
Introduction
Since the first step out of the marine world, the animals had to adapt to the lack of fluid and electrolytes found in abundance in seawater. Over time these creatures have developed a kidney capable of regulating salt and water retention. It is the most distal part of the nephron that is responsible for this regulation. When defective, the mechanisms that hold the maintenance of our effective plasma volume will cause electrolytes disturbance apparently unrelated but potentially dangerous, mainly hypokalemia and metabolic alkalosis. This activity will evaluate the function of the thick ascending limb and the distal convoluted tubule as well as the connecting tubule and their principal cells.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Low Blood Pressure
- Genetic diseases
- Bartter syndrome
- Gitelman syndrome
- Autosomal dominant hypocalcemia with hypercalciuria (ADHH)
- Acquired diseases
- Diuretic use
- Vomiting
High Blood Pressure
- Genetic disease
- Liddle Syndrome
- 11-beta-HSdehydrogenase inactivating mutation
-
Acquired diseases
- Conn disease/secreting adenoma of the adrenal glands/bilateral hyperplasia
- Cushing disease/tumor of the adrenals
- Chronic administration of corticosteroid
- Natural licorice abuse
Epidemiology
The diseases described in this activity are infrequent. However, the symptoms with which they present are more commonly induced by mimicking their features with medications, mostly diuretic abuse or steroid use/abuse and/or vomiting.
The primary care physician will encounter hypokalemic metabolic alkalosis as a result of therapy or abuse of the agents prescribed.
Pathophysiology
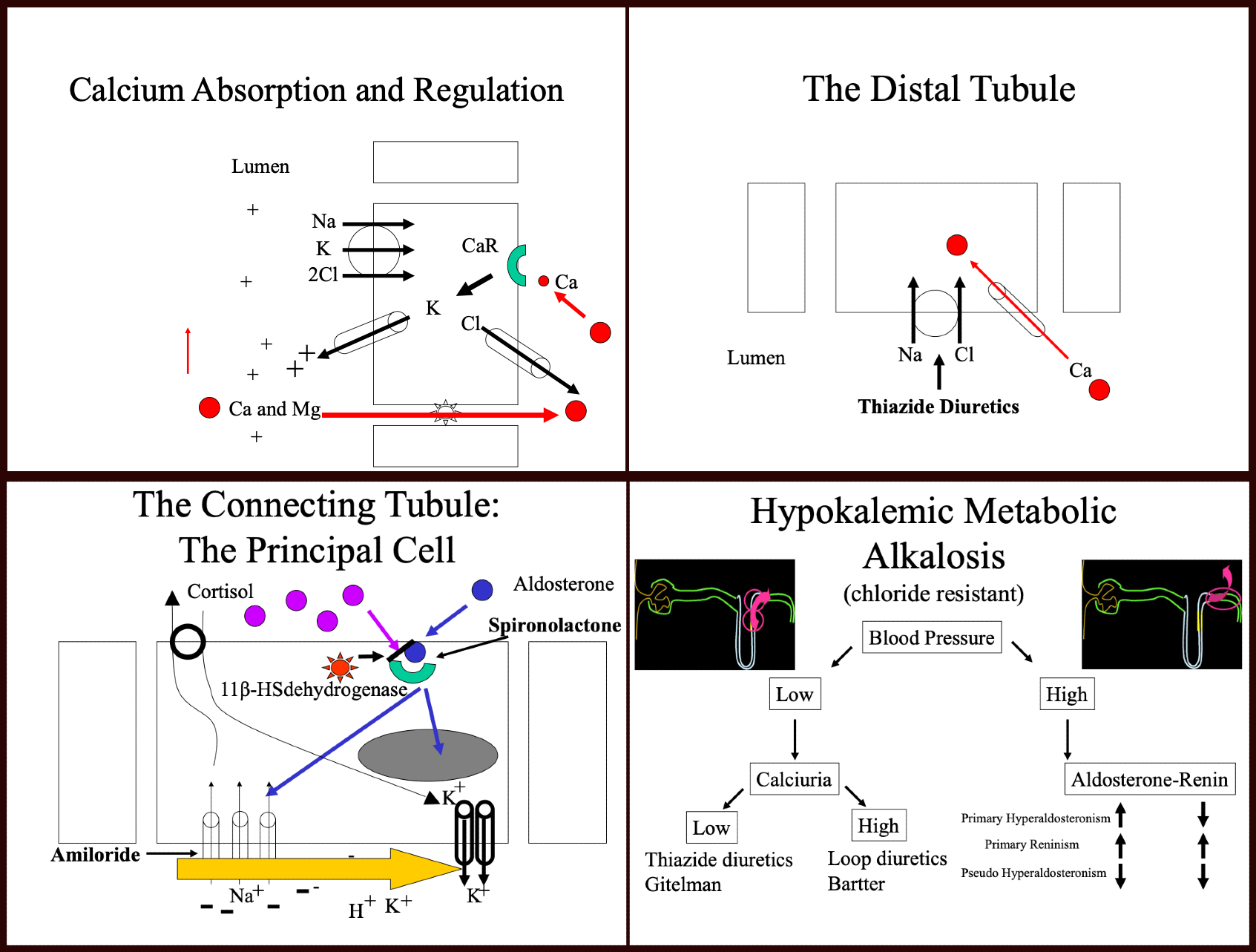
Thick ascending limb of Henle
[DIAGRAM 1]
Bartter syndrome, which presents as a salt-wasting disease with hypokalemia, was initially described in 1962 and thought to be already a genetic disease.[1] Multiple cases were then described as such, and nephrologists started to study the genetics of the disease.
