Introduction
Hypothyroid myopathy, observed in 30% to 80% of individuals with hypothyroidism, manifests in both congenital and acquired cases, presenting with generalized myalgias, muscle weakness, and muscle pain or stiffness. Thyroid hormone is pivotal for metabolism, growth, and organ function, thus influencing the musculoskeletal system. Severe or untreated hypothyroidism can lead to substantial muscle disease, resulting in severe functional limitations.[1]
The symptoms of hypothyroid myopathy can be gradual in onset and nonspecific, necessitating a high index of suspicion from clinicians to differentiate this condition from fatigue and other muscle disorders with similar presentations. All patients diagnosed with hypothyroidism should be questioned about musculoskeletal symptoms. Proximal muscles, such as those in the thighs, hips, shoulders, and neck, are particularly affected, impacting activities such as stair climbing, rising from a seated position, and lifting objects.[2] Rarely, severe hypothyroid myopathy can result in muscle necrosis, acute compartment syndrome, or respiratory failure.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Hypothyroid myopathy is a condition that occurs when the thyroid gland does not produce enough thyroid hormones. These hormones play a crucial role in the body's metabolism, including the metabolism of muscles. Consequently, low levels of thyroid hormones can result in muscle weakness, fatigue, and other symptoms. Some common causes of hypothyroidism are listed below.
-
Autoimmune disorders: Hashimoto thyroiditis is an autoimmune disorder in which the body's immune system attacks the thyroid gland, leading to hypothyroidism. This disorder stands as the most common cause of hypothyroidism in the developed world.
-
Iodine deficiency: Iodine is an essential nutrient that is required for the production of thyroid hormones. Insufficient iodine in the diet can lead to hypothyroidism and hypothyroid myopathy, making it the most prevalent cause worldwide.[3]
-
Thyroid surgery or radiation therapy: Surgery or radiation therapy to the thyroid gland can damage the gland or reduce its function, resulting in hypothyroidism and hypothyroid myopathy.[4]
-
Medications: Certain medications, such as lithium, can interfere with the production of thyroid hormones.
-
Congenital hypothyroidism: An underactive thyroid gland at birth can cause significant developmental delays and physical deficiencies.
-
Aging: The natural aging process may cause a decline in thyroid function.[5]
Overall, hypothyroid myopathy is caused by a lack of thyroid hormones in the body, which can be due to a variety of factors such as autoimmune disorders, iodine deficiency, thyroid surgery, medications, congenital hypothyroidism, and aging.
Epidemiology
Hypothyroidism is one of the most commonly diagnosed medical conditions, affecting up to 12% of Americans during their lifetime.[6] Women are affected more often compared to men, and it can manifest at any age, although it is commonly observed between the ages of 40 and 70. No specific racial predilection has been identified in studies regarding this condition. The prevalence of hypothyroidism also increases with age, with older adults being more affected compared to younger individuals.
Pathophysiology
The pathophysiology of hypothyroid myopathy is not fully understood. Thyroid hormones significantly influence cellular metabolism, and their deficiency causes impairment of the cell's normal functioning. Serum T3 is a primary regulator of skeletal muscle mitochondrial function.[7] Hypothyroid myopathy is likely secondary to metabolism alterations resulting in aberrant glycogen and oxidative metabolism in the actin-myosin unit.[8] Thyroxine (T4) deficiency results in a reduced mitochondrial oxidative capacity, abnormal glycogenolysis, and an insulin-resistant state of the cell. Consequently, there is a selective atrophy of type 2 muscle fibers (fast-twitching type) as they depend on glycolysis for energy, leading to the slowing of muscle contraction observed clinically in patients with hypothyroidism.[7] Oxidative damage also likely causes muscle cell injury and rhabdomyolysis.[9]
Muscle hypertrophy is believed to be a compensatory response to the accumulation of glycosaminoglycans in the muscle. An increase in connective tissue and muscle fibers also contributed to this hypertrophy. There is also a decrease in muscle carnitine in patients with thyroid dysfunction, causing myopathic symptoms. The muscle involvement in hypothyroidism is caused by alterations in muscle fibers from fast-twitching type 2 to slow-twitching type 1 fibers, deposition of glycosaminoglycans, poor contractility of actin-myosin units, low myosin ATPase activity, and low ATP turnover in skeletal muscle.[10]
Notably, the degree of muscle weakness does not always correlate with the severity of thyroid hormone deficiency, suggesting that besides impaired muscle function, structural muscle injury might have a role in the pathogenesis of myopathy in some cases. Changes in muscle cell membrane permeability can result in elevated levels of serum muscle enzyme in the absence of symptoms or structural abnormalities, and reduced clearance of these enzymes can also contribute to muscle injury.
