herniation can also exhibit symptoms of myelopathy such as spasticity, clumsiness, wide-based gate, and weakness, on physical examination hyperreflexia is the most important sign. The Lhermitte sign is the presence of an electric shock-like sensation towards the back and lower extremities, especially by flexing the neck.[13][14] Bowel and bladder dysfunction may indicate poor prognosis.
Evaluation
In the presence of low back pain without symptoms of radiculopathy, there is no need to request studies as most of the patients improve in a couple of weeks, a 4-week follow-up is a usual timeframe.[15]
X-ray is the initial workup study when there is a strong suspicion of a specific cause of cervical or back pain (fracture, infection, tumor) or in the presence of red flags (fever, age more than 50, recent trauma, pain at night or rest, unexplained weight loss, progressive motor or sensory deficit, saddle anesthesia, history of cancer or osteoporosis, failure to improve after six weeks of conservative treatment). Anteroposterior and lateral x-ray is helpful to assess fracture, bony deformity, decreased intervertebral height, osteophytes, spondylolisthesis, and facet joint osteoarthritis.
MRI is the recommended diagnostic imaging in cases of severe or progressive neurologic deficits, suspicion of an underlying condition such as infection, fracture, cauda equina syndrome, spinal cord compression. In cases of radiculopathy, most of the cases improve with conservative treatment and MRI is indicated in those cases with significant pain or neurologic deficits.[16]
CT myelogram is the imaging option in patients with contraindications to MRI.
CT scan is not usually requested in nucleus pulposus herniation. However, it can be helpful in some cases when there is a suspicion of calcified disc herniation (thoracic disc herniation has a 30 to 70% rate of calcification) which is more challenging especially when surgery is a consideration.
Treatment / Management
Therapeutic management of nucleus pulposus herniation encompasses conservative and surgical treatment. Conservative treatment is the main strategy due to the natural history of nucleus pulposus herniation, with good response to pain treatment or nerve root steroid injection as well as some cases of spontaneous regression.[17][18](A1)
Some patients will not benefit from conservative treatment and will require surgery to decompress the nerve involved. Classical surgical indications are motor deficit, cauda equina syndrome, and persistent pain after conservative treatment.
In cervical disc herniation, there is no evidence of effectiveness for conservative treatment compared with surgery [Level I].[19] Different randomized controlled trials (RTC) have compared conservative versus surgical treatment in lumbar disc herniation, observing faster pain relief and recovery in the early surgery groups, however, similar outcomes in the long term (one or two years) were found.[20][21] In another trial, carefully selected patients who underwent surgery for lumbar disc herniation achieved greater improvement compared to nonoperative treated patients at eight years follow up [Level II].[22](A1)
Differential Diagnosis
Nucleus pulposus herniation is the most common cause of radicular pain in the lumbar spine and the second most common cause in the cervical spine after degenerative spondylosis; however, other conditions in the differential diagnosis should be considered such as:
- Conjoined nerve root
- Facet joint cyst
- Facet joint/ligamentum flavum hypertrophy
- Neurinoma/schwannoma
- Spondylolisthesis
Prognosis
The majority of patients suffering from nucleus pulposus herniation experience symptoms resolution without surgery.[23] Conservative treatment is effective, and patients usually experience symptom relief after a couple of weeks. However, some cases do not improve with conservative treatment and may require more invasive therapies such as nerve root steroid injection or even surgery.
The presence of myelopathy in cases of central nucleus pulposus herniation in the cervical or thoracic region is an indication for surgery, especially in the setting of symptoms progression.
Complications
Complications associated with nucleus pulposus herniation can result from the compression effect on the nerve root in severe cases resulting in motor deficit, in the cervical and thoracic spine there is also a risk of spinal cord compression in severe cases. These complications are relatively uncommon but should be considered and properly treated to avoid a permanent neurological deficit.
Cauda equina syndrome is another complication that results from lumbosacral nerve roots compression with possible bowel or bladder dysfunction. It is a rarely occurring condition (less than 1%). However, it is considered an absolute indication for acute surgical resolution, and early decompression is associated with symptoms improvement.[24]
Deterrence and Patient Education
It is crucial for patients to recognize radicular pain because it can be the result of a nucleus pulposus herniation in the cervical or lumbar spine. It is essential to have a consult after a persistent radiating pain and be examined by a primary care provider. Most of the symptoms usually improve with conservative treatment; only a few cases with severe pain or neurologic deficit may need additional imaging studies and further specialist referral.
