
Introduction
The International Uveitis Study Group (IUSG) recommended the anatomical classification of uveitis into anterior uveitis, intermediate uveitis, posterior uveitis, and panuveitis.[1] The Standardization of Uveitis Nomenclature (SUN) working group endorsed the same anatomical classification.[2] This anatomical location is based on the actual site of inflammation and is not affected by the presence or absence of structural complications, including cystoid macular edema.[2] The primary location of inflammation in anterior uveitis is the anterior chamber (AC).[2] The anterior uveitis includes three entities, namely iritis, iridocyclitis, and anterior cyclitis.[2] The inflammation of the iris is termed as iritis, and that involving the anterior part of the ciliary body is known as anterior cyclitis.[3]
When both of these are involved, it is called iridocyclitis.[3] Anterior uveitis is the most common form of uveitis.[4] The most common clinical presentation is acute anterior uveitis (AAU).[5] The most common etiologies include HLA-B27 and idiopathic.[5] It is difficult to pinpoint the etiology in some cases, and it may be secondary to the cross-reactivity of microbial antigens in genetically predisposed patients.[6] The etiology of AAU can be varied, ranging from viral infections, bacterial infections, trauma, lens-related inflammation, keratitis, and scleritis. It can exist alone as AAU or in conjuction with intermediate uveitis, posterior uveitis, or panuveitis. Chronic anterior uveitis (CAU) is usually bilateral secondary to an underlying systemic pathology and is less common than AAU.[7] The prognosis is typically good in most idiopathic and HLAB27- related AAU cases, provided management is adequate.[8] Outcomes are more variable in CAU and cases with an underlying ocular or systemic disorder.[5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Most cases of iritis are idiopathic, while 20% are due to blunt trauma.[3]
Nontraumatic iritis often is associated with HLA- B27 systemic diseases, including:
- Juvenile Rheumatoid Arthritis (JRA)[9]
- Ulcerative Colitis[10]
- Reiter syndrome[11]
- Sarcoidosis[12]
- Behcet's disease[13]
- Tubulointerstitial Nephritis and Uveitis (TINU)[14]
- Systemic Lupus Erythematosus (SLE)[15]
- Multiple Sclerosis[16]
- Ankylosing Spondylitis[17]
Infectious Causes
- Tuberculosis[18]
- Chlamydia[19]
- Lyme's disease[20]
- Herpes Simplex[21]
- Toxoplasmosis[22]
- Varicella-Zoster virus (herpes zoster ophthalmicus or shingles)[23]
- Syphilis.[24][5][25].
Other Causes
- Drug-induced[26]
- Masquerade syndromes like lymphoma, leukemia, malignant melanoma[27]
- Juvenile Xanthogranuloma[28]
After Idiopathic variety, HLA-B27 associated uveitic ranks as the second commonest cause of anterior uveitis.[6] It is responsible for 40-70% of anterior uveitis cases in varied geographical regions. It is more common in males than females.[29]
The Various HLA-B27 Associated Conditions with Ocular Involvement are Listed Below[30]
|
S. No |
HLA-B27 associated condition |
Ocular features |
|
1 |
Ankylosing Spondylitis |
Acute anterior uveitis, conjunctivitis, keratitis |
|
2 |
Reiter's disease (reactive arthritis) |
Anterior uveitis, intermediate uveitis, posterior uveitis, keratitis, conjunctivitis, papillitis, scleritis, cataract |
|
3 |
Juvenile spondyloarthropathy |
Anterior uveitis |
|
4 |
Psoriatic arthritis |
Anterior uveitis, keratitis, dry eyes, conjunctivitis, panuveitis, scleritis, cataract, papillitis, pigmentary retinopathy |
|
5 |
Inflammatory bowel disease |
Conjunctivitis, episcleritis, scleritis anterior uveitis, cataract, vitritis retinal vasculitis, peripheral ulcerative keratitis
|
|
6 |
Undifferentiated spondyloarthropathies |
Acute anterior uveitis or chronic anterior uveitis, vitritis, retinal vasculitis
|
Rodriguez et al., from their large-scale analysis from a tertiary eye care center, listed the prevalence of various etiologies in all the anatomic forms of uveitis.[31]
The most common conditions were:
- Idiopathic
- Seronegative spondyloarthropathies
- Sarcoidosis
- JRA
- SLE
- Behcet's
- HIV
Ankylosing spondylitis, Inflammatory bowel disease, psoriatic arthritis, and Reiter's syndrome are grouped under seronegative spondyloarthropathies.[32] As per Rodriguez et al., the most common form was anterior uveitis, with the most common etiology being idiopathic followed by seronegative arthropathy, JRA, herpes, sarcoidosis, SLE, and rheumatoid arthritis. The next was posterior uveitis, with common etiologies being toxoplasmosis, idiopathic, CMV, SLE, and sarcoidosis.[33]
Epidemiology
Anterior uveitis is the most common form of uveitis (occurring every 12 per 100 000 cases).[5] It predominantly occurs in young and middle-aged people. In western countries, 50% to 70% of all uveitis cases are classified as anterior uveitis. Uveitis is responsible for 10% of legal blindness in the USA, and it accounts for approximately 30,000 new patients with blindness every year.[34] The study from northern California on the epidemiology of uveitis revealed an incidence of 52.4 per 100000 persons per year and a prevalence of 115.3 per 100000 persons.[35]
The maximum incidence and prevalence were seen in elderly patients above 65 years and lowest in the pediatric age group. Women had a higher prevalence than men.[35] The study from Affairs Medical Centre, Northwest Pacific, reported an incidence of 25.6 cases per 100000 persons and a prevalence of 69 per 100000 persons.[36] The study in the elderly population from the care survey medicare cohort revealed an incidence of uveitis ranging from 302-424 per 100000 persons per year and an average of 340.9 per 100000.[37] The mean incidence of uveitis was 243.6 per 100000. The reported incidence of posterior uveitis was 76.6 per 100000, and panuveitis incidence was 41.7 per 100000.[37]
Pathophysiology
Eye pain is thought to be due to irritation of the ciliary nerves and ciliary muscle spasms. Photophobia is caused by irritation of the trigeminal nerve from the ciliary spasm.[38] Increased permeability of blood vessels in the anterior chamber allows proteinaceous transudate ("flare") and WBCs ("cells"), the characteristic 'flare and cells' seen with the slit lamp.[39] In traumatic uveitis, there can be microbial contamination and retention of necrotic debris at the site of trauma, resulting from a florid inflammatory response in the anterior segment of the eye. In infectious uveitis, the pathophysiological mechanism is immune-mediated destruction of foreign antigens that may cause damage to the uveal tissue, vessels, and cells.[40] There is immune complex deposition inside the uveal tract in autoimmune uveitic conditions, a form of hypersensitivity reaction.[41][39]
Uveal inflammation behaves similarly to inflammation in other body tissues, i.e., having a vascular and cellular response. But due to excessive vascularity and looseness of uveal tissue, there is heightened vascular response. Pathophysiologically, the uveal inflammation is subdivided into purulent (suppurative) and nonpurulent (non-suppurative) types.[41]
Wood’s Classification of Non-Suppurative Inflammation[42]
- Non-granulomatous
- Granulomatous
Suppurative Uveitis
It results from exogenous infections from pyogenic microorganisms. It is a part of the spectrum of endophthalmitis or panophthalmitis and is caused by Staphylococci, Streptococci, Pseudomonas, Pneumococcus. In suppurative inflammation, there occur outpouring of purulent exudates and an increase in polymorphonuclear cells. The uveal tissue increases in size, becomes thickened, and demonstrates necrosis and pus formation in the cavities.[43]
Non-granulomatous Uveitis
In non-granulomatous (NG) uveitis, diffuse inflammation is characterized by dilatation and increase in permeability of vasculature, blood-aqueous barrier breakdown, increase in exudates, increased infiltration by lymphocytes, plasma cells and, macrophages.[44] The iris becomes edematous, muddy in color, and waterlogging occurs. As a result, there occur loss of crypts and furrows. Further, there is iridoplegia; the pupil becomes small and sluggish due to the engorgement of iris vessels. The infiltration of exudates and lymphocytes manifests as cells and flare in the anterior chamber and KPs at the back of endothelium.[45] The exudates can also be seen in the posterior segment and manifest as posterior synechiae, where the posterior iris adheres to the anterior lens capsule. Sometimes exudates may occupy the ciliary body and result in a cyclitic membrane. In the healing phase, atrophy of the iris is evident, and there may be areas of necrosis. Further destructive changes manifest as necrosis, gliotic and fibrotic areas, resulting in adhesions, scar formation, and eventual destruction of uveal tissue.[46]
Granulomatous Uveitis
In granulomatous uveitis, there is increased infiltration by lymphocytes, plasma cells, epithelioid cells, and giant cells resulting in nodule formation. The nodules may be seen at the pupillary border, such as Koeppe's nodules) and nodules may be seen at the back of the cornea as mutton fat KP's. This may be followed by necrosis, gliotic and fibrotic areas which result in adhesions, scar formation, and eventual destruction of uveal tissue.[5]
Histopathology
The histopathological findings in uveitis vary with etiology.