Animal studies have shown that thyroid hormones regulate the gene expression of skeletal muscle proteins such as myosin ATPase, strengthening the role of thyroid hormone deficiency in the pathogenesis of hypothyroid myopathy.
Histopathology
Microscopic examination of hypothyroid myopathy may reveal the following findings:
-
Muscle fiber atrophy: Decrease in the size of muscle fibers due to inadequate thyroid hormone levels, leading to muscle weakness.
-
Increased connective tissue: Accumulation of connective tissue within the muscle, which can contribute to muscle stiffness and weakness.
-
Fiber type changes: Shift in muscle fiber types, with a decrease in fast-twitch fibers (Type II) and an increase in slow-twitch fibers (Type I). This alteration can affect muscle function and endurance.
-
Vacuolar changes: Presence of vacuoles within muscle fibers, which may contain cellular debris or lipid droplets. These vacuoles can disrupt muscle structure and function.
-
Myopathic changes: Features such as fiber necrosis (death of muscle fibers), regeneration (attempted repair of muscle tissue), and inflammatory infiltrates (immune cells infiltrating muscle tissue). These changes are typically observed in more severe cases of hypothyroid myopathy.
-
Glycogen accumulation: Increased glycogen storage within muscle fibers due to impaired glycogenolysis, leading to muscle stiffness and weakness.
-
Reduced oxidative enzyme activity: Decreased activity of oxidative enzymes in muscle fibers, which can impair energy production and muscle function.
These microscopic findings collectively contribute to the characteristic muscle weakness and dysfunction observed in hypothyroid myopathy. However, the specific findings can vary depending on the severity and duration of hypothyroidism and individual patient factors.
Toxicokinetics
Endocrine disruptors impact various metabolic pathways, but effects on the thyroid axis are especially concerning due to hypothyroidism's effects on infant and childhood development. The Organization for Economic Co-operation and Development (OECD) and the United States Environmental Protection Agency (EPA) testing strategies for identifying developmental thyroid toxicants primarily rely on serum tetraiodothyronine (T4) measurements in rodents, paralleling the clinical monitoring of pregnant women and newborns. The use of T4 measurements is historically based on the idea that hormone measurements are linearly related to receptor occupancy, thus defining thyroid hormone action. However, significant research findings in thyroid biology have challenged this dogma. Although some xenobiotic exposures may reduce thyroid hormone actions, these observations may not be applicable at all life stages.[11][12] Once testing identifies specific thyroid hormone molecular pathway disruption, toxic effects on the thyroid gland causing hypothyroid myopathy can be addressed more specifically.[6]
History and Physical
Neuromuscular manifestations of hypothyroidism frequently occur in conjunction with the common systemic symptoms, such as fatigue, weight gain, cold intolerance, and dry skin.[13] Decreased or absent deep tendon reflexes are common. Rarely, muscle and nerve dysfunction may manifest as the initial symptom of hypothyroidism, highlighting the importance of considering thyroid dysfunction when evaluating new neuromuscular symptoms.
Hypothyroid myopathy presents with nonspecific symptoms of myalgias, muscle cramps, fatigue, and muscle weakness, particularly exacerbated with exertion and exercise. Typical features of hypothyroid myopathy are described below.
Myalgia, a common manifestation of hypothyroidism, presents as nonspecific muscle stiffness or diffuse pain, often exacerbated after exercise. This symptom may be associated with elevated levels of serum muscle enzyme.[2]
Proximal myopathy is characterized by a slowly progressive, symmetric proximal muscle weakness.[14] Shoulder and hip girdle muscles are most commonly affected. Occasionally, hypothyroid myopathy is more fulminant, with markedly elevated serum muscle enzymes. On examination, deep tendon reflexes are characteristically described as hung-up due to delayed muscle relaxation.
