Introduction
Inferior wall myocardial infarction (MI) occurs from a coronary artery occlusion with resultant decreased perfusion to that region of the myocardium. Unless there is timely treatment, this results in myocardial ischemia followed by infarction. In most patients, the inferior myocardium is supplied by the right coronary artery. In about 6-10% of the population, because of left dominance, the left circumflex will supply the posterior descending coronary artery. Approximately 40% of all MIs involve the inferior wall. Traditionally, inferior MIs have a better prognosis than those in other regions, such as the anterior wall of the heart. The mortality rate of an inferior wall MI is less than 10%. However, several complicating factors that increase mortality, including right ventricular infarction, hypotension, bradycardia heart block, and cardiogenic shock.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Inferior wall myocardial infarctions are due to ischemia and infarction to the inferior region of the heart. In 80% of patients, the inferior wall of the heart is supplied by the right coronary artery via the posterior descending artery (PDA). In the other 20% of patients, the PDA is a branch of the circumflex artery.[4]
Epidemiology
There were 8.6 million myocardial infarctions in 2013 worldwide. Inferior wall MIs are estimated to be 40% to 50% of all MIs. They have a better prognosis than other myocardial infarctions, with a mortality of 2% to 9%. However, up to 40% of inferior wall MIs have associated right ventricular involvement that portends a worse outcome.[5]
Pathophysiology
The pathophysiology of MI involves the rupture of a coronary artery plaque, thrombosis, and blockage of the downstream perfusion leading to myocardial ischemia then necrosis. The culprit vessel in most patients is the right coronary artery that then feeds the posterior descending artery. This anatomy is said to be right dominant. A minority of patients have left dominate anatomy with the posterior coronary artery supplied from the circumflex artery. The most common ECG finding with inferior wall MI is ST elevation in ECG leads II, III and aVF with reciprocal ST depression in lead aVL. The right coronary artery perfuses the AV node, so there are associated bradycardias, heart blocks and arrhythmias associated with inferior wall MIs.[6]
History and Physical
The history should focus on the usual investigation for an acute coronary syndrome. Symptoms include chest pain, heaviness or pressure and shortness of breath, and diaphoresis with radiation to the jaw or arms. There are often other symptoms such as fatigue, lightheadedness, or nausea. On physical exam, particular attention should be given to the heart rate since bradycardia and heart block may occur. Likewise, hypotension and evidence of poor perfusion should be assessed, especially if there is concomitant right ventricular infarction.
Evaluation
Early and serial ECGs are an essential part of the evaluation. ECG leads II, III, and aVF correlate with the inferior wall of the heart (see Image. ECG With Pardee Waves Indicating AMI). ST-segment elevation in those leads indicates an inferior wall STEMI. Reciprocal ST depression often is seen in lead aVL. Almost half of the inferior wall infarctions are associated with right ventricular MIs. The addition of right-sided ECG leads should be used to examine the right ventricle. Right-sided ECGs are performed by reversing the precordial leads to the right side of the chest in a mirror image of the traditional precordial leads. Lead V4R is particularly useful for detecting a right-sided infarction. If there is evidence of ST elevation MI, the catheterization laboratory should be activated. If there is no ST elevation, troponin levels should be followed.[7]
Treatment / Management
If there is evidence of ST elevation on the ECG, the patient should be sent for emergency cardiac angiography to the catheterization lab with a goal door-to-vessel open time of under 90 minutes. Thrombolysis should be considered, depending on facility capability or anticipated long transport time to an interventional catheterization lab. If there is evidence of right ventricular infarction, avoid nitrates and provide volume to assure adequate preload. The right ventricle contains less myocardium than the left and is dependent on adequate preload to assure adequate cardiac function. If there is damage to the right ventricle, preload reduction from nitrates could result in significant hypotension. If this occurs, resuscitation with intravenous crystalloids and possible vasopressors are needed. Other treatment includes aspirin load with 162 to 325 mg, unfractionated heparin, GP IIb/IIIa antagonist, and additional P2Y12 anti-platelets such as clopidogrel.[8][9][10](A1)
Differential Diagnosis
The differential diagnosis can be quite extensive. Factors that increase the likelihood of cardiac disease include exertional pain, diaphoresis, nausea and vomiting, and radiation of pain to the right arm. Other life-threatening illnesses to consider include pulmonary embolism, aortic dissection, pneumothorax, esophageal rupture, and cardiac tamponade. There may be atypical symptoms, especially in women and older patients, so a high degree of suspicion is required. Since symptoms include nausea, vomiting, epigastric pain, and fatigue it is imperative to consider cardiac causes of these symptoms and not dismiss these symptoms as a gastrointestinal illness.