- Lens induced uveitis - Macrophages, acute and chronic inflammatory cells[47]
- Parasitic uveitis - Eosinophils, polymorphonuclear neutrophils, and parasites occasionally[48]
- Masquerade syndrome - Cellular infiltrates in retinoblastoma, leukemia, etc. and malignant cells[49]
- Phacoanaphylactic uveitis - Epithelioid cells, polymorphonuclear neutrophils, and giant cells[50]
- Uveitis- Predominant lymphocytic infiltrate[51]
- Late-onset Endophthalmitis - Propionibacterium on gram stain, culture plating, or PCR[52]
- Endophthalmitis - Acute and chronic inflammatory cell infiltrate along with offending microorganism[53]
- Lymphomas (large cell) - Cells with pleomorphism, oval or circular nuclei, and scanty cytoplasm. There is an occasional predominance of micronuclei[54]
History and Physical
Classification
The anatomical classification of uveitis is proposed by the Standardization of Uveitis Nomenclature (SUN) Working Group.
Anatomical
- Anterior- Involving the iris and ciliary body[55]
- Intermediate- Involving vitreous and pars plana[56]
- Posterior- Involving retina and choroid[57]
- Panuveitis- Anterior, intermediate and posterior[2]
The Etiological Classification of Uveitis is Proposed by the International Uveitis Study Group (IUSG)
- Infectious- Viral, bacterial, parasitic, Lyme disease, etc. [58]
- Non-infectious- Idiopathic or associated with systemic diseases[45]
- Masquerade- Neoplastic and non-neoplastic[59]
SUN Working Group Proposed the Classification Based on the Timing of Inflammation
- Timing of onset- Insidious or sudden[60]
- Duration of inflammation- Limited (less than or equal to 3 months ) or persistent[61]
Clinical Activity
- Acute- Insidious or sudden
- Chronic- Persistent with relapse within three months after stopping the treatment
- Recurrent- Repeated episodes with an in-between inactive period
- Remission- No active episode for three months or more[3]
Anterior Uveitis
Acute
- Pain, redness, photophobia, tearing, and decreased vision with pain developing over a few hours or days except in trauma cases.[3]
Chronic
- Blurred vision, mild redness, and little pain or photophobia except during an acute episode.[62]
Slit Lamp Evaluation in Uveitis Patients
Circumciliary congestion or circumcorneal congestion (injection) gives the appearance of a purple hue due to involvement in conjunctival plexus and deeper vessels. It's a sign of AAU and may not be seen in CAU.
Pupillary miosis is due to iridoplegia and sphincter spasms, which lead to the formation of posterior synechiae.
Anterior chamber cells are estimated by SUN grading with the help of a 1x1 mm slit beam under adequate lighting and magnification. The cells and flare indicate inflammatory activity inside the anterior chamber. The cells and flare should be assessed before pupillary dilatation as dilatation invites pigment shedding into the aqueous. The cells can also be observed in the vitreous phase.[63]
SUN Grading of Cells in Anterior Chamber (1 mm x 1 mm Slit Beam)
|
S. No |
Grade |
Cells in the field |
|
1 |
0 |
< 1 |
|
2 |
0.5+ |
1-5 |
|
3 |
1+ |
6-15 |
|
4 |
2+ |
16-25 |
|
5 |
3+ |
26-50 |
|
6 |
4+ |
>50 |
An anterior chamber or aqueous flare is the turbid appearance of the aqueous in the anterior chamber due to the proteins secondary to the breakdown of the blood-aqueous barrier. In children with JIA-associated CAU, flare is taken as the level of inflammatory activity more than cells and indicates complications in the long term. Flare is graded on a slit lamp by assessing the iris and lens details. Laser flare photometry is another modality for objective grading.[63]
SUN Classification of Flare in the Anterior Chamber
|
S. No |
Grade |
Description |
|
1 |
0 |
None |
|
2 |
1+ |
Faint |
|
3 |
2+ |
Moderate- Clear iris and lens details |
|
4 |
3+ |
Marked- Hazy iris and lens details |
|
5 |
4+ |
Intense- Plastic or fibrin aqueous |
Hypopyon is the presence of whitish purulent exudative material in the anterior chamber. It is composed of inflammatory material, and form appears as a horizontal level that is gravity-dependent. It is common in HLA B27 associated uveitis. The hypopyon is immobile due to high fibrin content, making it difficult to absorb. Behcet's disease patients have a characteristically mobile hypopyon due to low fibrin content.[64] Hypopyon is inflammatory cells deposited in the anterior chamber and is composed of leucocytes.[64] It is measured with the help of a slit lamp micrometer. The shape, color, and consistency of hypopyon are indicators of etiology. It can be mobile or fixed. To test the mobility of hypopyon, the patient is asked to lie down supine for 10 minutes. Then after 10 minutes, the level of hypopyon is tested. In the case of fixed hypopyon, there is no movement, but in the case of mobile hypopyon, the level or height is changed.[65]
Various Types of Hypopyon in Different Condition
|
S. No |
Hypopyon characteristic |
Diagnosis/etiology |
|
1 |
Sterile |
Behcet's disease |
|
2 |
Mobile |
Bacterial keratitis |
|
3 |
Fixed/ Immobile |
Fungal keratitis |
|
4 |
Central |
Pneumococcal keratitis |
|
5 |
Haemorrhagic |
Pneumococcus, herpetic keratitis, trauma |
|
6 |
Other causes |
Endophthalmitis, ranibizumab, JIA, histiocytosis, Leukemia, laser iridotomy, lens-induced, HLA-B27 uveitis, leptospirosis, phacolysis |
Keratic precipitates (KPs) are inflammatory cellular deposits at the back of the cornea (endothelium). The cellular aggregates include lymphocytes, plasma cells, and macrophages. Epithelial cells and giant cells are also common in KPs. The KPs are seen inferior one-third of the cornea in a triangular pattern with the apex pointing upwards (Arlt's triangle). The KPs are distributed in Arlt's triangle due to aqueous convection currents and the effect of gravity. In contrast, they can be seen diffusely distributed in Fuch's heterochromic iridocyclitis (FHIC) and viral uveitis (stellate KPs). The morphological appearance of KPs indicates the type of uveitis, like small KPs in non-granulomatous (NG) uveitis and large in granulomatous uveitis. Large glistening greasy KPs are seen as granulomatous uveitis and are called mutton fat KPs. Once the acute episode resolves, KP usually disappears. Pigmented KPs can be observed (NG variety). The granulomatous KPs may also become pigmented and are classically described as the ground-glass appearance of KPs. Sometime before the appearance of KP's diffuse pigment deposition is seen at the back of the cornea called endothelial dusting.[66]
|
S. No |
Characteristic |
Type of KP |
|
|
Fresh |
Old |
||
|
1 |
Colour |
White |
Pigmented |
|
2 |
Shape |
Circular/ Round |
Flat |
|
3 |
Hydration |
Fully hydrated |
Dehydrated |
|
4 |
Edges |
Smooth |
Crenated |
The fibrinous membrane is a common entity in AAU and is seen in the anterior chamber.