Muscle pseudohypertrophy infrequently occurs in adults. Patients can have generalized muscular hypertrophy and variable degrees of weakness. The skin and subcutaneous tissues have a thickened, doughy appearance. Serum muscle enzymes are typically elevated. Signs of hypothyroidism are typically readily apparent and long-standing in this setting.[15][16]
Two associated syndromes related to muscle pseudohypertrophy include:
- Kocher-Debre-Semelaigne syndrome manifests in childhood and is associated with generalized muscular hypertrophy, myxoedema, short stature, and developmental delay.[17]
- Hoffmann syndrome typically occurs in adults and is characterized by pseudohypertrophy, painful spasms, proximal muscle weakness, and stiffness. This syndrome is generally observed in primary hypothyroidism and very rarely with secondary hypothyroidism. The cause of muscle pseudohypertrophy in Hoffmann syndrome is postulated to be due to the deposition of glycosaminoglycans and increased muscle fiber size. The muscles commonly involved are tongue, arm, and leg muscles.[18]
Rhabdomyolysis is a potential complication of hypothyroidism and can lead to extremely high levels of serum creatine kinase and rhabdomyolysis.[19] In some cases, this condition can be triggered by vigorous exercise, trauma, electrolyte abnormalities, alcohol consumption, or concurrent statin therapy. Renal failure may occur as a secondary complication.[20]
Myoedema refers to a small lump rising on the surface of a muscle after light pressure, such as with a percussion hammer. This phenomenon, characteristic of hypothyroid myopathy, lasts for 30 to 60 seconds due to a sustained contracture associated with delayed relaxation because of the slow reaccumulation of calcium by the sarcoplasmic reticulum.[15][21]
Acute compartment syndrome, characterized by increased pressure within a muscle compartment leading to vascular compromise, is a rare complication of hypothyroidism. Although its causative mechanisms are not clear, its syndrome can be triggered by strenuous exercise and statin or alcohol use.[22]
Evaluation
Hypothyroidism is a prerequisite for diagnosing hypothyroid myopathy and is diagnosed by measuring thyroid-stimulating hormone (TSH) and T4 levels in the blood. The most common laboratory finding in hypothyroid myopathy is an elevation in serum creatine kinase levels. However, this is not specific to myopathy, and patients may experience elevated levels of creatine kinase for many years before developing the myopathy.
Physical evaluation may include a 6-minute walking test, hand grip strength test, and timed chair standing test. These tests primarily assess proximal muscle strength.[23]
Electromyography (EMG) can demonstrate low or small amplitude potentials, which could help with diagnosis. However, this is normal in half of the patients, so a normal test does not preclude the diagnosis. Compared to myositis, there is a lack of fibrillation potentials on EMG with relatively normal motor units.[24] However, when Hoffman syndrome is present, chronic denervation can also lead to fibrillation and sharp waves.[7]
Although muscle biopsy is not necessary for diagnosis, if performed, it may show swollen and pale muscle tissue with loss of striations and increased separation between the muscle fibers due to mucinous depositions. Type I muscle fiber hypertrophy, type 2 muscle fiber atrophy, focal necrosis, and degeneration of muscle fibers may also be noted.[25] Moreover, increased numbers of internal nuclei, mitochondrial inclusions, glycogen accumulation, autophagic vacuoles, and myofibrillar disorganization are other nonspecific histopathological features that may be observed on the muscle biopsy.
Treatment / Management
The synthetic form of the thyroid hormone thyroxine (T4), levothyroxine, is the primary medication used for hypothyroidism and its associated myopathy. Levothyroxine, with a half-life of 7 days, is slowly absorbed and rapidly equilibrates in its distribution volume. However, it takes approximately 6 weeks for complete equilibration of the free thyroxine levels and to notice the clinical effects of levothyroxine. Dosage adjustments are made by monitoring free thyroxine and TSH levels, aiming for normalization within approximately 2 months. The myopathy typically improves within 2 to 3 weeks, but months may be required to resolve completely. See StatPearls' companion reference, "Hypothyroidism," for more information.
Management of hypothyroidism is the mainstay of treating hypothyroid myopathy.[14] The initial dose of levothyroxine is typically 1.6 mcg/kg body weight per day, although it may be lower for older patients or those with coronary heart disease. The dose timing is essential, and the medication should be taken on an empty stomach with water, ideally 30 to 60 minutes before a meal. If a patient has persistent symptoms after 2 to 3 weeks, they should be re-evaluated, and serum-free T4 and TSH levels should be remeasured in 3 weeks. The maintenance dose may vary based on the cause of hypothyroidism. Serum TSH levels are measured annually or more often with an abnormal result or a change in the patient's status.(B3)
According to a study, T4 requirements correlate more with lean body mass than total body weight. The study also found that the average full replacement dose after thyroidectomy varied depending on the patient's body mass index (BMI). Patients with a BMI of less than 25 kg/m2 had an average dose of 1.76 mcg/kg body weight, whereas those with a BMI between 25 and 29 kg/m2 had an average dose of 1.47 mcg/kg. Patients with a BMI between 30 and 34 kg/m2 had an average dose of 1.42 mcg/kg, whereas those with a BMI between 35 and 39 kg/m2 had an average dose of 1.27 mcg/kg. Patients with a BMI over 40 kg/m2 had an average dosage of 1.28 mcg/kg.[26]
Adrenal insufficiency should be ruled out before initiating hormonal replacement therapy to avoid an adrenal crisis that could be life-threatening.[27] With adequate thyroid hormone replacement and restoration of normal thyroid function, most patients gradually resolve most of the neuromuscular symptoms. Creatine kinase levels fall quickly with thyroxine replacement within a few weeks and may resolve before TSH normalization. Hence, this can be used as a surrogate to monitor treatment response in the initial stages, as the myopathic symptoms can take up to 6 months to resolve completely. Most of the symptoms resolve within a year of adequate hormone replacement.[14](A1)
Differential Diagnosis
The differential diagnosis of hypothyroid myopathy includes:
- Acid maltase deficiency
- Acute poliomyelitis
- Amyotrophic lateral sclerosis
- Becker muscular dystrophy
- Inclusion body myositis
- Polymyositis
- Post-polio syndrome
- Peripheral neuropathy
Toxicity and Adverse Effect Management
Although generally well-tolerated, levothyroxine can occasionally lead to adverse effects, particularly if the dosage is too high or if there are underlying medical conditions. The following list describes how the adverse effects of levothyroxine are managed in the context of hypothyroid myopathy.
