Introduction
Herpangina is a viral infection that is manifested clinically as an acute febrile illness with small ulcerative or vesicular lesions in the posterior oropharynx. Though primarily a pediatric disease, multiple cases in newborns, adolescents, and young adults have also been reported. The disease is highly contagious, and most cases are reported in the summer months. The disease is caused by 22 enterovirus serotypes and is most commonly associated with the Coxsackie B virus serotype. It can occur in association with an enteroviral exanthem and several neurological conditions, including, but not limited to, aseptic meningitis, acute flaccid paralysis, and encephalitis.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Herpangina was first recognized in the 1920s, but the exact etiology was not described until almost 30 years later.[1] The febrile enanthem of herpangina is caused by multiple enteroviruses, but the most commonly implicated etiological agents include the coxsackie B virus, coxsackie A16 virus, enterovirus 71 virus serotypes. Other agents mentioned by various sources include echovirus, adenovirus, parechovirus, and herpes simplex virus. Enteroviruses are small, non-enveloped, single positive-strand RNA viruses. They are capable of surviving in a wide pH range and retain infectivity in temperatures up to 50 C. These characteristics make them capable of surviving in the environment for relatively extended periods. Humans are the only natural host of these viruses.[2][3]
Epidemiology
Herpangina most frequently occurs in the pediatric population in patients younger than 10 years of age. Children are often infected via exposure at childcare centers or schools. Adolescents and adults are less frequently affected. Newborns, immunocompromised, and pregnant patients can develop more severe disease. Neither gender is more commonly infected. In the United States, most infections occur during the summer and fall months in temperate climates but may occur all year round in tropical climates. Cases of herpangina have been reported worldwide, and the most recent fatal outbreak was reported in Japan in 2007.[4] In tropical climates, these diseases usually occur during the rainy seasons.[5]
Pathophysiology
The genus Enterovirus belongs to the Picornaviridae family. Enteroviruses are typically spread via the fecal-oral route. Transmission can additionally result from the ingestion of infected saliva, respiratory droplets, or direct contact with fluid from vesicles. The incubation period ranges from 3 to 5 days. Viral shedding can occur even in asymptomatic patients. Respiratory viral shedding can persist for up to 3 weeks and in the stool for up to 8 weeks. Patients are most contagious in the first 1 to 2 weeks of infection.[6] Of all the enteroviruses involved in causing herpangina, enterovirus 71 is emerging as an important public health concern causing severe illness, encephalitis, encephalomyelitis, and potentially death in newborns and young children.[7]
History and Physical
History
A complete and thorough history and physical examination are necessary to make the diagnosis and to exclude various other childhood disorders that have a similar presentation. Most symptomatic patients report malaise and high-grade fever, which may be high enough to provoke febrile seizures. Young children usually exhibit fussiness, poor feeding, and anorexia. Older children may report back pain and headache. Most patients also develop sore throats a day before the onset of the enanthem. Some patients may also develop anorexia, dehydration, and abdominal pain. An exanthem is also frequently reported by patients with herpangina, but the specific characteristics and rates of occurrence vary depending on the subtype of enterovirus causing the infection. Depending on the severity and organ system involvement, the patients may also report headaches, neck stiffness, confusion, seizures, muscle weakness, and difficulty breathing.
Physical Examination
Herpangina is associated with a painful enanthem that typically occurs on the soft palate, tonsils, and posterior pharynx. It is usually characterized by hyperemia of the pharynx with discrete erythematous macules that evolve into vesicles and eventually ulcerate centrally. The lesions are usually smaller than 5 mm and may occasionally appear on the buccal wall and posterior tongue. They persist for up to one week. Other physical examination findings include pharyngitis and cervical lymphadenopathy.[8]
A variant of herpangina caused by the Coxsackie A10 virus serotype is the acute lymphonodular pharyngitis. This condition is characterized by nodular lesions in the same location and distribution as the lesions of herpangina but does not undergo vesiculation or ulceration.[9] A subset of patients may develop a rash on the body with lesions that may be macular, maculopapular, vesicular, papulovesicular, papulopustular, morbilliform, or petechial. The rates of occurrence of the rash and specific characteristics vary, depending on the virus subtype responsible. Neurological physical examination findings, such as neck stiffness or paralysis, may be present if the patient has developed complications such as meningitis, acute flaccid paralysis, encephalitis, or encephalomyelitis. Dehydration is a common complication of herpangina, and signs such as dry mouth and decreased skin turgor may be seen.