Prognosis
While inferior wall MIs traditionally have a good prognosis, there are a few factors that may increase mortality. Approximately 40% of inferior wall infarctions also involve the right ventricle. Right ventricular infarctions are very pre-load dependent, and nitrates may precipitate a drop in blood pressure. The addition of right-sided ECGs leads, especially lead V4r, will aid in that diagnosis. If timely treatment does not occur, there is a risk of cardiogenic shock as more myocardial death occurs. Also, because the right coronary artery perfuses the sinoatrial node, heart block and bradycardia may occur. A high degree heart block, defined as a second or third-degree block, is seen in 19% of patients with acute inferior wall MI. The amount of collateral circulation to the AV impacts the rate of heart blocks. If there is a concomitant disease to the other coronary arteries, collateral circulation to the AV node will be reduced, and the likelihood of heart block would be increased.
Complications
- Cardiogenic shock
- Atrioventricular block
- Need for pacing
- Ventricular fibrillation
Postoperative and Rehabilitation Care
- Cardiac rehabilitation
- Lowering blood pressure
- Decreasing cholesterol and blood glucose
- Maintaining a healthy body weight
Deterrence and Patient Education
- Discontinue smoking
- Eat healthy
- Exercise
Pearls and Other Issues
Heart blocks are present in approximately 9% of patients upon presentation, and two-thirds of patients who develop a high-degree heart block during the acute course of their inferior wall MI do so during the first 24 hours. While heart blocks are a main contributor to morbidity and mortality, most high-degree heart blocks are treatable with atropine. It is seldom necessary to use a temporary pacemaker. The damaged myocardium can lead to potentially lethal arrhythmias such as ventricular tachycardia and ventricular fibrillation (see Image. Ischemic Ventricular Tachycardia in a Patient With an Old Inferior Myocardial Infarction). It is necessary to monitor these patients in a monitored setting, usually an intensive care unit, during the acute part of the event. When potentially lethal arrhythmias occur, early defibrillation is essential.
Enhancing Healthcare Team Outcomes
Managing an inferior wall MI requires an interprofessional team of nurses, physicians, a cardiac surgeon, and a cardiologist. These patients are prone to life-threatening complications and hence prevention is the best approach. At discharge, the patients should be educated by the nurse about the potential need for pacing in the future. The dietitian should recommend a low salt, low-fat diet. The patient should be enrolled in a cardiac rehab program. The pharmacist should encourage smoking cessation, compliance with medications and lowering both blood cholesterol and glucose. [11][12][13](Level V)
Outcomes
When the RV is involved in an inferior wall MI it is an independent predictor of major complications and lengthening hospital stay. In addition, ischemia to the conducting pathways are disrupted leading to a high degree of an atrioventricular blockade, that frequently requires pacing. The mortality rates when the RV is involved is often more than 25% compared to patients without Rv involvement. In addition, even after discharge, a significant number of these patients need permanent pacing within 3 years.[14][15][16] [Level 5]
Media
(Click Image to Enlarge)
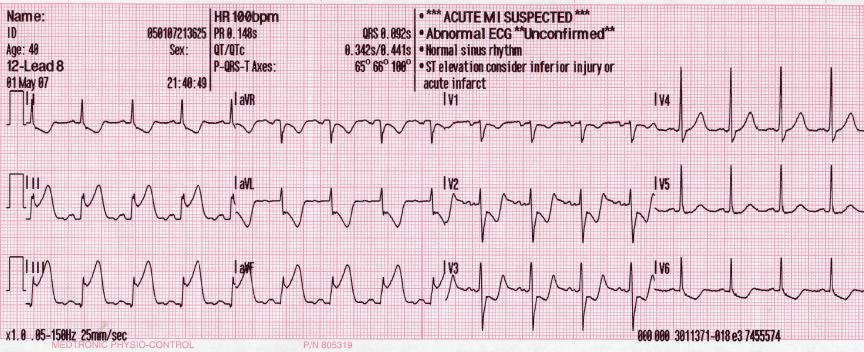
ECG With Pardee Waves Indicating AMI. Pardee waves indicate acute myocardial infarction in the inferior leads II, III, and aVF with reciprocal changes in the anterolateral leads.
