Introduction
Herpetic gingivostomatitis is a manifestation of herpes simplex virus type 1 (HSV-1) and is characterized by high-grade fever and painful oral lesions. While herpetic gingivostomatitis most commonly occurs in children from ages 6 months to 5 years, it may also occur in adults.[1] HSV-1 is usually spread from direct contact or via droplets of oral secretions or lesions from an asymptomatic or symptomatic individual. Once a patient is infected with the herpes simplex virus, the infection can recur in the form of herpes labialis (cold sores) with intermittent re-activation occurring throughout life.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The causative agent is Herpes simplex virus type 1 (HSV-1), which belongs to the alphaherpesvirus group. The virus is enveloped and has a linear double-stranded DNA genome. HSV-1 is mostly responsible for oral, ocular, and facial infections as it has a tropism for oral epithelium. While most cases of herpetic gingivostomatitis are associated with HSV-1 infection, some adult cases have been reported where HSV-2 was isolated from the oral lesions. Oral infection with HSV-2 is probably transmitted through orogenital contact and has also been observed in HIV-positive patients and patients undergoing immunosuppressive therapy.[3]
Epidemiology
Primary herpetic gingivostomatitis typically occurs in children younger than the age of 5 years, but can also occur in adolescents and adults. HSV-1 is usually acquired in childhood by coming into contact with oral secretions. It is estimated that almost 90% of the world’s population is seropositive for HSV-1 by 35 years of age, and half of the individuals carrying the virus will experience reactivation in the form of herpes labialis. Herpetic gingivostomatitis is equally distributed amongst gender and race groups and is not found to have a particular seasonal or geographic distribution.[4][5]
Pathophysiology
Both HSV-1 and HSV-2 have three major biological properties that play an important role in disease pathogenesis. These include neurovirulence, latency, and reactivation. Neurovirulence is the ability to invade and replicate in the nervous system, and latency is the ability to maintain the latent infection in the nerve cell. Reactivation is the ability to replicate and cause the disease process again, once induced by specific stimuli. HSV-1 causes herpes gingivostomatitis and eventually herpes labialis using the same biological properties. The pathogenesis of herpes gingivostomatitis involves the replication of the herpes simplex virus, cell lysis, and eventual destruction of mucosal tissue. Exposure to HSV-1 of the abraded surfaces allows the virus to enter and rapidly replicate in epidermal and dermal cells. This results in the clinical manifestation of perioral blisters, erosions of the lips and mucosa, and eventual hemorrhagic crusting. Sufficient viral inoculation and replication allow the virus to enter sensory and autonomic ganglia, where it travels intra-axonally to the ganglionic nerve bodies. HSV-1 most commonly infects the trigeminal ganglia, where the virus remains latent until reactivation, most commonly in the form of herpes labialis.[2]
Histopathology
Histological appearance of a mucosal herpetic infection includes degeneration of stratified squamous epithelial cells, acantholysis, and formation of an inflammatory infiltrate around the capillaries of the dermis. The characteristic intranuclear inclusion bodies known as Cowdry type A are found on light microscopy showing arrays of viral capsids and electron-dense glycoproteins.[6] Cowdry type A bodies are eosinophilic inclusion bodies that are also found in varicella-zoster, making the histologic lesions of herpetic gingivostomatitis and varicella indistinguishable. Direct immunohistochemistry using fluorescent antibodies can be used to further distinguish between the herpes virus and the varicella virus.[7]
History and Physical
Primary herpes gingivostomatitis usually occurs in children who have not been previously exposed to the virus. It may be asymptomatic in some cases, but most cases develop a prodrome of fever, anorexia, irritability, and the development of painful oral lesions. Associated symptoms include malaise, lethargy, and cervical or submandibular lymphadenopathy.[8]
The initial sign of herpetic gingivostomatitis is hyperemia of the oral and perioral mucosa, followed by rapidly spreading vesicular lesions on the gingiva, palate, buccal, and labial mucosa. The lesions may ulcerate and then eventually rupture. On physical examination, they may appear flat, yellowish in color, and approximately 2 to 5 mm in size. The ulcers are quick to bleed and typically heal without scarring in 2 to 3 weeks.