The history and physical examination should also focus on ruling out other serious and potentially life-threatening febrile exanthems, including Kawasaki disease, Rocky Mountain spotted fever, eczema herpeticum, and toxic shock syndrome that have a similar presentation.
Evaluation
The diagnosis of herpangina is usually made clinically. In mild cases, no imaging or laboratory testing is required. Laboratory studies are usually obtained to gain additional information about complications such as dehydration or to rule out alternative diagnoses. The white blood cell count is usually within normal limits, though lymphocytosis may be seen in some situations. Confirmatory testing is usually required only in complicated disease, for the collection of epidemiological data during epidemics, or to differentiate herpangina from more serious diseases such as eczema herpeticum. Isolation of the enterovirus in cell culture is the “gold standard” for confirmatory testing, which can often take longer than a week to obtain results. This makes it an impractical test for clinical practice. Polymerase chain reaction (PCR) testing is fast and highly sensitive for enteroviruses. Samples may be obtained from the stool, mucocutaneous ulcers, vesicular fluid, or cerebrospinal fluid. Enzyme-linked immunosorbent assays (ELISA) testing is also available. ELISA testing for enteroviruses is generally less sensitive than PCR and should be utilized only in cases where PCR is not available. Serum antibodies to coxsackievirus may also be measured after clinical symptoms have developed. The antibody titer may show a four-fold rise in serial samples conducted two to three weeks apart.
Treatment / Management
Herpangina is a self-limited illness, and the treatment is primarily supportive. The management can be described as general treatment, symptomatic treatment, and antiviral treatment.
General
Patients should be isolated in well-aerated and clean rooms to prevent cross-infection. The general management includes a healthy diet and adequate hydration. The patient’s diet should be comprised of light, liquid, or semi-liquid foods with adequate calories and should avoid hot, spicy, and/or irritating foods. Emphasis should be placed on oral care, and it is recommended that patients rinse their mouths with normal saline after meals. Younger children can have their mouths wiped with normal saline. If normal saline is unavailable, salted water can be considered.[10] Oral hydration is very important, and for children with high-grade fever and feeding difficulty, proper rehydration with electrolyte solutions is recommended. The patients should be monitored closely while on treatment.(B3)
Symptomatic
High-grade fever is the most common symptom reported for herpangina. For patients whose temperature exceeds greater than 101.3 F (38.5 C), antipyretics such as ibuprofen or acetaminophen can be considered. The dosage, timing, and duration depend on the patient’s age and symptoms and are administered according to the treating physician’s recommendation. Several physical cooling options can be considered, including cool compresses of the forehead, fever cooling patches, or sleeping with an ice pack under the head. Adequate hydration should be ensured while treating with these drugs. Topical therapies containing lidocaine or diphenhydramine are not generally recommended for symptomatic treatment of the oral lesions in herpangina. This is due to the risks of toxicity associated with these medications and the lack of adequate trials.[11] Younger children with high-grade fever may develop febrile seizures during the disease, which should be controlled and treated immediately. Some sources recommend using intravenous midazolam (0.1-0.3 mg/kg/dose).[10](B2)
Antiviral
No specific antiviral drugs are currently available for the treatment of herpangina. Interferon-alpha spray, however, has shown some promising effects. Local administration of the drug can potentially have some local immunomodulatory and antiviral effects, as interferon-alpha plays a key role in maintaining anti-infection immunity for the mucosa.[12] In addition, the topical use of the spray has the benefits of being convenient, safe and makes it easier to maintain good drug compliance in children. Broad-spectrum antiviral drugs, such as acyclovir and gancyclovir, play no role in the treatment of herpangina as they are anti-DNA viral drugs, and the causative agents of herpangina are RNA viruses. Ribavirin is not recommended either for the routine treatment of herpangina, though it may have some role in the early stages of the disease.[10](B3)
Differential Diagnosis
Herpangina has a clinical presentation similar to several childhood disorders. Table 1 gives a summary of the differences in the clinical presentations of these disorders. Other diseases and conditions that should be ruled out before making the diagnosis include:
- Eczema herpeticum
- Toxic shock syndrome
- Measles
- Varicella
- Kawasaki disease
- Insect bites
- Rocky Mountain spotted fever
- Drug eruption
- Erythema multiforme major
Prognosis
Herpangina is generally a mild and self-limited disease. If appropriate care measures, patient isolation, adequate food intake, and hydration are maintained, the disease resolves in less than ten days. Symptomatic treatment for the patient’s fever and oral lesions and close observation for the development of febrile seizures in young children with high-grade fever also improve the prognosis of the disease. Patients who develop serious neurological complications have a variable course, and the prognosis is poor in certain situations. Thus patients should be monitored closely for the development of complications, including flaccid paralysis, meningitis/encephalitis, and myocarditis.