Glenlarson, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
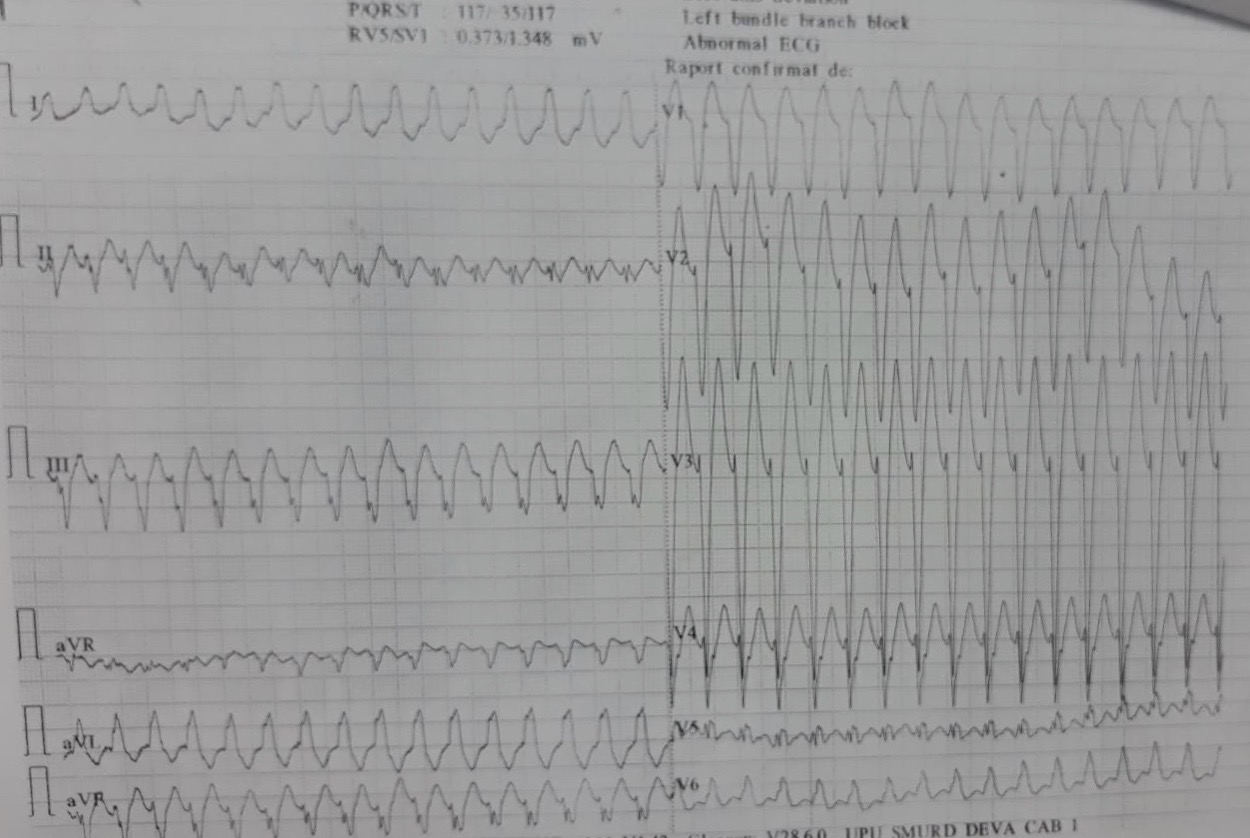
Ischemic Ventricular Tachycardia in a Patient With an Old Inferior Myocardial Infarction.
Contributed by A Negru, MD
References
Aydin F, Turgay Yildirim O, Dagtekin E, Huseyinoglu Aydin A, Aksit E. Acute Inferior Myocardial Infarction Caused by Lightning Strike. Prehospital and disaster medicine. 2018 Dec:33(6):658-659. doi: 10.1017/S1049023X18000705. Epub 2018 Aug 29 [PubMed PMID: 30156178]
Lévy S. Bundle branch blocks and/or hemiblocks complicating acute myocardial ischemia or infarction. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2018 Aug:52(3):287-292. doi: 10.1007/s10840-018-0430-3. Epub 2018 Aug 22 [PubMed PMID: 30136134]
Balasubramanian K, Ramachandran B, Subramanian A, Balamurugesan K. Combined ST Elevation in a Case of Acute Myocardial Infarction: How to Identify the Infarct-related Artery? International journal of applied & basic medical research. 2018 Jul-Sep:8(3):184-186. doi: 10.4103/ijabmr.IJABMR_365_16. Epub [PubMed PMID: 30123751]
Level 3 (low-level) evidenceBouhuijzen LJ, Stoel MG. Inferior acute myocardial infarction with anterior ST-segment elevations. Netherlands heart journal : monthly journal of the Netherlands Society of Cardiology and the Netherlands Heart Foundation. 2018 Oct:26(10):515-516. doi: 10.1007/s12471-018-1147-8. Epub [PubMed PMID: 30105594]
Aguiar Rosa S, Timóteo AT, Ferreira L, Carvalho R, Oliveira M, Cunha P, Viveiros Monteiro A, Portugal G, Almeida Morais L, Daniel P, Cruz Ferreira R. Complete atrioventricular block in acute coronary syndrome: prevalence, characterisation and implication on outcome. European heart journal. Acute cardiovascular care. 2018 Apr:7(3):218-223. doi: 10.1177/2048872617716387. Epub 2017 Jun 15 [PubMed PMID: 28617040]
Roshdy HS, El-Dosouky II, Soliman MH. High-risk inferior myocardial infarction: Can speckle tracking predict proximal right coronary lesions? Clinical cardiology. 2018 Jan:41(1):104-110. doi: 10.1002/clc.22859. Epub 2018 Jan 29 [PubMed PMID: 29377172]
Albulushi A, Giannopoulos A, Kafkas N, Dragasis S, Pavlides G, Chatzizisis YS. Acute right ventricular myocardial infarction. Expert review of cardiovascular therapy. 2018 Jul:16(7):455-464. doi: 10.1080/14779072.2018.1489234. Epub 2018 Jun 27 [PubMed PMID: 29902098]
Albaghdadi A, Teleb M, Porres-Aguilar M, Porres-Munoz M, Marmol-Velez A. The dilemma of refractory hypoxemia after inferior wall myocardial infarction. Proceedings (Baylor University. Medical Center). 2018 Jan:31(1):67-69. doi: 10.1080/08998280.2017.1401347. Epub 2018 Feb 1 [PubMed PMID: 29686558]