Recurrent herpes lesions commonly develop in one-third of the patients who have experienced primary herpetic gingivostomatitis. The patient’s symptoms include burning and itching, followed by the formation of vesicular lesions in a localized area. The lesions mostly develop on keratinized skin such as the vermillion border of the lips, perioral skin, or the hard palate. The lesions may develop when the patient is under physical or emotional stress or systemic illness. Other triggers include sunlight exposure and trauma. The lesions occur in the same area during every episode of recurrence, and systemic manifestations such as malaise and lymphadenopathy are mild.[9]
Evaluation
The diagnosis of herpetic gingivostomatitis is usually clinical, based on the patient’s history and physical examination. The appearance of the oral vesicular and ulcerative lesions is sufficient for the diagnosis. However, if additional testing is required, herpetic gingivostomatitis can be confirmed using a direct immunofluorescent examination of ulcer scrapings or blister fluid. Another test that can be used but is not entirely reliable for diagnosis is the Tzanck smear, which shows the cytologic changes induced by the herpes virus. The Tzanck smear will confirm the presence of a virus in the active lesions but fails to distinguish between HSV-1, HSV-2, and varicella-zoster virus.[10] The gold standard for diagnosis is the isolation of the virus in tissue culture. Antibody testing can help demonstrate seroconversion but does not yield a diagnosis.
Treatment / Management
Herpes gingivostomatitis is generally a mild and self-limited condition, and supportive care is generally adequate. Barrier lip creams such as petroleum jelly have been suggested to prevent adhesions in patients with active herpetic gingivostomatitis. The most important component in the management of herpetic gingivostomatitis is hydration. Adequate hydration is often achieved with pain control; thus, analgesics such as oral acetaminophen and oral rinses are encouraged to make the patient more comfortable and promote fluid intake. It is important to note that patients who are unable to drink to maintain proper hydration should be hospitalized. Other indications for hospitalization include immunocompromised children, patients who develop eczema herpeticum, and HSV spread that results in encephalitis or pneumonitis.[11](B3)
Several studies suggest the usage of acyclovir cream or oral suspension in a rinse and swallow technique.[7] Immunocompetent patients with significant pain or refusal to drink can be administered oral acyclovir if they present within the first 72 hours of disease onset.[12](A1)
Differential Diagnosis
Despite the largely based clinical diagnosis of herpetic gingivostomatitis, it is important first to rule out other diseases that present similarly, keeping in mind the age group and past medical history of the patient. Table 1 explains the differences in causation and clinical presentation of several childhood disorders that may be confused with herpes gingivostomatitis. Some of the differential diagnoses to keep in mind when considering herpetic gingivostomatitis include:
- Herpes zoster
- Primary chickenpox
- Behcet disease
- Herpetiform aphthae
- Erythema multiforme
- Acute necrotizing gingivostomatitis
- Reactive arthritis
- Cytomegalovirus ulceration
- Traumatic ulcers
- Burns, chemical and thermal
- Factitial injuries
- Vesiculobullous disease
Complications
Complications of herpetic gingivostomatitis may include:[13]
- Dehydration
- Herpes labialis
- HSV encephalitis
- Herpetic whitlow
- Herpetic keratitis
- Eczema herpeticum[14]
Deterrence and Patient Education
The patients and their families should be informed that the disease is generally mild and self-limited. They should be told about the appropriate management strategy that includes supportive care with pain control, adequate hydration, and a healthy diet. The patients should be managed at home but should be monitored closely for the development of any complications, such as difficulty in eating or drinking, or worsening of lesions. The patients and their families (especially in the case of young children) should be in regular contact with the primary treating physician. The patient should also be educated about the recurrence of the oral lesions (herpes labialis or cold sores) that may develop in one-third of the patients who develop primary herpetic gingivostomatitis.
Enhancing Healthcare Team Outcomes
Herpes gingivostomatitis is a viral infection characterized by high-grade fever and painful oral lesions, occurring most commonly in children from ages 6 months to 5 years. Out-patient management is sufficient in most situations, but hospital admission may be warranted if the patient develops complications. The disease is best managed by an interprofessional team that includes a primary care provider, an internist, a pediatrician, a nurse practitioner, an emergency department physician, an infectious disease specialist, and a pharmacist. Coordination by different health care experts is necessary to improve patient outcomes and enhance patient care.