Early studies of renal physiology demonstrated that most of the lumen of the nephron has a negative charge except in the thick ascending limb of Henle, which led to the discovery of sodium and chloride transport in this part of the nephron. It appears that chloride first binds to the transporter, followed then by sodium and potassium. It is this first move of chloride that leaves a positive charge in the lumen. Researchers later identified this transporter as NKCC2.[2] Renal physiologists already knew at the time (Kokko, Imai) that loop diuretics (furosemide) inhibited this transporter. It appeared that the mutation of NKCC2 could not account for all the cases of Bartter syndrome. Hence, more studies followed.
Potassium is not abundant in this segment of the nephron and is however necessary for the transport of sodium and chloride by NKCC2. It felt intuitively that potassium needed to be recycled by the thick ascending limb cells into the lumen. Also, creating a more positive charge. That intuition led to the discovery of the ROMK channel.[3]
This potassium channel gets expressed at the luminal side of the cell and, when available, allow potassium to travel down their concentration gradient into the lumen. Any genetic defect of this channel will cause Bartter syndrome (now called Barter syndrome Type II).
That still did not account for all the patients with Bartter syndrome. The ingenuity of nephrology physiologists led to think that maybe chloride played a role in some cases of Bartter syndrome. Sure enough, researchers discovered a mechanism that transports chloride to the interstitium.[4] The responsible molecule is a chloride channel that is expressed at the apical side of the thick ascending cell and allows chloride to flow from the intracellular component to the interstitium of the renal cortex. A genetic mutation of that channel was described and caused Bartter Syndrome Type III. If most of the patients with Bartter syndrome fall in these three categories, there are still cases that cannot be explained by a mutation of one of these three genes. One example is an association found between Bartter syndrome and activation of the calcium-sensing receptor (CASR).[5] It appears that the constant activation of the CASR inhibits the function of the potassium channel (ROMK), as in Bartter Type II. It is most probable that more similar discoveries will come to account for all Bartter syndrome cases.
The diagnosis of Bartter syndrome results from the association of volume depletion, metabolic alkalosis, hypokalemia, and hypercalciuria. To explain the hypercalciuria, we need to review the calcium absorption in the thick ascending limb of Henle.