-
Symptom assessment: Patients should be monitored for palpitations, tremors, anxiety, insomnia, heat intolerance, sweating, weight loss, and diarrhea.
-
Thyroid function tests: Regular monitoring of thyroid function tests, including TSH and T4, and dosage adjustment as needed is essential.
-
Gradual titration: Dosage adjustments should be made gradually to minimize the risk of abrupt changes in thyroid hormone levels, which can exacerbate symptoms or lead to adverse effects.
-
Review of medications and supplements: Certain medications and supplements can interfere with levothyroxine absorption or metabolism. Reviewing the patient's medication list and adjusting doses or avoiding interactions when possible can help optimize treatment outcomes.
When intravenous (IV) steroids or biological agents are required in patients with hypothyroid myopathy, careful monitoring and management of potential adverse effects are essential because both IV steroids and some biological agents can affect thyroid function.
-
Management of underlying conditions: Patients with underlying medical conditions such as cardiovascular disease, osteoporosis, or diabetes may require special consideration when prescribing levothyroxine.
Consultation With Endocrinologists
In cases where dosage adjustment or management of adverse effects is challenging, consultation with an endocrinologist or thyroid specialist may be warranted. These specialists can provide expertise in managing complex cases of hypothyroidism and associated myopathy.
Management of Steroid-Induced Myopathy
Steroid-induced myopathy is a potential adverse effect of IV steroids, characterized by muscle weakness and wasting. In individuals with hypothyroid myopathy, the combination of steroid-induced myopathy and underlying muscle weakness from hypothyroidism can exacerbate symptoms. Management may include physical therapy, exercise programs tailored to individual capabilities, and optimizing thyroid hormone replacement therapy to address underlying hypothyroidism.
Medical Oncology
Thyroid dysfunction and associated hypothyroid myopathy are common adverse events observed with the use of immune checkpoint inhibitors.[28] Immune checkpoint inhibitors commonly affect the endocrine system, leading to autoimmunity while treating the neoplastic process.[29] The thyroid dysfunction can present as hypothyroidism or, more rarely, thyrotoxicosis.[30]
Staging
Staging
Hypothyroid myopathy typically does not have a formal staging system similar to some other medical conditions. However, its severity can vary widely among individuals and may be assessed based on the degree of muscle weakness, functional impairment, and associated symptoms. A general framework for understanding the severity or staging of hypothyroid myopathy is as follows:
-
Mild: Patients with mild hypothyroid myopathy may experience subtle muscle weakness, fatigue, and stiffness, which may not significantly impact their daily activities. They may notice symptoms such as difficulty climbing stairs, lifting objects, or participating in physical activities.
-
Moderate: Muscle weakness and fatigue may be more pronounced in moderate cases, affecting the individual's ability to perform routine tasks. They may experience difficulty with activities requiring muscle strength and endurance, such as walking longer distances, standing from a seated position, or carrying groceries.
-
Severe: Severe hypothyroid myopathy is characterized by profound muscle weakness and fatigue, significantly impairing mobility and functional independence. Patients may struggle to perform basic activities of daily living, such as dressing, bathing, or climbing stairs, and may require assistance or mobility aids.
-
Complications: In some cases, hypothyroid myopathy can lead to complications such as falls, fractures (due to muscle weakness and impaired bone health), or respiratory compromise (due to weakness of respiratory muscles).