Iris atrophy is another clinical sign of uveitic sequelae. Diffuse iris atrophy is observed in FHIC, and a patchy or sectoral pattern appears in herpetic uveitis. Sectoral iris atrophy can be seen more in herpes zoster uveitis, although both sectoral and diffuse patterns can be observed in both herpes simplex and zoster uveitis.[67]
Iris nodules are observable in both NG and the granulomatous variety.
- Koeppe's nodules - These are present at the pupillary margin or the location of posterior synechiae. These are ectodermal nodules usually white and may be pigmented. They can be seen in granulomatous as well as non granulomatous uveitis.
- Busacca's nodules - These involve the iris stroma and are predominantly seen in granulomatous variety.
- Roseolae - These are yellow nodules are seen in Syphilis, resulting from dilatation of iris vessels.
- Berlin nodules - These are seen in angles in cases with sarcoidosis.
- Iris pearls - These are observed in lepromatous uveitis.
- Russell bodies - These, also called iris crystals, are seen in FHIC and rare cases of chronic uveitis. They are thought to result from immunoglobin deposits.[68]
Posterior synechiae (PS) are another essential clinical finding in uveitic cases. They result from adhesion of the pupil margin to the anterior capsule secondary to uncontrolled inflammation. PS can be seen at the site of the Koeppe nodule. All cases should be instilled with a cycloplegic agent like atropine or homatropine to prevent PS formation.[69]
Types of Posterior Synechiae
- Segmental - They are adhesions of the iris at some points over the lens
- Annular (ring) - They are 360-degree adhesion of the iris to the anterior lens capsule
- Total- These are plastered posterior surface of iris to the lens
- Broad- They are seen in tubercular uveitis
- Filiform-They are seen in non-tubercular uveitis
- Seculusio pupillae- When synechiae cover the 360-degree pupil and prevent migration of aqueous from posterior to the anterior chamber
- Occlusio pupillae- Formation of membrane over the lens surface
- Festooned pupil- When synechiae are localized, and on dilatation, the pupil takes an irregular shape
Heterochromic iris is the difference in the color of the iris between the two eyes. Heterochromia is seen in FHIC.[70]
Neovascularization of the iris (rubeosis iris) can result from chronic inflammation. The vascularization seems to be less as compared to posterior segment pathologies. FHIC shows abnormal iris vessels but does not result in synechial angle closure. Iris's new vessels are also seen in posterior uveitis. Sometimes it becomes difficult to differentiate between new and normal iris vessels (pseudo-rubeosis of the iris). The differentiating point is new vessels show irregular branching in contrast to normal vessels, which are radial. Fluorescein angiography is used to assess the leakage from new vessels.[71]
Fundus evaluation is mandatory in each case to rule out masquerades like malignant melanoma, retinal detachment, cystoid macular edema, and other posterior segment complications.
Difference between Granulomatous and Non-Granulomatous Uveitis
|
S. No |
Characteristic |
Type of Uveitis |
|
|
Granulomatous |
Non-Granulomatous |
||
|
1. |
Time of onset |
Insidious |
Acute |
|
2 |
Pain severity |
Mild |
Marked |
|
3 |
Photophobia |
Mild |
Marked |
|
4 |
Congestion |
Minimal |
Marked |
|
5 |
Keratic precipitates |
Large- Mutton fat |
Small |
|
6 |
Anterior chamber flare |
Mild |
Marked |
|
7 |
Iris nodules |
Present |
Absent |
|
8 |
Posterior synechiae |
Thick and broad |
Thin and flat |
|
9 |
Posterior segment |
Patchy involvement |
Diffuse involvement |
Difference between Acute and Chronic Uveitis
|
S. No |
Characteristic |
Type of Uveitis |
|
|
Acute |
Chronic |
||
|
1. |
Time of onset |
Sudden |
Acute |
|
2 |
Symptoms |
Pain, redness, photophobia |
Asymptomatic, reduced vision and floaters |
|
3 |
Start date |
Definite |
Not definitive |
|
4 |
Resolution |
Self-resolving mostly |
Long duration |
Evaluation
Since iritis involves anterior uveitis per se, the evaluation and treatment are focussed on anterior uveitis only. Further laboratory tests or imaging may be required if systemic involvement or infectious disease is suspected to be the underlying cause.[72][73][74][75] In most uveitic cases, the investigations are normal, and no underlying etiology can be discerned. Tailored made investigations are needed in each patient to pinpoint the etiology based on the clinical signs. In some cases, the etiology is evident on the clinical examination, like uveitis in the case of endophthalmitis post-surgery. Most patients also need systemic evaluation and careful review by an internist.[76]
Visual Acuity
Visual acuity depends on the extent of inflammatory activity and associated complications. It is generally minimally reduced in AAU. Snellen's uncorrected and best-corrected visual acuity should be documented in each patient. The improvement in visual acuity is also an indicator of resolution of uveitis and reduction in inflammation.[77]
Intraocular Pressure
Intraocular pressure (IOP) can be raised in uveitic cases. The reduction in IOP is due to ciliary shutdown or reduction in aqueous secretion from the ciliary epithelium. The raised IOP can be due to angle closure, trabeculitis, steroid-induced, and other causes. The IOP can be measured by noncontact tonometry, ICARE tonometer, or Goldman applanation tonometer and should be documented on each visit.[78]
Cases of Uveitis where Investigations are Not Mandatory
- The first episode of unilateral mild NG AAU with no previous ocular or systemic history
- Classical clinical signs of a specific etiology for which investigation will not be helpful like FHIC
- When the systemic signs and symptoms are indicative of a particular etiology associated with uveitis like sarcoidosis, tuberculosis, multiple sclerosis, etc. [79]
Cases of Uveitis where Investigations Will be Helpful
- Bilateral cases of AAU
- Severe cases AAU
- Recurrent cases of AAU
- Chronic A.U. resistance to treatment
- Granulomatous AU
- AAU associated with I.U. or posterior uveitis or panuveitis cases
- Ocular and systemic signs indication underlying pathology[3]
Further laboratory tests or imaging may be required if systemic involvement or infectious disease is suspected to be the underlying cause.[72][73][74][75]
Imaging
Chest radiography may be considered if sarcoidosis or tuberculosis is the underlying cause of uveitis. In granulomatous uveitis cases, a high index of suspicion should be kept to rule out these treatable systemic conditions as well as syphilis. X-ray of the sacroiliac joint reveals bamboo spine and sacroiliitis in cases with ankylosing spondylitis and other seronegative spondyloarthropathies.[80]
Ocular Imaging
B Scan Ultrasound
A B scan should be performed in the fundus that is not visualized due to small pupil, anterior chamber reaction, fibrinous membrane, or vitreous haze.[81]
Optical Coherence Tomography
It's a handy tool to rule out cystoid macular edema and epiretinal membrane and look for cells and flare.[82]
Fundus Fluorescein Angiography
This is an essential investigation in chronic uveitis cases to rule out posterior segment pathology like vasculitis macular ischemia delineate capillary non-perfusion areas and white dot syndrome spectrum.[83]
Fundus Autofluorescence
Fundus autofluorescence (FAF) is essential in posterior segment pathologies to rule out white dot syndromes and severe inflammatory conditions.