Enhancing Healthcare Team Outcomes
Nucleus pulposus herniation is a common complaint among young adults; clinical symptoms such as low back or cervical pain with radicular pain (brachialgia or sciatica) may raise suspicion of a possible nerve root inflammation/compression and further referral to a specialist. In cervical disc herniation, there is no evidence of effectiveness for conservative treatment compared with surgery [Level I], on the other hand, carefully selected patients who underwent surgery for lumbar disc herniation achieved more significant improvement compared to nonoperative treated patients [Level II]. A coordinated effort between the primary care provider, specialty-trained nurses, spine specialists, physical therapists and chiropractors (who may be the patient's first point of contact), communicating across professions, and providing patient and family education is vital to guide proper management in patients with symptomatic nucleus pulposus herniation [Level V].
Media
(Click Image to Enlarge)
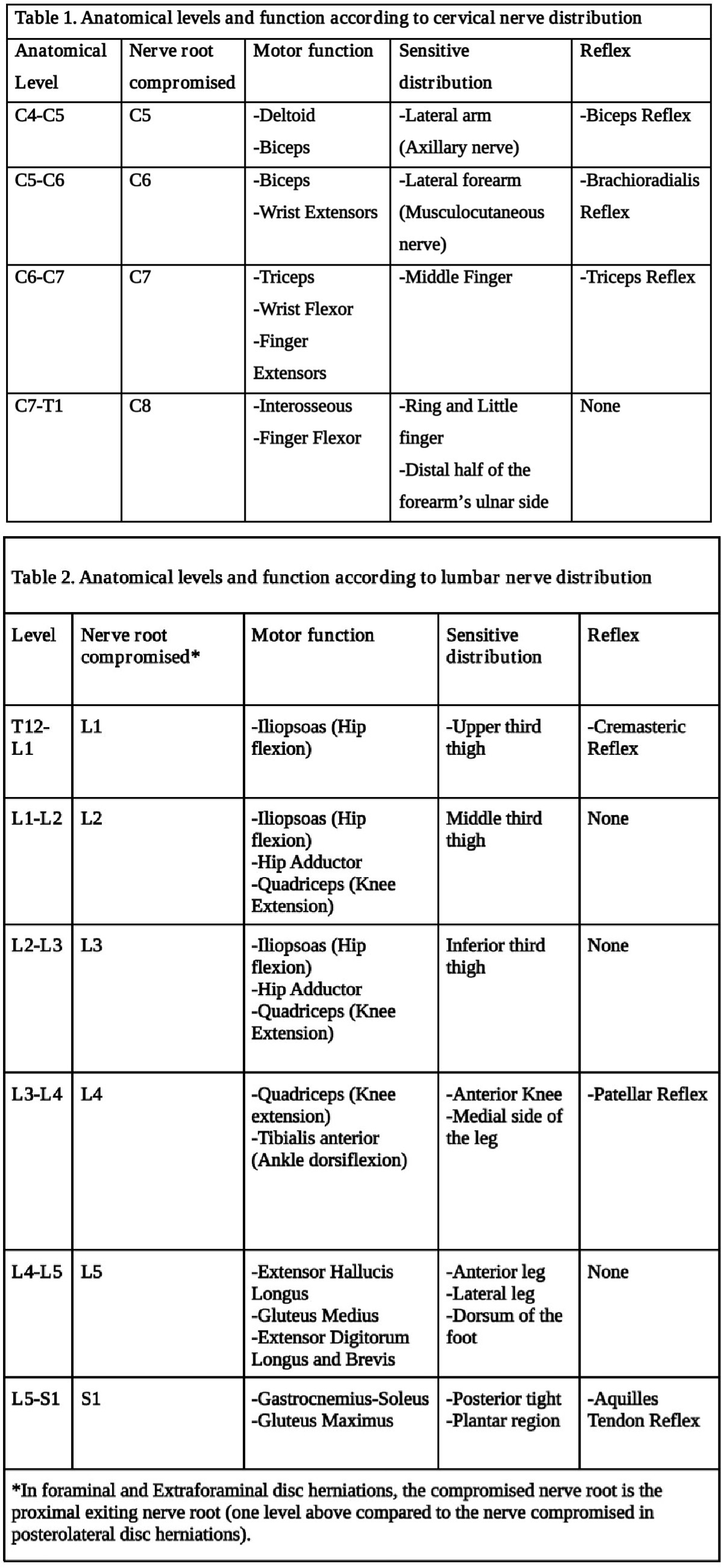
Tables one and two of Nucleus pulposus herniation Contributed by Gaston Camino Willhuber, MD
(Click Image to Enlarge)
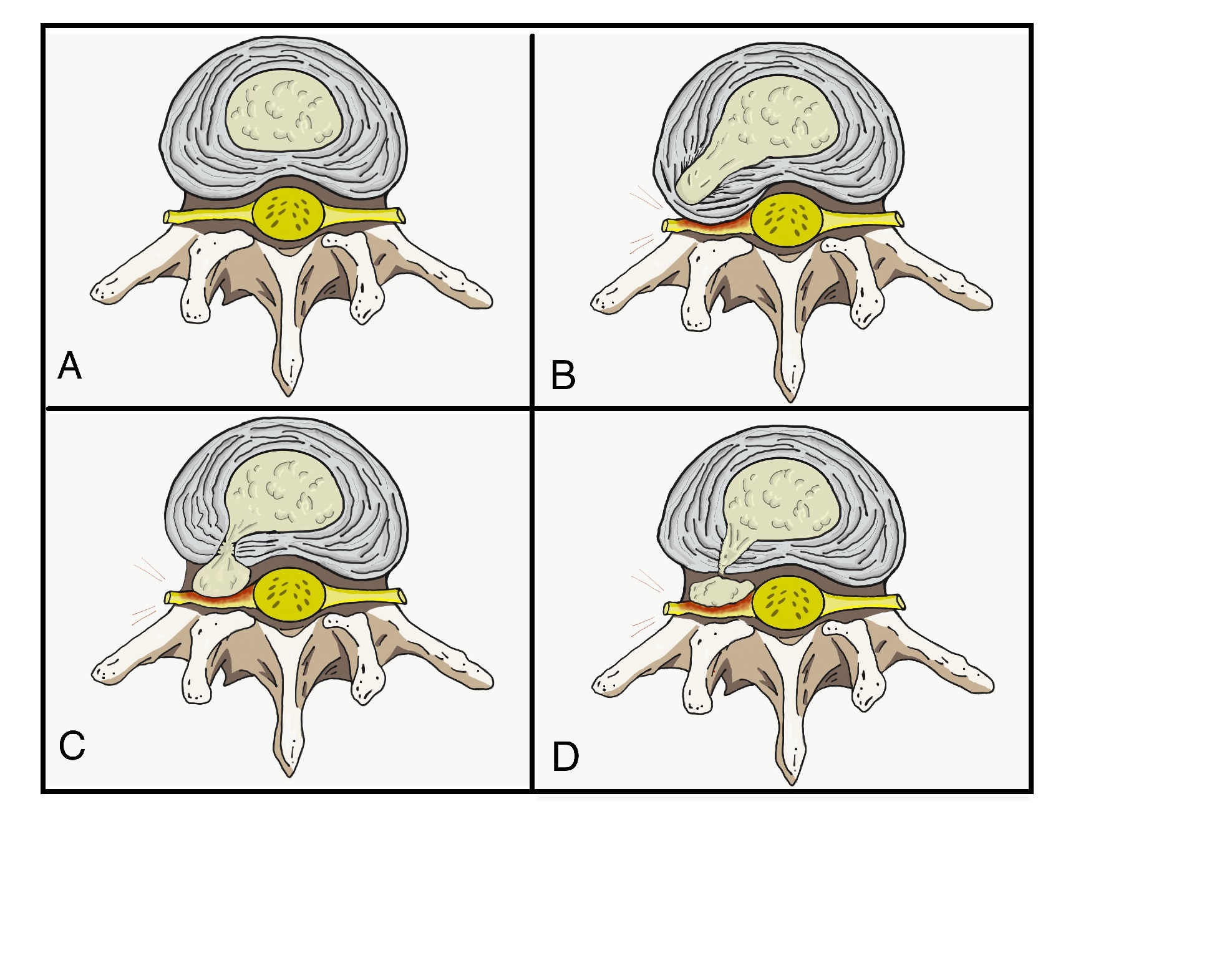
Figure 1. A) Normal disc anatomy B) Disc Protrusion C) Disc Extrusion D) Disc Sequestration Contributed by Franco De Cicco MD
References
Martin BI, Mirza SK, Comstock BA, Gray DT, Kreuter W, Deyo RA. Reoperation rates following lumbar spine surgery and the influence of spinal fusion procedures. Spine. 2007 Feb 1:32(3):382-7 [PubMed PMID: 17268274]
Level 2 (mid-level) evidenceChen S, Fu P, Wu H, Pei M. Meniscus, articular cartilage and nucleus pulposus: a comparative review of cartilage-like tissues in anatomy, development and function. Cell and tissue research. 2017 Oct:370(1):53-70. doi: 10.1007/s00441-017-2613-0. Epub 2017 Apr 17 [PubMed PMID: 28413859]