The severity of hypothyroid myopathy can be influenced by factors such as the duration and extent of thyroid hormone deficiency, the presence of other medical conditions or comorbidities, and individual variations in muscle function and response to treatment.
Prognosis
In general, the prognosis for hypothyroid myopathy is good with prompt and appropriate treatment.[14] Most patients experience muscle strength and function improvement with thyroid hormone replacement therapy. However, the recovery process may take some time, and patients may need to continue treatment for an extended period.
The prognosis may be poor in severe cases, particularly when diagnosis is delayed or when the patient has other underlying medical issues. In such cases, patients may experience permanent muscle damage, leading to muscle strength and function loss.
Complications
Hypothyroid myopathy may progress and lead to symptoms and complications listed below.
Muscle cramps: Hypothyroid myopathy can cause muscle cramps due to prolonged contraction of already weak muscles.
Reduced mobility: Muscle weakness and fatigue caused by hypothyroid myopathy can reduce mobility, making it difficult to perform daily activities such as walking, climbing stairs, and standing up from a seated position.
Increased risk of falls: Reduced mobility can lead to an increased risk of falls, especially in older adults. Falls can result in injuries such as fractures, further reducing mobility and quality of life.
Respiratory complications: Severe hypothyroid myopathy can weaken the muscles involved in breathing, leading to respiratory complications such as shortness of breath and difficulty breathing.
Cardiovascular complications: Hypothyroid myopathy can also affect the heart muscles, leading to cardiovascular complications such as an increased risk of heart failure and arrhythmias.
Psychological impact: Chronic muscle weakness and fatigue associated with hypothyroid myopathy can have a significant psychological impact, leading to depression, anxiety, and decreased self-esteem.
Long-term disability: In severe cases of hypothyroid myopathy, persistent muscle weakness and functional impairment may result in long-term disability, requiring ongoing support and assistance with daily activities.
Postoperative and Rehabilitation Care
Rehabilitation care for hypothyroid myopathy aims to improve muscle strength, endurance, and functional abilities through targeted interventions. Although there is no specific rehabilitation protocol for hypothyroid myopathy, general principles of rehabilitation can be applied to address muscle weakness and other symptoms associated with the condition. The components of rehabilitation care for hypothyroid myopathy are as follows:
-
Physical therapy assessment: A physical therapist can assess the patient's muscle strength, range of motion, balance, and functional abilities. They can identify areas of weakness or impairment and develop an individualized treatment plan to address these deficits.
-
Exercise therapy: Exercise is a cornerstone of rehabilitation for hypothyroid myopathy. A structured exercise program can help improve muscle strength, endurance, and mobility. Exercises may include strength, aerobics, flexibility, and balance training. The program should be adjusted over time.
-
Energy conservation techniques: Fatigue is a common symptom of hypothyroidism, and patients may benefit from learning energy conservation techniques to help manage their daily activities more efficiently. The energy conservation techniques may include pacing activities, prioritizing tasks, and using adaptive equipment or assistive devices to reduce physical strain.
-
Gait training: Patients with hypothyroid myopathy may experience difficulties with walking and mobility. Gait training exercises can help improve walking patterns, balance, and coordination. These exercises may include practicing specific gait tasks, such as heel-to-toe walking, side stepping, and stair negotiation.
-
Functional training: Rehabilitation should focus on improving the patient's ability to perform activities of daily living independently, such as dressing, bathing, grooming, and household chores. Functional training exercises can simulate real-life activities and help patients regain confidence and independence in their daily routines.
-
Education and self-management: Providing education about hypothyroidism, its impact on muscle function, and the importance of adherence to medication and lifestyle recommendations is essential. Patients should be empowered to take an active role in managing their condition and maintaining their rehabilitation progress.
-
Collaboration with other healthcare providers: Rehabilitation care for hypothyroid myopathy may involve collaboration with other healthcare providers, such as endocrinologists, neurologists, and occupational therapists, to address the multifaceted requirements of patients with hypothyroidism.
Overall, rehabilitation care for hypothyroid myopathy should be tailored to the individual patient's requirements and goals, aiming to improve muscle function, enhance functional abilities, and optimize overall quality of life. A comprehensive and multidisciplinary approach can help achieve optimal outcomes for patients with hypothyroid myopathy.
Deterrence and Patient Education
Patients should be advised to promptly inform their healthcare provider about any emergence or aggravation of muscle weakness, cramping, or myalgias as part of monitoring for hypothyroid myopathy. Regular follow-up appointments are crucial to evaluate thyroid function changes and make appropriate medication dosage adjustments as needed.