Indocyanine Green Angiography
Indocyanine green angiography (ICGA) is needed in cases with uveitis-associated choroidal pathology.[84]
Ultrasound Biomicroscopy
Ultrasound biomicroscopy (UBM) is helpful to rule out hypotony (ciliary shutdown), choroidal effusion, cyclodialysis cleft, and cyclitic membrane.[85]
Laboratory Workup
Laboratory workup is usually not necessary. In mild unilateral non-granulomatous uveitis with trauma or no evidence of systemic disease, laboratory studies are unlikely to be helpful. If there is the presence of bilateral granulomatous or recurrent uveitis, a workup is indicated.[3] Tests to consider include:
Human Leucocyte Antigen tissue typing (HLA-B27)
- HLA- B27 testing should be done in any patient with recurrent A.U. or chronic N.G. A.U. The various HLA types and their associations are detailed below.
- HLA B27- Recurrent AAU
- HLA-B51 and HLA B5- Behcet's disease
- HLA-A29- Birdshot retinochoroiditis
- HLA-DR4- Sympathetic Ophthalmia and Vogt-Koyanagi-Harada disease
- HLA-B7 and HLA-DR- Presumed Ocular Histoplasmosis Syndrome[86]
Syphilis Serology
The various test implicated in syphilis is treponemal antibody tests such as ELISA- enzyme-linked immunosorbent assay, which has high specificity and sensitivity but takes approximately three months to show positivity. Anti-cardiolipin antibody tests (non-specific) like venereal research laboratory test (VDRL) and rapid plasma regain (RPR) demonstrate positive results in the acute phase of the disease and help to monitor the disease and treatment. The patients having features of ocular syphilis should be referred to an internist to rule out sexually transmitted syphilis.[87]
Angiotensin-Converting Enzyme
This is a non-specific test to rule out the cause of N.G. A.U. such as sarcoidosis, tuberculosis, and Hansen disease. Serum levels of ACE are elevated in approximately 80% of patients with sarcoidosis but come down to normal levels during remission.[88]
Serum Lysozyme Assay
Lysozyme, an enzyme, is found in neutrophils and tear secretion. It has antibacterial properties and can cause bacterial cell wall breakdown. This test has comparatively less sensitivity and specificity than serum ACE in diagnosing sarcoidosis, but the combined test may prove more beneficial.[76]
Complete Blood Count
A raised leucocyte count is indicative of infective may be a hematological malignancy. Eosinophils are raised in parasitic causes of uveitis.[3]
Inflammatory Markers
C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and acute phase reactants may be elevated in systemic inflammatory disorders.[89]
Lyme Disease Serology
Disease-specific serology is essential in endemic areas, including serology for other infections like brucellosis and leptospirosis.[90]
Antinuclear Antibody
Antinuclear antibody (ANA) is the most important marker for juvenile idiopathic arthritis in children. ANA positivity is an indicator of CAU.[91]
Antineutrophil Cytoplasmic Antibody
Antineutrophil cytoplasmic antibody (ANCA) is valuable for anterior uveitis associated with scleritis. It is a valuable marker for Wegner granulomatosis (c-ANCA) and Polyarteritis Nodosa (PAN) {p-ANCA}.[92]
Interferon-Gamma Release Assay
Interferon-gamma Release Assay such as QuantiFERON-TB Gold for diagnosis of tuberculosis.[93]
HIV Serology
HIV tridot test for suspected patients with immunosuppression.[94]
Anterior Chamber Tap
An anterior chamber aqueous tap can be performed, and a sample can be sent for a polymerase chain reaction in cases of suspected viral uveitis like herpes, varicella, and rubella. PCR will also distinguish Propionibacterium acne infection in chronic uveitis in pseudophakic eyes.[95]
Iris Biopsy
Iris biopsy is another critical investigation but is rarely done nowadays.[96]
Vitreous Biopsy
In the case of associated posterior segment involvement, especially in the case of suspected endophthalmitis.[97]
Conjunctival Biopsy
In case of suspected granulomas or infiltrative lesions, a conjunctival biopsy is indicated.[98]
Physician Referral
To rule out systemic pathologies, timely referral to an internist is essential to pinpoint the etiology—for example, HRCT in pulmonary tuberculosis and MRI in cases of multiple sclerosis.
Treatment / Management
Treatment is primarily aimed at reducing inflammation and pain and preventing complications. First-line treatment involves topical cycloplegics (dilate the pupil, prevent the ciliary body and pupillary spasm) and topical steroids (decrease inflammation). The patient should be referred to an ophthalmologist within 24 to 48 hours. The review frequency is decided based on the clinical presentation and degree of inflammatory activity. Those with severe inflammation need review within a day or two, and those with mild AAU may be seen after a week or so.
- Sustained-release corticosteroid vitreous implants (fluocinolone acetonide, dexamethasone) are available to treat inflammation-induced cases of panuveitis, intermediate uveitis, and posterior uveitis.
- Corticosteroids should be initiated only in conjunction with the approval of an ophthalmologist because uveitis is a diagnosis of exclusion.
- Steroids can have adverse effects, such as causing intraocular pressure, cataract formation, steroid-induced glaucoma, and the development of herpes keratitis.
- Potassium-sparing drugs should be used when chronic steroid use is required to control inflammation. Approximately half of the patients with uveitis need treatment beyond corticosteroid treatment to prevent vision loss.[5]
Topical Steroids
Corticosteroids decrease inflammation. Treatment should only be initiated after consultation with an ophthalmologist. Prednisolone 1% or dexamethasone 0.1% are potent steroids and are the first treatment choice for uveitis. They work by decreasing inflammation by reversing increased capillary permeability and suppressing the migration of polymorphonuclear leukocytes.
The other drugs used for iritis management are difluprednate 0.05% (lower frequency), prednisolone 0.5%, loteprednol etabonate 0.5% and 0.2%, betamethasone, fluorometholone, and rimexolone (moderate to low potency). Steroid regimen can be altered based on the response and intraocular pressure elevation. Betamethasone ointment can be used at bedtime. The steroid regimen varies according to the degree of inflammation, starting from an hourly regimen for three days to every two hours for three days, then 6/5/4/3/2/1 times one week each. The treatment is usually stopped after 6 to 8 weeks. Timely and regular follow-up is mandated in each case. In CAU cases, the target is the full resolution of inflammation. Low-grade persistent inflammation can result in a higher incidence of complications which can be reduced with regular and timely steroids instillation. Steroids can act as a bilateral sword, resulting in elevated IOP (steroid response), cataract, glaucoma, keratitis, and corneal melt.[99]
Cycloplegics
Cycloplegics block nerve impulses to the ciliary muscles and pupillary sphincter to decrease photophobia and pain. They are implicated in AAU and CAU exacerbations. These help to break down the already formed posterior synechiae prevent the formation of new synechiae.
Homatropine
- Induces cycloplegia in 30 to 90 minutes.
- Induces mydriasis in 10 to 30 minutes.
- Effects last 10 to 48 hours for cycloplegia and 6 to 96 hours for mydriasis, but the duration may be less if severe anterior chamber reaction.
- Homatropine is an agent of choice for uveitis.
Cyclopentolate 0.5% to 2%
- Induces cycloplegia in 25 to 75 minutes.
- Induces mydriasis in 30 to 60 minutes.
- Effects usually last one day.
- Less attractive for treating uveitis than homatropine.