Complications
Herpangina itself is generally a mild condition, but some causative microorganisms, such as enterovirus 71, may result in severe complications, including the following:
- Brain stem encephalitis
- Acute flaccid paralysis
- Aseptic meningitis
- Myocarditis
Such patients are generally deemed critical and necessitate hospitalization. ICU care is advised in some cases.
Deterrence and Patient Education
The patients and their families should be informed about the self-limited nature of the disease. As herpangina is primarily a pediatric disease and can be a source of significant stress for the family members, the families need to be reassured. The families should be educated about the contagion of the disease and that the patient should be isolated in a well-aerated room until the symptoms improve. Emphasis should be placed on adequate diet and hydration and close monitoring of symptoms. Close attention should be paid to hand hygiene, and frequent handwashing should be recommended. The importance of handwashing should also be explained to family members in close contact with the patient during care, especially after activities such as changing diapers or feeding the child. The sanitization of surfaces and objects the patient is in contact with is also recommended. Though home treatment is generally preferred, the caretakers should be informed to stay in regular contact with the treating physician and should observe the patient closely for any change in symptoms. Out-patient follow-up care is generally not needed as the disease is short-lived.
Enhancing Healthcare Team Outcomes
Herpangina is a viral infection that is generally self-limited but may lead to serious complications. The diagnosis is primarily clinical, and specific diagnostic investigations are ordered in unclear presentations. Health-care providers must be well-versed with the range of clinical presentations seen in herpangina and should be able to differentiate it from other pediatric disorders with a similar presentation. They need to educate the family regarding the disease, the home-management, and prevention. An interprofessional approach with effective communication between the members of the healthcare team, including internists, pediatricians, nurses, and pharmacists, is essential for effective patient care and improved outcomes. [Level 5]
Media
(Click Image to Enlarge)
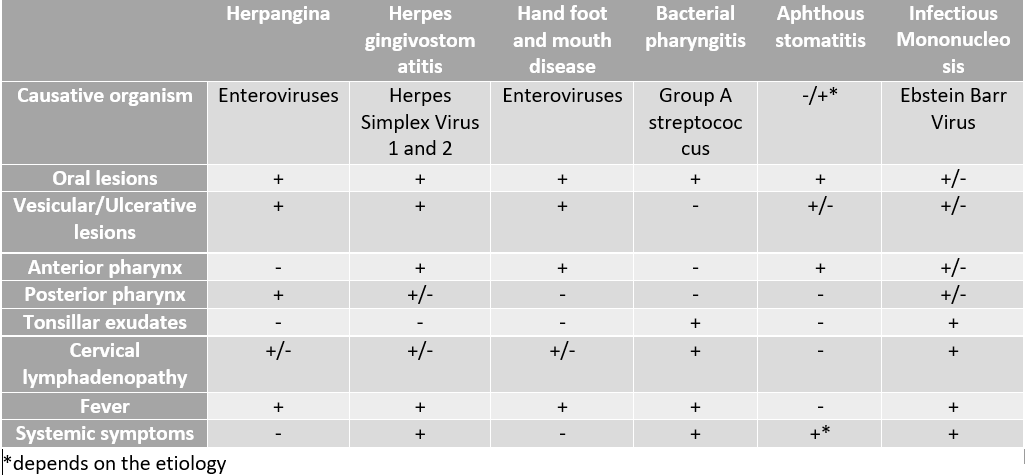
Differential diagnosis of pediatric oral lesions Contributed by Rimsha Ali, MD
References
HUEBNER RJ, COLE RM, BEEMAN EA, BELL JA, PEERS JH. Herpangina; etiological studies of a specific infectious disease. Journal of the American Medical Association. 1951 Mar 3:145(9):628-33 [PubMed PMID: 14794498]
B'Krong NTTC, Minh NNQ, Qui PT, Chau TTH, Nghia HDT, Do LAH, Nhung NN, Van Vinh Chau N, Thwaites G, Van Tan L, van Doorn HR, Thanh TT. Enterovirus serotypes in patients with central nervous system and respiratory infections in Viet Nam 1997-2010. Virology journal. 2018 Apr 12:15(1):69. doi: 10.1186/s12985-018-0980-0. Epub 2018 Apr 12 [PubMed PMID: 29650033]