As most molecules, most of the calcium undergoes reabsorption in the proximal tubule.[6] A more fine-tuned regulation of calcium is made in the thick ascending limb through a paracellular pathway involving paracellin 1 (claudin 16).[7] An electrical gradient drives calcium and magnesium from a positively charged lumen towards the interstitium. A functional paracellular molecule is essential to this reabsorption. When the positive charges become decreased in the thick ascending limb, calcium is then retained in the lumen and lost in the urine, causing "hypercalciuria." This condition is a known feature of Bartter’s syndrome as well as loop diuretic use.
Much more common conditions can mimic these diseases:
- Loop Diuretic use or abuse
- Induced Vomiting
- The Distal Convoluted Tubule (DCT) [Diagram 2]
In the DCT, sodium is absorbed through a sodium chloride cotransporter (NCC).[8] It causes a salt-wasting syndrome described initially by Dr. Gitelman.[9] The syndrome features volume depletion, hypokalemia, metabolic alkalosis, and hypomagnesemia, as well as hypocalciuria. There are controversies as of the cause of hypocalciuria.[6] Initially thought to be a change of membrane potential by inhibition of NCC. This change in membrane potential would open the calcium channel (ECaC) present in the luminal side of the cell and so increase calcium absorption in this segment of the tubule.[10] Others have shown differently and have proved that it is, in fact, the reduced extracellular volume (ECV), which causes enhanced proximal tubule calcium reabsorption.[6][11]
More common conditions can mimic this disease:
- Thiazide use or abuse
- Induced vomiting
Earlier, this activity described salt-wasting conditions accompanied by hypokalemic metabolic alkalosis. It will now review salt retention conditions with hypokalemic metabolic alkalosis, which involve the principal cells of the connecting/collecting duct.
[Diagram 3]
Early experiments have shown that increased urine flow through the distal part of the nephron induces potassium losses. That finding led to the discovery that potassium excretion is proportionally related to the sodium content of this segment of the tubule. Further electrophysiological studies have shown that electrical charges in this segment were responsible for this effect.[12] Aggressive sodium reabsorption regulated by the renin-angiotensinogen aldosterone system (RAAS) leaves a negative charge in the lumen and so traps other positively charged ions, including protons and potassium. Potassium itself is highly regulated by aldosterone, which upon binding to its intracellular receptor, induces increased expression of epithelial sodium channels (ENaC) and potassium channels, which leads to sodium absorption and potassium excretion. Aldosterone secretion is regulated by renin secretion, itself controlled by the loss of volume in the distal convoluted tubule.
Potassium-sparing diuretics affect this segment of the nephron. Spironolactone binds and blocks the aldosterone receptor.
Amiloride blocks the sodium channel ENac.
Several syndromes affect the regulation of this system.
Primary Hyperaldosteronism
Dr. Conn initially described this syndrome and is due to excessive secretion of aldosterone by the zona glomerulosa of the adrenal gland. The histopathology will not be reviewed here. Excess of aldosterone binding to its receptor in the principal cells will, as mentioned, increase the expression of ENaC and potassium channels on the luminal side of those cells; this will dramatically increase sodium absorption and potassium excretion in the tubule. The excess of sodium absorption will leave a negatively charged lumen, which will augment potassium trapping in the lumen as well as protons leading to hypokalemia and metabolic alkalosis.
The treatment of this condition, in addition to blood pressure control, is the administration of spironolactone or eplerenone.
After the initial cases of Conn syndrome, multiple patients demonstrated similar features.
Primary Reninism
In 1967 a case of HTN due to a renin-secreting tumor was reported which led to the description by Dr. Conn of primary reninism.
The features of this syndrome are almost identical to primary hyperaldosteronism including volume retention, severe hypertension, and hypokalemic metabolic alkalosis with the only difference being that the culprit of all the clinical findings is an excess secretion of renin.
Evaluations of multiple patients with hypertension and hypokalemic metabolic alkalosis left many cases without an increase in aldosterone secretion to be called pseudohyperaldosteronism.