The other cycloplegics available are atropine which has a long duration of action of 7-10 days. In AAU, 2.5% or 10% phenylephrine can also break posterior synechiae. Bedtime administration of the drug should be promoted to avoid difficulties with accommodation during the daytime. Atropine has been known to cause toxic side effects like seizures amblyopia in children, and extra precautions should be taken while administering drugs to children.[3]
Mydricaine
Mydricaine is a preparation of 0.3 ml containing 0.12 mg adrenaline, 1mg atropine, and 6 mg procaine. Adrenaline and atropine break the posterior synechiae and procaine to improve comfort. The drug combination is given as a subconjunctival injection. Another installation method is cotton pledget dipped in Mydricaine and kept for 5 minutes in the superior and inferior fornices for 5 minutes. Mydricaine number 1 is used pediatric version, and mydricaine number 2 is used in adults. The side effect reported with Mydricaine is transient sinus tachycardia.[100](B3)
Tissue Plasminogen Activator
In severe fibrinous anterior uveitis cases, 12.5 to 25 ug of tissue plasminogen activator is injected in the anterior chamber in 0.1 ml solution with a 30 G needle under topical anesthesia. This will dissolve the fibrin membrane and break down the posterior synechiae.[101](B3)
Subconjunctival Steroids
Betamethasone sodium phosphate and acetate combination can be given for severe A.U. and patients with poor compliance subconjunctivally.[102]
Subtenons Injection of Steroids
Posterior sub tenons injection of methylprednisolone or triamcinolone acetonide can be given in cases with aggressive posterior segment inflammation and in patients with anterior uveitis having cystoid macular edema a complication. They can be instilled as an OPD procedure or given during the surgery to supplement the systemic steroids. The onset of action is four weeks, and the maximum duration is around three months. Varied complications have been reported like secondary glaucoma, globe perforation, subconjunctival hemorrhage, cataract, retrobulbar hemorrhage, and ptosis.[103](B2)
Intravitreal Steroids
Intravitreal triamcinolone acetonide (4 mg in 0.1 ml) is also implicated in cystoid macular edema after anterior uveitis, which is not responding to other therapy. The complications are similar to sub tenons administration except pseudohypopyon, exclusive to intravitreal steroids.[104](B3)
Systemic Steroids
When the inflammation is severe and response to topical treatment is inadequate, oral prednisolone is indicated. They are given in tapering doses, and each case should monitor side effects.[102]
Non- Steroidal Anti- Inflammatory Drugs (NSAIDs)
Naproxen and tolmetin are implicated in CAU cases and can be used for the long term under physician observation.[99]
Antimetabolites
Methotrexate is implicated in CAU secondary to juvenile idiopathic arthritic in children when steroids fail to control the inflammation.[105]
Tumor Necrosis Factor Blockers
Infliximab or adalimumab may be used as second-line treatment for patients with vision-threatening chronic uveitis caused by seronegative spondyloarthropathy.[106]
Differential Diagnosis
The differential diagnoses include
- Acute angle-closure glaucoma
- Conjunctivitis
- Subconjunctival hemorrhage
- Trauma
- Episcleritis
- Scleritis
- Dry eyes
- Pingueculitis
- Inflammed pterygium
- Corneal abrasion
- Corneal ulcer
- HSV keratitis
- Intraocular foreign body
- Scleritis
- Ulcerative keratitis
- Ultraviolet keratitis
Prognosis
The prognosis is good with appropriate treatment. To have the best prognosis, follow-up care with an ophthalmologist within 24 hours is imperative. Monitoring should include repeat slit-lamp and intraocular pressure checks every few days. When the condition is stable, monitoring can be every 1 to 6 months. If not diagnosed and treated on time and neglected cases usually develop complications like cataract, glaucoma, retinal detachment, and macular edema, and the prognosis is guarded in these cases.[107]
Complications
- Corneal scar (keratouveitis)
- Band shaped keratopathy
- Hyphema
- Non-resolving hypopyon
- Iris atrophy
- Posterior synechiae
- Cataract (Inflammation related, steroid-induced)
- Secondary glaucoma (pupillary block, inflammation, or topical corticosteroid)
- Occlusio pupillae
- Festooned pupil
- Seclusio pupillae
- Cystoid macular edema
- Optic neuropathy
- Optic disc neovascularization
- Macular scar
- Hypotony
- Vitreous hemorrhage (associated intermediate, posterior, or panuveitis)
- Retinal detachment
- Endophthalmitis[53]
- Panophthalmitis
- Permanent blindness
- Strabismus[108]
Postoperative and Rehabilitation Care
In cases undergoing cataract surgery, postoperative care is required for complicated cataract of filtration surgery for non-resolving glaucoma or progressive glaucomatous changes. For patients undergoing cataract surgery, the usual regimen is topical steroids (1% prednisolone or 0.1% dexamethasone) or steroids and antibiotic combination (0.1% dexamethasone + 0.5% gatifloxacin) 6/5/4/3/2/1 times for one week each along with a cycloplegic like topical 5% homatropine or 1% atropine two times per day for 2 to 3 weeks.[3]
The patients should be regularly and closely followed to prevent any complications. In patients undergoing filtration surgery, the usual regimen is topical steroids (prednisolone 1% or dexamethasone 0.1%) or steroids and antibiotic combination (dexamethasone 0.1% + gatifloxacin 0.5%) 8/7/6/5/4/3/2/1 times for one week each along with a cycloplegic like topical homatropine 5% or atropine 1% two times per day for 2 to 3 weeks. These patients should be closely followed up to rule out complications like macular snuff out, hypotony, uncontrolled glaucoma and check for the normal functioning bleb.[109] The patients requiring retinal detachment repair are also treated post-operatively with the same regimen as glaucoma patients. Two to three months later, these patients will require silicon oil removal. All these patients should also be closely followed up to rule out re-detachment and other complications of retinal surgery.[110]
Consultations
Any patient presenting to the clinic with pain, redness, and photophobia should be meticulously evaluated by an Ophthalmologist with suspicion of iritis. In the case of keratouveitis, the patient should be referred to a cornea specialist for higher opinion and management to rule out infective and autoimmune keratitis. Non-resolving iritis, endophthalmitis, or cases with diagnostic dilemmas must be evaluated by a retina and uvea specialist for expert opinion and further management. The patient with underlying systemic pathology leading to iritis and uveitis should be referred timely to an internist to pinpoint the etiology and targeted systemic treatment. Iritis with trabeculitis, angle-closure, or open-angle glaucoma should be managed with a glaucoma specialist. Patients with complicated cataracts requiring surgical intervention should be ideally operated on by a cataract and IOL surgeon for an excellent visual outcome.[3]
Deterrence and Patient Education
Patients with iritis should be explained about the ocular pathology the importance of regular and timely treatment and follow-up. The patient should be educated about the underlying systemic pathology associated with iritis and the critical role of the internist in treating the condition. The patients should also be explained about the complications related to iritis and the side effects of irregular and long-term use of steroids.