Pearls and Other Issues
Some considerations for hypothyroid myopathy management include:
- In patients with severe hypothyroid myopathy, it may be necessary to delay thyroid hormone replacement therapy until other comorbidities are managed and the patient is stable.
- Hypothyroid myopathy can present with a wide range of symptoms, including muscle weakness, cramps, stiffness, and pain.
- In some cases, hypothyroid myopathy can be the first sign of underlying hypothyroidism, and patients with unexplained muscle weakness should be screened for thyroid dysfunction.
- In patients with hypothyroid myopathy who are being treated with thyroid hormone replacement therapy, it is important to monitor thyroid function regularly to ensure they receive an adequate dose.
- Hypothyroid myopathy can affect patients of all ages, but it is more common in older adults, especially women older than 60.
Enhancing Healthcare Team Outcomes
Assessment and management of hypothyroid myopathy should be tailored to the individual patient based on the patient's clinical presentation, functional status, and response to treatment. A multidisciplinary approach involving collaboration among endocrinologists, neurologists, physical therapists, nurses, pharmacists, and other healthcare professionals is crucial to optimize care and improve outcomes for patients with hypothyroid myopathy. The primary goals are to replace the thyroid hormone, encourage physical activity, and enroll in a physical therapy program.
Every member of the interprofessional team should be empowered to bring up the possibility of hypothyroid myopathy in patients. Nurses play a vital role in patient education, progress monitoring, communication with patients and caregivers, and reporting any deterioration or improvement to the rest of the interprofessional team.
The recovery is not always immediate and may take months or even several years. Regular monitoring of creatine kinase levels is essential for assessing progress. Even after treatment, residual muscle pain and fatigue may persist in some patients. Nursing staff should assist with monitoring, follow-up, and educating the patient and family. Effective collaboration, shared decision-making, and clear communication among team members are essential for achieving favorable outcomes.
Media
(Click Image to Enlarge)
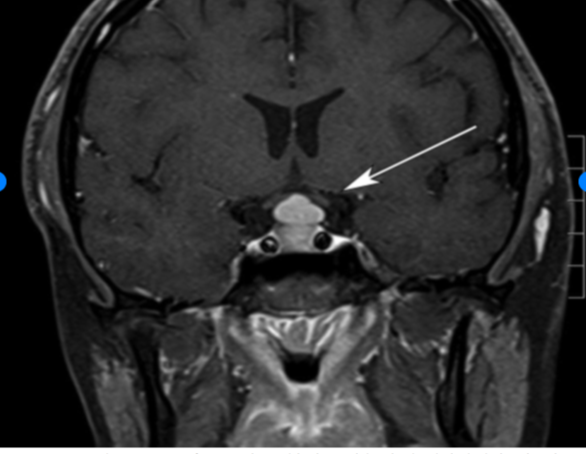
Pituitary Hyperplasia. The hyperplasia is due to primary hypothyroidism.
Siddiqi AI, Grieve J, Baldeweg SE, Miszkiel K. Tablets or scalpel: pituitary hyperplasia due to primary hypothyroidism. Radiol Case Rep. 2016;10(2):1099. doi: 10.2484/rcr.v10i2.1099.
References
Sindoni A, Rodolico C, Pappalardo MA, Portaro S, Benvenga S. Hypothyroid myopathy: A peculiar clinical presentation of thyroid failure. Review of the literature. Reviews in endocrine & metabolic disorders. 2016 Dec:17(4):499-519. doi: 10.1007/s11154-016-9357-0. Epub [PubMed PMID: 27154040]
Brzozowska MM, Banthia S, Thompson S, Narasimhan M, Lee J. Severe Hypothyroidism Complicated by Myopathy and Neuropathy with Atypical Demyelinating Features. Case reports in endocrinology. 2021:2021():5525156. doi: 10.1155/2021/5525156. Epub 2021 May 19 [PubMed PMID: 34104497]
Level 3 (low-level) evidencePearson S, Donnellan C, Turner L, Noble E, Seejore K, Murray RD. Endemic goitre and hypothyroidism in an adult female patient dependent on total parenteral nutrition. Endocrinology, diabetes & metabolism case reports. 2017:2017():. doi: 10.1530/EDM-17-0030. Epub 2017 Jun 7 [PubMed PMID: 28620494]