Liddle Syndrome
Initially described in 1963 by Dr. Liddle as a "familial renal disorder simulating primary hyperaldosteronism but with negligible aldosterone secretion" (Liddle G.W et al. 1963) was further determined to be a genetic mutation of the epithelial sodium channel inducing its overexpression at the luminal side of the principal cell causing unregulated absorption of sodium.[13] As in primary hyperaldosteronism, this causes hypertension, volume retention, and hypokalemic metabolic alkalosis. However, aldosterone and renin levels become decreased. In addition to treating hypertension, amiloride improves this condition.
Cushing Syndrome (Glucocorticoid excess)
Initially described by Dr. Cushing in 1932.[14] This disease causes the overstimulation of the corticoid receptor in the principal cells due to excess production of cortisol by the follicular layer of the adrenal gland. Upon binding to its receptor, cortisol has the same if not better affinity to the aldosterone receptor than aldosterone itself. There are many more molecules of cortisol than aldosterone in the serum, and this would overstimulate the receptor if it weren't for an enzyme (11-beta-HSdehydrogenase) which quickly converts cortisol to cortisone and renders it unable to bind the receptor. In the face of significant glucocorticoid excess, this enzyme is overwhelmed and leaves some of the hormones to bind the aldosterone receptor leading to an apparent aldosterone excess, which, in turn, induces volume retention, hypertension, and hypokalemia, and metabolic alkalosis but low aldosterone and low renin.
The use or abuse of steroids can mimic this.
Apparent Mineralocorticoid Excess
Even in the absence of glucocorticoid excess, several cases of apparent mineralocorticoid excess were described. It was found to be due to a genetic mutation of 11-beta-HSdehydrogenase which leaves the aldosterone receptor available to be bound by cortisol and leads to volume retention, hypertension, hypokalemia, and metabolic alkalosis.[15]
Of note, 11-beta-HSdehydrogenase can be inhibited by glycyrrhizic acid contained in natural licorice, and it is a well-known fact that the consumption of large amounts of licorice causes HTN with apparent mineralocorticoid excess.
History and Physical
There are not many findings in the history and physical for these conditions except for blood pressure findings low or elevated and the possible history of medication use and abuse and, of course, more rarely family history in Bartter, Gittleman, and Liddle syndrome.
Evaluation
Most of these cases are discovered incidentally on routine blood work, including potassium level and bicarbonate level and simple physical exam leading to a diagnosis of low blood pressure vs. high blood pressure. Further evaluation, as seen in the previous paragraphs, is necessary for the low blood pressure arm of the diagram. Urine calcium measurements will lead to the differential diagnosis between Bartter/ loop diuretic use or abuse (high calciuria) and Gittleman syndrome/thiazide use or misuse (hypocalciuria and hypomagnesemia). For the high blood pressure arm of the diagram, one must obtain the level of aldosterone and renin concomitantly, which will separate the three most common syndromes. High renin and high aldosterone is present in primary reninism. Low renin and high aldosterone is present in primary hyperaldosteronism, and low renin and low aldosteronism is present in pseudohypoaldosteronism.
Treatment / Management
As described in the pathophysiology, the treatment of the low blood pressure section of the diagram will be to evaluate the possibility of diuretic use or abuse and or induced vomiting and provide ample volume and potassium administration. For the high blood pressure section of the diagram, it would be the use of the appropriate diuretics, spironolactone for hyperaldosteronism, and amiloride for pseudohyperaldosteronism as well as potassium for both conditions.