Pearls and Other Issues
Anterior uveitis can present as an isolated entity or associated intermediate and posterior uveitis. There can be a spillover of anterior segment inflammation into the vitreous or posterior segment. All patients should undergo extensive evaluation to pinpoint the etiology. The internists have a key role to play in the diagnosis and management of uveitic cases. If untreated, complications can include decreased visual acuity and/or blindness, glaucoma, cataracts, and irregular pupil.[5]
Enhancing Healthcare Team Outcomes
The management of a patient with iritis is interprofessional. Whenever a patient presents with eye pain, tearing, photophobia, vision loss, and red-eye in the absence of trauma, the patient must be referred to an ophthalmologist as soon as possible. The treatment of iritis primarily aims to reduce inflammation and pain and prevent complications. First-line treatment involves topical cycloplegics (dilate the pupil, prevent the ciliary body and pupillary spasm) and topical steroids (decrease inflammation). Depending on the cause, most patients respond well to treatment and retain full vision. However, at least 10 to 30% of patients may need treatment beyond steroids to prevent vision loss.[24][111] [Level 5] Once discharged, the patient may follow up with the ophthalmic nurse, primary care provider, or ophthalmologist.[5]
Media
(Click Image to Enlarge)
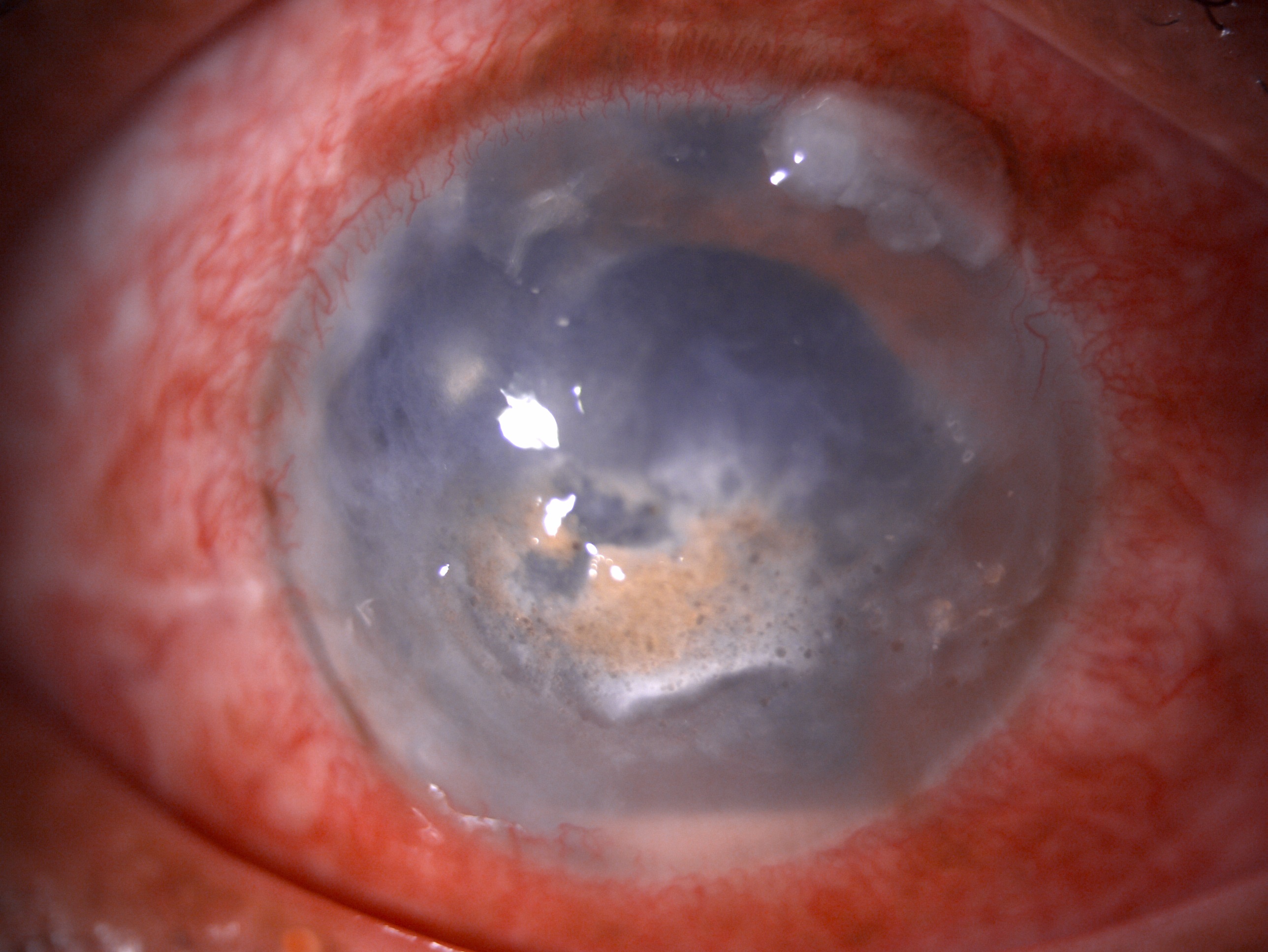
Slit-lamp image of the patient of recurrent anterior uveitis depicting circumciliary congestion, corneal scarring, central band shaped keratopathy, hypopyon in anterior chamber and pseudophakia Contributed by Dr. Bharat Gurnani, MBBS, DNB, FCRS, FICO, MRCS Ed, MNAMS
(Click Image to Enlarge)
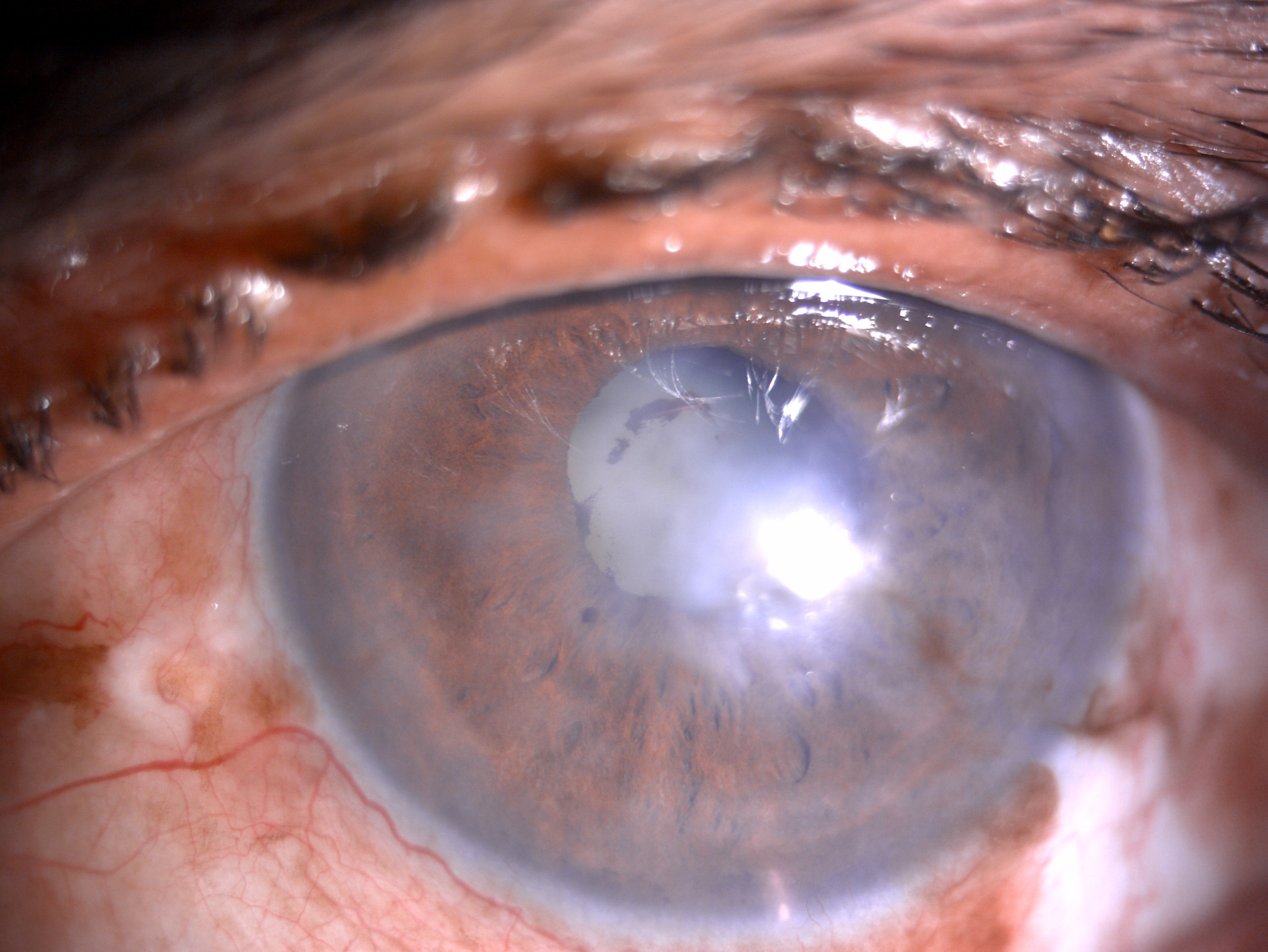
Slit- lamp image of the patient with recurrent uveitis depicting mild circumciliary congestion, nebular corneal scarring, few areas of iris atrophy along with a complicated cataract Contributed by Dr. Bharat Gurnani, MBBS, DNB, FCRS, FICO, MRCS Ed, MNAMS
References
Bloch-Michel E, Nussenblatt RB. International Uveitis Study Group recommendations for the evaluation of intraocular inflammatory disease. American journal of ophthalmology. 1987 Feb 15:103(2):234-5 [PubMed PMID: 3812627]
Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. American journal of ophthalmology. 2005 Sep:140(3):509-16 [PubMed PMID: 16196117]
Agrawal RV, Murthy S, Sangwan V, Biswas J. Current approach in diagnosis and management of anterior uveitis. Indian journal of ophthalmology. 2010 Jan-Feb:58(1):11-9. doi: 10.4103/0301-4738.58468. Epub [PubMed PMID: 20029142]
Duplechain A, Conrady CD, Patel BC, Baker S. Uveitis. StatPearls. 2023 Jan:(): [PubMed PMID: 31082037]
Harthan JS, Opitz DL, Fromstein SR, Morettin CE. Diagnosis and treatment of anterior uveitis: optometric management. Clinical optometry. 2016:8():23-35. doi: 10.2147/OPTO.S72079. Epub 2016 Mar 31 [PubMed PMID: 30214346]
Wakefield D,Clarke D,McCluskey P, Recent Developments in HLA B27 Anterior Uveitis. Frontiers in immunology. 2020 [PubMed PMID: 33469457]
Kestelyn PG, An eye on inflammatory eye disease. Acta clinica Belgica. 2005 Sep-Oct [PubMed PMID: 16398326]
Biggioggero M,Crotti C,Becciolini A,Miserocchi E,Favalli EG, The Management of Acute Anterior Uveitis Complicating Spondyloarthritis: Present and Future. BioMed research international. 2018 [PubMed PMID: 30406148]
Gallagher KT,Bernstein B, Juvenile rheumatoid arthritis. Current opinion in rheumatology. 1999 Sep; [PubMed PMID: 10503657]
Level 3 (low-level) evidenceUngaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet (London, England). 2017 Apr 29:389(10080):1756-1770. doi: 10.1016/S0140-6736(16)32126-2. Epub 2016 Dec 1 [PubMed PMID: 27914657]
Barth WF,Segal K, Reactive arthritis (Reiter's syndrome). American family physician. 1999 Aug [PubMed PMID: 10465225]
Ungprasert P,Ryu JH,Matteson EL, Clinical Manifestations, Diagnosis, and Treatment of Sarcoidosis. Mayo Clinic proceedings. Innovations, quality & outcomes. 2019 Sep [PubMed PMID: 31485575]
Level 2 (mid-level) evidenceNair JR,Moots RJ, Behcet's disease. Clinical medicine (London, England). 2017 Feb [PubMed PMID: 28148585]
Clive DM, Vanguri VK. The Syndrome of Tubulointerstitial Nephritis With Uveitis (TINU). American journal of kidney diseases : the official journal of the National Kidney Foundation. 2018 Jul:72(1):118-128. doi: 10.1053/j.ajkd.2017.11.013. Epub 2018 Feb 9 [PubMed PMID: 29429748]