Level 2 (mid-level) evidenceHe Y, Qiu Y, Zhu F, Zhu Z. Quantitative analysis of types I and II collagen in the disc annulus in adolescent idiopathic scoliosis. Studies in health technology and informatics. 2006:123():123-8 [PubMed PMID: 17108414]
Level 2 (mid-level) evidenceRoughley PJ, Alini M, Antoniou J. The role of proteoglycans in aging, degeneration and repair of the intervertebral disc. Biochemical Society transactions. 2002 Nov:30(Pt 6):869-74 [PubMed PMID: 12440935]
Level 3 (low-level) evidenceHadjipavlou AG, Tzermiadianos MN, Bogduk N, Zindrick MR. The pathophysiology of disc degeneration: a critical review. The Journal of bone and joint surgery. British volume. 2008 Oct:90(10):1261-70. doi: 10.1302/0301-620X.90B10.20910. Epub [PubMed PMID: 18827232]
Battié MC, Videman T, Kaprio J, Gibbons LE, Gill K, Manninen H, Saarela J, Peltonen L. The Twin Spine Study: contributions to a changing view of disc degeneration. The spine journal : official journal of the North American Spine Society. 2009 Jan-Feb:9(1):47-59. doi: 10.1016/j.spinee.2008.11.011. Epub [PubMed PMID: 19111259]
MacLean JJ, Lee CR, Alini M, Iatridis JC. The effects of short-term load duration on anabolic and catabolic gene expression in the rat tail intervertebral disc. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2005 Sep:23(5):1120-7 [PubMed PMID: 16140193]
Level 3 (low-level) evidenceMacLean JJ, Lee CR, Grad S, Ito K, Alini M, Iatridis JC. Effects of immobilization and dynamic compression on intervertebral disc cell gene expression in vivo. Spine. 2003 May 15:28(10):973-81 [PubMed PMID: 12768134]
Level 3 (low-level) evidenceLotz JC, Chin JR. Intervertebral disc cell death is dependent on the magnitude and duration of spinal loading. Spine. 2000 Jun 15:25(12):1477-83 [PubMed PMID: 10851095]
Level 3 (low-level) evidenceLotz JC, Colliou OK, Chin JR, Duncan NA, Liebenberg E. Compression-induced degeneration of the intervertebral disc: an in vivo mouse model and finite-element study. Spine. 1998 Dec 1:23(23):2493-506 [PubMed PMID: 9854748]