Level 3 (low-level) evidenceBird RJ, Bryce DP. Longterm effects of heavy irradiation to the neck. The Journal of otolaryngology. 1980 Feb:9(1):18-23 [PubMed PMID: 7359610]
Level 3 (low-level) evidenceMammen JSR. Thyroid and Aging. Endocrinology and metabolism clinics of North America. 2023 Jun:52(2):229-243. doi: 10.1016/j.ecl.2022.10.008. Epub 2023 Feb 19 [PubMed PMID: 36948777]
O'Shaughnessy KL, Gilbert ME. Thyroid disrupting chemicals and developmental neurotoxicity - New tools and approaches to evaluate hormone action. Molecular and cellular endocrinology. 2020 Dec 1:518():110663. doi: 10.1016/j.mce.2019.110663. Epub 2019 Nov 21 [PubMed PMID: 31760043]
Winter S, Heiling B, Eckardt N, Kloos C, Axer H. Hoffmann's syndrome in the differential work-up of myopathic complaints: a case report. Journal of medical case reports. 2023 Oct 31:17(1):473. doi: 10.1186/s13256-023-04184-6. Epub 2023 Oct 31 [PubMed PMID: 37907975]
Level 3 (low-level) evidenceHorak HA, Pourmand R. Endocrine myopathies. Neurologic clinics. 2000 Feb:18(1):203-13 [PubMed PMID: 10658176]
Tiniakou E, Mammen AL. Necrotizing myopathy caused by central hypothyroidism. Muscle & nerve. 2015 Jul:52(1):152-3. doi: 10.1002/mus.24637. Epub 2015 Jun 1 [PubMed PMID: 25808401]
Kaminsky P, Klein M, Duc M. [Hypothyroid myopathy. Physiopathological approach]. Annales d'endocrinologie. 1992:53(4):125-32 [PubMed PMID: 1339062]
Calvo R, Obregón MJ, Escobar del Rey F, Morreale de Escobar G. The rat placenta and the transfer of thyroid hormones from the mother to the fetus. Effects of maternal thyroid status. Endocrinology. 1992 Jul:131(1):357-65 [PubMed PMID: 1612015]
O'Shaughnessy KL, Kosian PA, Ford JL, Oshiro WM, Degitz SJ, Gilbert ME. Developmental Thyroid Hormone Insufficiency Induces a Cortical Brain Malformation and Learning Impairments: A Cross-Fostering Study. Toxicological sciences : an official journal of the Society of Toxicology. 2018 May 1:163(1):101-115. doi: 10.1093/toxsci/kfy016. Epub [PubMed PMID: 29385626]
Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet (London, England). 2017 Sep 23:390(10101):1550-1562. doi: 10.1016/S0140-6736(17)30703-1. Epub 2017 Mar 20 [PubMed PMID: 28336049]
Jervis W, Shah N, Mongolu SK, Sathyapalan T. Severe proximal myopathy secondary to Hashimoto's thyroiditis. BMJ case reports. 2019 Jul 27:12(7):. doi: 10.1136/bcr-2019-230427. Epub 2019 Jul 27 [PubMed PMID: 31352397]
Level 3 (low-level) evidenceTakkar A, Sachdeva J, Vojjala N, Lal V. Myoedema with pseudohypertrophic hypothyroid myopathy (Hoffman's syndrome). Practical neurology. 2021 Aug:21(4):360-362. doi: 10.1136/practneurol-2020-002898. Epub 2021 Mar 30 [PubMed PMID: 33785566]
Ahmed GS, Zaid HM, Moloney M. Hashimoto's thyroiditis presenting as Hoffman's syndrome, rhabdomyolysis and acute kidney injury. BMJ case reports. 2014 Jul 4:2014():. doi: 10.1136/bcr-2013-203269. Epub 2014 Jul 4 [PubMed PMID: 25100806]
Level 3 (low-level) evidenceCimbek EA, Şen Y, Yuca SA, Çam D, Gür C, Peru H. Kocher-Debré-Semelaigne syndrome with rhabdomyolysis and increased creatinine. Journal of pediatric endocrinology & metabolism : JPEM. 2015 Nov 1:28(11-12):1383-5. doi: 10.1515/jpem-2014-0411. Epub [PubMed PMID: 26181046]
Achappa B, Madi D. Hoffmann's Syndrome- A Rare Form of Hypothyroid Myopathy. Journal of clinical and diagnostic research : JCDR. 2017 May:11(5):OL01-OL02. doi: 10.7860/JCDR/2017/21234.9913. Epub 2017 May 1 [PubMed PMID: 28658840]
Zhou Q, Li B, Tian X. Rhabdomyolysis Caused by Hypothyroidism: Research Progress. Hormone and metabolic research = Hormon- und Stoffwechselforschung = Hormones et metabolisme. 2022 Nov:54(11):731-735. doi: 10.1055/a-1951-1646. Epub 2022 Nov 10 [PubMed PMID: 36356569]