Fava A, Petri M. Systemic lupus erythematosus: Diagnosis and clinical management. Journal of autoimmunity. 2019 Jan:96():1-13. doi: 10.1016/j.jaut.2018.11.001. Epub 2018 Nov 16 [PubMed PMID: 30448290]
Ghasemi N, Razavi S, Nikzad E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell journal. 2017 Apr-Jun:19(1):1-10 [PubMed PMID: 28367411]
Zhu W,He X,Cheng K,Zhang L,Chen D,Wang X,Qiu G,Cao X,Weng X, Ankylosing spondylitis: etiology, pathogenesis, and treatments. Bone research. 2019 [PubMed PMID: 31666997]
Level 2 (mid-level) evidenceHolmes KK, Bertozzi S, Bloom BR, Jha P, Bloom BR, Atun R, Cohen T, Dye C, Fraser H, Gomez GB, Knight G, Murray M, Nardell E, Rubin E, Salomon J, Vassall A, Volchenkov G, White R, Wilson D, Yadav P. Tuberculosis. Major Infectious Diseases. 2017 Nov 3:(): [PubMed PMID: 30212088]
Mohseni M, Sung S, Takov V. Chlamydia. StatPearls. 2024 Jan:(): [PubMed PMID: 30725971]
Biesiada G,Czepiel J,Leśniak MR,Garlicki A,Mach T, Lyme disease: review. Archives of medical science : AMS. 2012 Dec 20 [PubMed PMID: 23319969]
Whitley RJ, Herpes simplex virus infection. Seminars in pediatric infectious diseases. 2002 Jan [PubMed PMID: 12118847]
Halonen SK, Weiss LM. Toxoplasmosis. Handbook of clinical neurology. 2013:114():125-45. doi: 10.1016/B978-0-444-53490-3.00008-X. Epub [PubMed PMID: 23829904]
Level 3 (low-level) evidenceJohnson RW,Alvarez-Pasquin MJ,Bijl M,Franco E,Gaillat J,Clara JG,Labetoulle M,Michel JP,Naldi L,Sanmarti LS,Weinke T, Herpes zoster epidemiology, management, and disease and economic burden in Europe: a multidisciplinary perspective. Therapeutic advances in vaccines. 2015 Jul [PubMed PMID: 26478818]
Level 3 (low-level) evidenceReddy AK,Engelhard SB,Shah CT,Sim AJ,Thorne JE, Medical Malpractice in Uveitis: A Review of Clinical Entities and Outcomes. Ocular immunology and inflammation. 2018; [PubMed PMID: 27715388]
Delwig A,Keenan JD,Margolis TP, Topical Valganciclovir for the Treatment of Hypertensive Anterior Uveitis. Cornea. 2015 Nov; [PubMed PMID: 26356754]
Moorthy RS,London NJ,Garg SJ,Cunningham ET Jr, Drug-induced uveitis. Current opinion in ophthalmology. 2013 Nov [PubMed PMID: 24100371]
Level 3 (low-level) evidenceKubicka-Trzaska A,Romanowska-Dixon B, Malignant uveitis masquerade syndromes. Klinika oczna. 2008; [PubMed PMID: 18655462]
Cypel TK,Zuker RM, Juvenile xanthogranuloma: case report and review of the literature. The Canadian journal of plastic surgery = Journal canadien de chirurgie plastique. 2008 Fall [PubMed PMID: 19721800]
Level 3 (low-level) evidenceYeung IY,Popp NA,Chan CC, The role of sex in uveitis and ocular inflammation. International ophthalmology clinics. 2015 Summer; [PubMed PMID: 26035764]
D'Ambrosio EM, La Cava M, Tortorella P, Gharbiya M, Campanella M, Iannetti L. Clinical Features and Complications of the HLA-B27-associated Acute Anterior Uveitis: A Metanalysis. Seminars in ophthalmology. 2017:32(6):689-701. doi: 10.3109/08820538.2016.1170158. Epub 2016 Jul 12 [PubMed PMID: 27404944]
Rodriguez A,Calonge M,Pedroza-Seres M,Akova YA,Messmer EM,D'Amico DJ,Foster CS, Referral patterns of uveitis in a tertiary eye care center. Archives of ophthalmology (Chicago, Ill. : 1960). 1996 May [PubMed PMID: 8619771]
Miller MM, Ankylosing spondylitis, Reiter's syndrome, psoriatic arthritis, and arthritis of inflammatory bowel disease. Primary care. 1984 Jun; [PubMed PMID: 6332327]
Sen HN,Davis J,Ucar D,Fox A,Chan CC,Goldstein DA, Gender disparities in ocular inflammatory disorders. Current eye research. 2015 Feb [PubMed PMID: 24987987]
DARRELL RW,WAGENER HP,KURLAND LT, Epidemiology of uveitis. Incidence and prevalence in a small urban community. Archives of ophthalmology (Chicago, Ill. : 1960). 1962 Oct; [PubMed PMID: 13883604]
Gritz DC, Wong IG. Incidence and prevalence of uveitis in Northern California; the Northern California Epidemiology of Uveitis Study. Ophthalmology. 2004 Mar:111(3):491-500; discussion 500 [PubMed PMID: 15019324]
Level 2 (mid-level) evidenceSuhler EB, Lloyd MJ, Choi D, Rosenbaum JT, Austin DF. Incidence and prevalence of uveitis in Veterans Affairs Medical Centers of the Pacific Northwest. American journal of ophthalmology. 2008 Dec:146(6):890-6.e8. doi: 10.1016/j.ajo.2008.09.014. Epub [PubMed PMID: 19027424]
Level 2 (mid-level) evidenceReeves SW, Sloan FA, Lee PP, Jaffe GJ. Uveitis in the elderly: epidemiological data from the National Long-term Care Survey Medicare Cohort. Ophthalmology. 2006 Feb:113(2):307.e1 [PubMed PMID: 16406541]