Level 3 (low-level) evidenceTakahashi K, Miyazaki T, Ohnari H, Takino T, Tomita K. Schmorl's nodes and low-back pain. Analysis of magnetic resonance imaging findings in symptomatic and asymptomatic individuals. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 1995:4(1):56-9 [PubMed PMID: 7749909]
Jha SC, Takata Y, Abe M, Yamashita K, Tezuka F, Sakai T, Higashino K, Nagamachi A, Sairyo K. High intensity zone in lumbar spine and its correlation with disc degeneration. The journal of medical investigation : JMI. 2017:64(1.2):39-42. doi: 10.2152/jmi.64.39. Epub [PubMed PMID: 28373626]
Siivola SM, Levoska S, Tervonen O, Ilkko E, Vanharanta H, Keinänen-Kiukaanniemi S. MRI changes of cervical spine in asymptomatic and symptomatic young adults. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2002 Aug:11(4):358-63 [PubMed PMID: 12193998]
Uribe JS, Smith WD, Pimenta L, Härtl R, Dakwar E, Modhia UM, Pollock GA, Nagineni V, Smith R, Christian G, Oliveira L, Marchi L, Deviren V. Minimally invasive lateral approach for symptomatic thoracic disc herniation: initial multicenter clinical experience. Journal of neurosurgery. Spine. 2012 Mar:16(3):264-79. doi: 10.3171/2011.10.SPINE11291. Epub 2011 Dec 16 [PubMed PMID: 22176427]
Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr, Shekelle P, Owens DK, Clinical Efficacy Assessment Subcommittee of the American College of Physicians, American College of Physicians, American Pain Society Low Back Pain Guidelines Panel. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Annals of internal medicine. 2007 Oct 2:147(7):478-91 [PubMed PMID: 17909209]
Level 3 (low-level) evidenceLateef H, Patel D. What is the role of imaging in acute low back pain? Current reviews in musculoskeletal medicine. 2009 Jun:2(2):69-73. doi: 10.1007/s12178-008-9037-0. Epub 2009 Apr 28 [PubMed PMID: 19468875]