Sibbing D, Aradi D, Jacobshagen C, Gross L, Trenk D, Geisler T, Orban M, Hadamitzky M, Merkely B, Kiss RG, Komócsi A, Dézsi CA, Holdt L, Felix SB, Parma R, Klopotowski M, Schwinger RHG, Rieber J, Huber K, Neumann FJ, Koltowski L, Mehilli J, Huczek Z, Massberg S, TROPICAL-ACS Investigators. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): a randomised, open-label, multicentre trial. Lancet (London, England). 2017 Oct 14:390(10104):1747-1757. doi: 10.1016/S0140-6736(17)32155-4. Epub 2017 Aug 28 [PubMed PMID: 28855078]
Level 1 (high-level) evidenceBahramali E, Askari A, Zakeri H, Farjam M, Dehghan A, Zendehdel K. Fasa Registry on Acute Myocardial Infarction (FaRMI): Feasibility Study and Pilot Phase Results. PloS one. 2016:11(12):e0167579. doi: 10.1371/journal.pone.0167579. Epub 2016 Dec 1 [PubMed PMID: 27907128]
Level 2 (mid-level) evidenceUdroiu CA,Cotoban A,Ursulescu A,Siliste C,Vinereanu D, Interdisciplinary Approach in a Complex Case of STEMI. Maedica. 2014 Dec [PubMed PMID: 25705309]
Level 3 (low-level) evidenceMartin D, Bekiaris B, Hansen G. Mobile emergency simulation training for rural health providers. Rural and remote health. 2017 Jul-Sep:17(3):4057. doi: 10.22605/RRH4057. Epub 2017 Oct 17 [PubMed PMID: 29040811]
Kiani F, Hesabi N, Arbabisarjou A. Assessment of Risk Factors in Patients With Myocardial Infarction. Global journal of health science. 2015 May 28:8(1):255-62. doi: 10.5539/gjhs.v8n1p255. Epub 2015 May 28 [PubMed PMID: 26234995]
Li H, Guo W, Dai W, Li L. Short-versus long-term dual antiplatelet therapy after second-generation drug-eluting stent implantation: a systematic review and meta-analysis of randomized controlled trials. Drug design, development and therapy. 2018:12():1815-1825. doi: 10.2147/DDDT.S165435. Epub 2018 Jun 22 [PubMed PMID: 29970956]
Level 1 (high-level) evidenceGinanjar E,Yulianto Y, ST Elevation in Lead aVR and Its Association with Clinical Outcomes. Acta medica Indonesiana. 2017 Oct [PubMed PMID: 29348386]
Level 2 (mid-level) evidenceAltıntaş B, Yaylak B, Ede H, Altındağ R, Baysal E, Bilge Ö, Çiftçi H, Adıyaman MŞ, Karahan MZ, Kaya I, Çevik K. Impact of right ventricular diastolic dysfunction on clinical outcomes in inferior STEMI. Herz. 2019 Apr:44(2):155-160. doi: 10.1007/s00059-017-4631-9. Epub 2017 Oct 9 [PubMed PMID: 28993840]
Level 2 (mid-level) evidence