Peringat J, Manappallil RG, Karadan U. Rhabdomyolysis: a rare complication of Hashimoto's thyroiditis precipitated by statin therapy. BMJ case reports. 2018 Feb 12:2018():. pii: bcr-2017-223229. doi: 10.1136/bcr-2017-223229. Epub 2018 Feb 12 [PubMed PMID: 29440138]
Level 3 (low-level) evidenceVignesh G, Balachandran K, Kamalanathan S, Hamide A. Myoedema: A clinical pointer to hypothyroid myopathy. Indian journal of endocrinology and metabolism. 2013 Mar:17(2):352. doi: 10.4103/2230-8210.109672. Epub [PubMed PMID: 23776921]
van Veelen NM, Fischli S, Beeres FJP, Eisenhut T, Babst R, Henzen C, Link BC. Compartment syndrome of the leg after thyroid hormone withdrawal; two cases and a systematic review of the literature. BMC endocrine disorders. 2020 Jun 5:20(1):80. doi: 10.1186/s12902-020-00555-y. Epub 2020 Jun 5 [PubMed PMID: 32503586]
Level 1 (high-level) evidenceGallo D, Piantanida E, Veronesi G, Lai A, Sassi L, Lombardi V, Masiello E, Premoli P, Bianconi E, Cusini C, Rosetti S, Tanda ML, Toniolo A, Ferrario M, Bartalena L. Physical performance in newly diagnosed hypothyroidism: a pilot study. Journal of endocrinological investigation. 2017 Oct:40(10):1099-1106. doi: 10.1007/s40618-017-0661-7. Epub 2017 Apr 22 [PubMed PMID: 28434158]
Level 3 (low-level) evidenceEslamian F, Bahrami A, Aghamohammadzadeh N, Niafar M, Salekzamani Y, Behkamrad K. Electrophysiologic changes in patients with untreated primary hypothyroidism. Journal of clinical neurophysiology : official publication of the American Electroencephalographic Society. 2011 Jun:28(3):323-8. doi: 10.1097/WNP.0b013e31821c30d9. Epub [PubMed PMID: 21633261]
Li Q, Bao L, Liu M, Zhang R, Shi H, Chen H. Hypothalamic hypernatremic myopathy: A single-center case series. Muscle & nerve. 2023 Mar:67(3):231-236. doi: 10.1002/mus.27781. Epub 2023 Jan 9 [PubMed PMID: 36576109]
Level 2 (mid-level) evidencePapoian V, Ylli D, Felger EA, Wartofsky L, Rosen JE. Evaluation of Thyroid Hormone Replacement Dosing in Overweight and Obese Patients After a Thyroidectomy. Thyroid : official journal of the American Thyroid Association. 2019 Nov:29(11):1558-1562. doi: 10.1089/thy.2019.0251. Epub 2019 Oct 1 [PubMed PMID: 31573413]
Brahmer JR, Lacchetti C, Schneider BJ, Atkins MB, Brassil KJ, Caterino JM, Chau I, Ernstoff MS, Gardner JM, Ginex P, Hallmeyer S, Holter Chakrabarty J, Leighl NB, Mammen JS, McDermott DF, Naing A, Nastoupil LJ, Phillips T, Porter LD, Puzanov I, Reichner CA, Santomasso BD, Seigel C, Spira A, Suarez-Almazor ME, Wang Y, Weber JS, Wolchok JD, Thompson JA, National Comprehensive Cancer Network. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2018 Jun 10:36(17):1714-1768. doi: 10.1200/JCO.2017.77.6385. Epub 2018 Feb 14 [PubMed PMID: 29442540]
Level 1 (high-level) evidenceEl Sabbagh R, Azar NS, Eid AA, Azar ST. Thyroid Dysfunctions Due to Immune Checkpoint Inhibitors: A Review. International journal of general medicine. 2020:13():1003-1009. doi: 10.2147/IJGM.S261433. Epub 2020 Nov 4 [PubMed PMID: 33177863]
Postow MA, Sidlow R, Hellmann MD. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. The New England journal of medicine. 2018 Jan 11:378(2):158-168. doi: 10.1056/NEJMra1703481. Epub [PubMed PMID: 29320654]
Iyer PC, Cabanillas ME, Waguespack SG, Hu MI, Thosani S, Lavis VR, Busaidy NL, Subudhi SK, Diab A, Dadu R. Immune-Related Thyroiditis with Immune Checkpoint Inhibitors. Thyroid : official journal of the American Thyroid Association. 2018 Oct:28(10):1243-1251. doi: 10.1089/thy.2018.0116. Epub [PubMed PMID: 30132401]