Media
(Click Image to Enlarge)
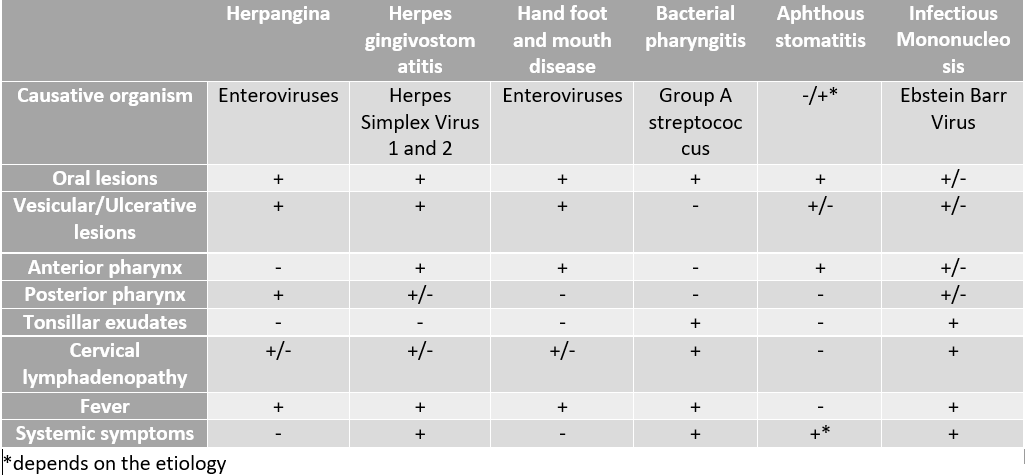
Differential diagnosis of pediatric oral lesions Contributed by Rimsha Ali, MD
References
Tovaru S, Parlatescu I, Tovaru M, Cionca L. Primary herpetic gingivostomatitis in children and adults. Quintessence international (Berlin, Germany : 1985). 2009 Feb:40(2):119-24 [PubMed PMID: 19169443]
Level 2 (mid-level) evidenceArduino PG, Porter SR. Herpes Simplex Virus Type 1 infection: overview on relevant clinico-pathological features. Journal of oral pathology & medicine : official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology. 2008 Feb:37(2):107-21. doi: 10.1111/j.1600-0714.2007.00586.x. Epub [PubMed PMID: 18197856]
Level 3 (low-level) evidenceGeorge AK, Anil S. Acute herpetic gingivostomatitis associated with herpes simplex virus 2: report of a case. Journal of international oral health : JIOH. 2014 Jun:6(3):99-102 [PubMed PMID: 25083042]
Level 3 (low-level) evidenceTaieb A, Body S, Astar I, du Pasquier P, Maleville J. Clinical epidemiology of symptomatic primary herpetic infection in children. A study of 50 cases. Acta paediatrica Scandinavica. 1987 Jan:76(1):128-32 [PubMed PMID: 3031926]
Level 3 (low-level) evidenceCataldo F, Violante M, Maltese I, Traverso G, Paternostro D. [Herpetic gingivostomatitis in children: the clinico-epidemiological aspects and findings with acyclovir treatment. A report of the cases of 162 patients]. La Pediatria medica e chirurgica : Medical and surgical pediatrics. 1993 Mar-Apr:15(2):193-5 [PubMed PMID: 8321723]
Level 2 (mid-level) evidenceLeinweber B, Kerl H, Cerroni L. Histopathologic features of cutaneous herpes virus infections (herpes simplex, herpes varicella/zoster): a broad spectrum of presentations with common pseudolymphomatous aspects. The American journal of surgical pathology. 2006 Jan:30(1):50-8 [PubMed PMID: 16330942]
Level 2 (mid-level) evidenceMohan RP, Verma S, Singh U, Agarwal N. Acute primary herpetic gingivostomatitis. BMJ case reports. 2013 Jul 8:2013():. doi: 10.1136/bcr-2013-200074. Epub 2013 Jul 8 [PubMed PMID: 23839615]
Level 3 (low-level) evidenceYarom N, Buchner A, Dayan D. Herpes simplex virus infection: part I--Biology, clinical presentation and latency. Refu'at ha-peh veha-shinayim (1993). 2005 Jan:22(1):7-15, 84 [PubMed PMID: 15786655]
Leung AKC, Barankin B. Herpes Labialis: An Update. Recent patents on inflammation & allergy drug discovery. 2017:11(2):107-113. doi: 10.2174/1872213X11666171003151717. Epub [PubMed PMID: 28971780]
Mortazavi H, Safi Y, Baharvand M, Rahmani S. Diagnostic Features of Common Oral Ulcerative Lesions: An Updated Decision Tree. International journal of dentistry. 2016:2016():7278925 [PubMed PMID: 27781066]
Faden H. Management of primary herpetic gingivostomatitis in young children. Pediatric emergency care. 2006 Apr:22(4):268-9 [PubMed PMID: 16651921]
Level 3 (low-level) evidenceAmir J, Harel L, Smetana Z, Varsano I. Treatment of herpes simplex gingivostomatitis with aciclovir in children: a randomised double blind placebo controlled study. BMJ (Clinical research ed.). 1997 Jun 21:314(7097):1800-3 [PubMed PMID: 9224082]
Level 1 (high-level) evidenceAmir J, Harel L, Smetana Z, Varsano I. The natural history of primary herpes simplex type 1 gingivostomatitis in children. Pediatric dermatology. 1999 Jul-Aug:16(4):259-63 [PubMed PMID: 10469407]
Tamay Z, Ozcekert D, Onel M, Agacfidan A, Guler N. A child presenting with primary gingivostomatitis and eczema herpeticum. Minerva pediatrica. 2016 Feb:68(1):72-3 [PubMed PMID: 26864720]