Differential Diagnosis
The differential diagnosis is described in the history and physical and evaluation and summarized in the diagram below:
- Bartter syndrome
- Congenital chloride-losing diarrhea
- Glucocorticoid therapy and Cushing syndrome
- Hyperaldosteronism
- Hypercalciuria
- Hypomagnesemia
- Milk-alkali syndrome
- Pediatric hypercalcemia
- Pediatric hypokalemia
- Pediatric hyponatremia
- Posthypercapnic alkalosis
- Sinonasal manifestations of cystic fibrosis
- Uric acid stones
[Diagram 4]
Prognosis
Most of the genetic diseases inducing low blood pressure are usually detected in childhood with much more severe symptoms in the Bartter variety than in the Gitleman variety and so far has not affected the life span of those individuals. As for the high blood pressure category of diseases, it is clear that when a tumor is found (reninoma), leading to primary hyperaldosteronism and glucocorticoid excess, it requires surgical excision, and the genetic diseases can lead to complications of hypertension including, strokes, coronary artery disease, and end-stage kidney disease. Induced syndromes will have to be treated accordingly by changing the medication regimen or psychiatric evaluation but usually have a good prognosis.
Complications
The complications of the diseases described above are mostly related to the danger of hypokalemia with cardiac complications and the risks of hypertension.
Deterrence and Patient Education
It is essential to educate patients about their health. A patient placed on a diuretic needs to understand the consequences of overuse or underuse. The patient also needs to be aware that any symptoms of high blood pressure, dizziness, or change in normal behavior should prompt them to see a physician.
Enhancing Healthcare Team Outcomes
Patient care is an interprofessional task at all times. The clinician is only aware of the patient's circumstances during their visit. Any overuse of medications and early prescription refills should be acknowledged and reported by the pharmacists to reduce abuse. Any other clinician or nurse seeing the patient and noticing changes, such as hypertension, dizziness, signs of vomiting, and dehydration, should discuss this with all the clinicians involved in the patient's care. The pharmacist should verify all dosing for potassium repletion as well as any diuretic therapy. These will be administered by nursing, who will also be the first to evaluate therapeutic effects and adverse events associated with medication treatment and report these to the clinician in charge of the case. Nursing must be vigilant in monitoring and report to the clinicians any status changes; they can also check patient compliance and answer patient questions. A collaborative interprofessional healthcare team approach is necessary for optimal patient outcomes, given the rarity and potential differentials for hypokalemic acidosis. [Level 5]
Media
(Click Image to Enlarge)
Metabolic Alkalosis Diagram
Contributed by Farah Leclercq, MD
References
BARTTER FC, PRONOVE P, GILL JR Jr, MACCARDLE RC. Hyperplasia of the juxtaglomerular complex with hyperaldosteronism and hypokalemic alkalosis. A new syndrome. The American journal of medicine. 1962 Dec:33():811-28 [PubMed PMID: 13969763]
Simon DB, Karet FE, Hamdan JM, DiPietro A, Sanjad SA, Lifton RP. Bartter's syndrome, hypokalaemic alkalosis with hypercalciuria, is caused by mutations in the Na-K-2Cl cotransporter NKCC2. Nature genetics. 1996 Jun:13(2):183-8 [PubMed PMID: 8640224]
Jeck N, Derst C, Wischmeyer E, Ott H, Weber S, Rudin C, Seyberth HW, Daut J, Karschin A, Konrad M. Functional heterogeneity of ROMK mutations linked to hyperprostaglandin E syndrome. Kidney international. 2001 May:59(5):1803-11 [PubMed PMID: 11318951]