Sayegh FE, Kenanidis EI, Papavasiliou KA, Potoupnis ME, Kirkos JM, Kapetanos GA. Efficacy of steroid and nonsteroid caudal epidural injections for low back pain and sciatica: a prospective, randomized, double-blind clinical trial. Spine. 2009 Jun 15:34(14):1441-7. doi: 10.1097/BRS.0b013e3181a4804a. Epub [PubMed PMID: 19525834]
Level 1 (high-level) evidenceTurk O, Antar V, Yaldiz C. Spontaneous regression of herniated nucleus pulposus: The clinical findings of 76 patients. Medicine. 2019 Feb:98(8):e14667. doi: 10.1097/MD.0000000000014667. Epub [PubMed PMID: 30813213]
Gebremariam L, Koes BW, Peul WC, Huisstede BM. Evaluation of treatment effectiveness for the herniated cervical disc: a systematic review. Spine. 2012 Jan 15:37(2):E109-18. doi: 10.1097/BRS.0b013e318221b5af. Epub [PubMed PMID: 21587105]
Level 1 (high-level) evidencePeul WC, van Houwelingen HC, van den Hout WB, Brand R, Eekhof JA, Tans JT, Thomeer RT, Koes BW, Leiden-The Hague Spine Intervention Prognostic Study Group. Surgery versus prolonged conservative treatment for sciatica. The New England journal of medicine. 2007 May 31:356(22):2245-56 [PubMed PMID: 17538084]
Level 1 (high-level) evidenceJacobs WC, van Tulder M, Arts M, Rubinstein SM, van Middelkoop M, Ostelo R, Verhagen A, Koes B, Peul WC. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2011 Apr:20(4):513-22. doi: 10.1007/s00586-010-1603-7. Epub 2010 Oct 15 [PubMed PMID: 20949289]
Level 1 (high-level) evidenceLurie JD, Tosteson TD, Tosteson AN, Zhao W, Morgan TS, Abdu WA, Herkowitz H, Weinstein JN. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial. Spine. 2014 Jan 1:39(1):3-16. doi: 10.1097/BRS.0000000000000088. Epub [PubMed PMID: 24153171]
Level 1 (high-level) evidenceBenoist M. The natural history of lumbar disc herniation and radiculopathy. Joint bone spine. 2002 Mar:69(2):155-60 [PubMed PMID: 12027305]
Srikandarajah N, Boissaud-Cooke MA, Clark S, Wilby MJ. Does early surgical decompression in cauda equina syndrome improve bladder outcome? Spine. 2015 Apr 15:40(8):580-3. doi: 10.1097/BRS.0000000000000813. Epub [PubMed PMID: 25646751]
Level 2 (mid-level) evidence