Abedi GR, Watson JT, Pham H, Nix WA, Oberste MS, Gerber SI. Enterovirus and Human Parechovirus Surveillance - United States, 2009-2013. MMWR. Morbidity and mortality weekly report. 2015 Sep 4:64(34):940-3. doi: 10.15585/mmwr.mm6434a3. Epub 2015 Sep 4 [PubMed PMID: 26334674]
Sano T,Saito T,Kondo M,Watanabe S,Onoue Y,Konnai M,Sato Y,Orihara N, Enterovirus detection status of patients with herpangina and hand, foot and mouth disease in epidemic season 2007, Kanagawa Prefecture, Japan. Japanese journal of infectious diseases. 2008 Mar [PubMed PMID: 18362414]
Level 3 (low-level) evidenceYao X, Bian LL, Lu WW, Li JX, Mao QY, Wang YP, Gao F, Wu X, Ye Q, Li XL, Zhu FC, Liang Z. Epidemiological and etiological characteristics of herpangina and hand foot mouth diseases in Jiangsu, China, 2013-2014. Human vaccines & immunotherapeutics. 2017 Apr 3:13(4):823-830. doi: 10.1080/21645515.2016.1236879. Epub 2016 Oct 21 [PubMed PMID: 27768527]
Level 2 (mid-level) evidenceRepass GL, Palmer WC, Stancampiano FF. Hand, foot, and mouth disease: identifying and managing an acute viral syndrome. Cleveland Clinic journal of medicine. 2014 Sep:81(9):537-43. doi: 10.3949/ccjm.81a.13132. Epub [PubMed PMID: 25183845]
Choi CS, Choi YJ, Choi UY, Han JW, Jeong DC, Kim HH, Kim JH, Kang JH. Clinical manifestations of CNS infections caused by enterovirus type 71. Korean journal of pediatrics. 2011 Jan:54(1):11-6. doi: 10.3345/kjp.2011.54.1.11. Epub 2011 Jan 31 [PubMed PMID: 21359055]
Takeuchi Y. [Herpangina]. Nihon rinsho. Japanese journal of clinical medicine. 2007 Mar 28:65 Suppl 3():355-8 [PubMed PMID: 17491405]
STEIGMAN AJ, LIPTON MM, BRASPENNICKX H. Acute lymphonodular pharyngitis: a newly described condition due to Coxsackie A virus. The Journal of pediatrics. 1962 Sep:61():331-6 [PubMed PMID: 13916595]
Yu H, Li XW, Liu QB, Deng HL, Liu G, Jiang RM, Deng JK, Ye YZ, Hao JH, Chen YH, Nong GM, Shen ZB, Liu CS, Zou YX, Wu JZ, Wu XD, Chen BQ, Luo RP, Lin AW, Chen Y, Liu XD. Diagnosis and treatment of herpangina: Chinese expert consensus. World journal of pediatrics : WJP. 2020 Apr:16(2):129-134. doi: 10.1007/s12519-019-00277-9. Epub 2019 Jul 25 [PubMed PMID: 31347021]
Level 3 (low-level) evidenceYan X, Zhang ZZ, Yang ZH, Zhu CM, Hu YG, Liu QB. Clinical and Etiological Characteristics of Atypical Hand-Foot-and-Mouth Disease in Children from Chongqing, China: A Retrospective Study. BioMed research international. 2015:2015():802046. doi: 10.1155/2015/802046. Epub 2015 Nov 26 [PubMed PMID: 26693489]
Level 2 (mid-level) evidenceMangan NE, Fung KY. Type I interferons in regulation of mucosal immunity. Immunology and cell biology. 2012 May:90(5):510-9. doi: 10.1038/icb.2012.13. Epub 2012 Mar 20 [PubMed PMID: 22430250]
Level 3 (low-level) evidence