Level 3 (low-level) evidenceSimon DB, Bindra RS, Mansfield TA, Nelson-Williams C, Mendonca E, Stone R, Schurman S, Nayir A, Alpay H, Bakkaloglu A, Rodriguez-Soriano J, Morales JM, Sanjad SA, Taylor CM, Pilz D, Brem A, Trachtman H, Griswold W, Richard GA, John E, Lifton RP. Mutations in the chloride channel gene, CLCNKB, cause Bartter's syndrome type III. Nature genetics. 1997 Oct:17(2):171-8 [PubMed PMID: 9326936]
Watanabe S, Fukumoto S, Chang H, Takeuchi Y, Hasegawa Y, Okazaki R, Chikatsu N, Fujita T. Association between activating mutations of calcium-sensing receptor and Bartter's syndrome. Lancet (London, England). 2002 Aug 31:360(9334):692-4 [PubMed PMID: 12241879]
Level 3 (low-level) evidenceNijenhuis T, Vallon V, van der Kemp AW, Loffing J, Hoenderop JG, Bindels RJ. Enhanced passive Ca2+ reabsorption and reduced Mg2+ channel abundance explains thiazide-induced hypocalciuria and hypomagnesemia. The Journal of clinical investigation. 2005 Jun:115(6):1651-8 [PubMed PMID: 15902302]
Level 3 (low-level) evidenceSimon DB, Lu Y, Choate KA, Velazquez H, Al-Sabban E, Praga M, Casari G, Bettinelli A, Colussi G, Rodriguez-Soriano J, McCredie D, Milford D, Sanjad S, Lifton RP. Paracellin-1, a renal tight junction protein required for paracellular Mg2+ resorption. Science (New York, N.Y.). 1999 Jul 2:285(5424):103-6 [PubMed PMID: 10390358]
Simon DB, Nelson-Williams C, Bia MJ, Ellison D, Karet FE, Molina AM, Vaara I, Iwata F, Cushner HM, Koolen M, Gainza FJ, Gitleman HJ, Lifton RP. Gitelman's variant of Bartter's syndrome, inherited hypokalaemic alkalosis, is caused by mutations in the thiazide-sensitive Na-Cl cotransporter. Nature genetics. 1996 Jan:12(1):24-30 [PubMed PMID: 8528245]
Level 3 (low-level) evidenceGitelman HJ, Graham JB, Welt LG. A new familial disorder characterized by hypokalemia and hypomagnesemia. Transactions of the Association of American Physicians. 1966:79():221-35 [PubMed PMID: 5929460]
Level 3 (low-level) evidenceNijenhuis T, Hoenderop JG, Loffing J, van der Kemp AW, van Os CH, Bindels RJ. Thiazide-induced hypocalciuria is accompanied by a decreased expression of Ca2+ transport proteins in kidney. Kidney international. 2003 Aug:64(2):555-64 [PubMed PMID: 12846750]
Level 3 (low-level) evidenceEllison DH. Divalent cation transport by the distal nephron: insights from Bartter's and Gitelman's syndromes. American journal of physiology. Renal physiology. 2000 Oct:279(4):F616-25 [PubMed PMID: 10997911]
Level 3 (low-level) evidenceGiebisch GH, Wingo CS. Renal potassium homeostasis: a short historical perspective. Seminars in nephrology. 2013 May:33(3):209-14. doi: 10.1016/j.semnephrol.2013.05.001. Epub [PubMed PMID: 23953798]
Level 3 (low-level) evidenceHansson JH, Nelson-Williams C, Suzuki H, Schild L, Shimkets R, Lu Y, Canessa C, Iwasaki T, Rossier B, Lifton RP. Hypertension caused by a truncated epithelial sodium channel gamma subunit: genetic heterogeneity of Liddle syndrome. Nature genetics. 1995 Sep:11(1):76-82 [PubMed PMID: 7550319]
Level 3 (low-level) evidenceBertagna X, Guignat L, Groussin L, Bertherat J. Cushing's disease. Best practice & research. Clinical endocrinology & metabolism. 2009 Oct:23(5):607-23. doi: 10.1016/j.beem.2009.06.001. Epub [PubMed PMID: 19945026]
Agarwal AK, Giacchetti G, Lavery G, Nikkila H, Palermo M, Ricketts M, McTernan C, Bianchi G, Manunta P, Strazzullo P, Mantero F, White PC, Stewart PM. CA-Repeat polymorphism in intron 1 of HSD11B2 : effects on gene expression and salt sensitivity. Hypertension (Dallas, Tex. : 1979). 2000 Aug:36(2):187-94 [PubMed PMID: 10948076]
Level 1 (high-level) evidence