Level 2 (mid-level) evidenceDigre KB, Brennan KC. Shedding light on photophobia. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2012 Mar:32(1):68-81. doi: 10.1097/WNO.0b013e3182474548. Epub [PubMed PMID: 22330853]
Balamurugan S, Das D, Hasanreisoglu M, Toy BC, Akhter M, Anuradha VK, Anthony E, Gurnani B, Kaur K. Interleukins and cytokine biomarkers in uveitis. Indian journal of ophthalmology. 2020 Sep:68(9):1750-1763. doi: 10.4103/ijo.IJO_564_20. Epub [PubMed PMID: 32823391]
Akinsoji E,Goldhardt R,Galor A, A Glimpse into Uveitis in the Aging Eye: Pathophysiology, Clinical Presentation and Treatment Considerations. Drugs & aging. 2018 May [PubMed PMID: 29663152]
Yanai R,Takeda A,Yoshimura T,Sonoda KH, [Pathophysiology and new treatment of uveitis]. Nihon Rinsho Men'eki Gakkai kaishi = Japanese journal of clinical immunology. 2014 [PubMed PMID: 24835134]
Shah KK, Pritt BS, Alexander MP. Histopathologic review of granulomatous inflammation. Journal of clinical tuberculosis and other mycobacterial diseases. 2017 May:7():1-12. doi: 10.1016/j.jctube.2017.02.001. Epub 2017 Feb 10 [PubMed PMID: 31723695]
Saygın D,Syed AU,Lowder CY,Srivastava S,Maya JJ,Hajj-Ali RA, Characteristics of inflammatory eye disease associated with hidradenitis suppurativa. European journal of rheumatology. 2018 Sep [PubMed PMID: 30071934]
Mérida S,Palacios E,Navea A,Bosch-Morell F, Macrophages and Uveitis in Experimental Animal Models. Mediators of inflammation. 2015 [PubMed PMID: 26078494]
Level 3 (low-level) evidenceJoltikov KA,Lobo-Chan AM, Epidemiology and Risk Factors in Non-infectious Uveitis: A Systematic Review. Frontiers in medicine. 2021 [PubMed PMID: 34568364]
Level 1 (high-level) evidencePhillips CI,Clark CV,Levy AM, Posterior synechiae after glaucoma operations: aggravation by shallow anterior chamber and pilocarpine. The British journal of ophthalmology. 1987 Jun; [PubMed PMID: 3620422]
Nche EN, Amer R. Lens-induced uveitis: an update. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2020 Jul:258(7):1359-1365. doi: 10.1007/s00417-019-04598-3. Epub 2020 Jan 6 [PubMed PMID: 31907641]
Bakunowicz-Lazarczyk A,Proniewska-Skretek E,Walkowiak M,Grochowski J, [Parasitic uveitis in children]. Klinika oczna. 1992 [PubMed PMID: 1640677]
Read RW,Zamir E,Rao NA, Neoplastic masquerade syndromes. Survey of ophthalmology. 2002 Mar-Apr [PubMed PMID: 11918892]
Level 3 (low-level) evidenceAbrahams IW, Diagnosis and surgical management of phacoanaphylactic uveitis following extracapsular cataract extraction with intraocular lens implantation. Journal - American Intra-Ocular Implant Society. 1985 Sep; [PubMed PMID: 4044382]
Level 3 (low-level) evidenceRodriguez-Perez JC,Cruz-Alamo M,Perez-Aciego P,Macía-Heras M,Naranjo-Hernandez A,Plaza-Toledano C,Hortal-Cascon L,Fernandez-Rodriguez A, Clinical and immune aspects of idiopathic acute tubulointerstitial nephritis and uveitis syndrome. American journal of nephrology. 1995; [PubMed PMID: 7503137]
Ormerod LD,Puklin JE,Giles CL, Chronic Propionibacterium acnes endophthalmitis as a cause of intermediate uveitis. Ocular immunology and inflammation. 1997 Mar [PubMed PMID: 9145695]
Level 3 (low-level) evidenceGurnani B, Kaur K. Endogenous Endophthalmitis. StatPearls. 2024 Jan:(): [PubMed PMID: 35015416]
Schwock J,Geddie WR, Diagnosis of B-cell non-hodgkin lymphomas with small-/intermediate-sized cells in cytopathology. Pathology research international. 2012 [PubMed PMID: 22693682]
Wang BH,Yao YF, Effect of primary iris and ciliary body cyst on anterior chamber angle in patients with shallow anterior chamber. Journal of Zhejiang University. Science. B. 2012 Sep; [PubMed PMID: 22949363]
Ozdal PC, Berker N, Tugal-Tutkun I. Pars Planitis: Epidemiology, Clinical Characteristics, Management and Visual Prognosis. Journal of ophthalmic & vision research. 2015 Oct-Dec:10(4):469-80. doi: 10.4103/2008-322X.176897. Epub [PubMed PMID: 27051493]
Sudharshan S,Ganesh SK,Biswas J, Current approach in the diagnosis and management of posterior uveitis. Indian journal of ophthalmology. 2010 Jan-Feb [PubMed PMID: 20029144]
Coburn J,Garcia B,Hu LT,Jewett MW,Kraiczy P,Norris SJ,Skare J, Lyme Disease Pathogenesis. Current issues in molecular biology. 2021 [PubMed PMID: 33353871]
Deschenes J,Murray PI,Rao NA,Nussenblatt RB,International Uveitis Study Group., International Uveitis Study Group (IUSG): clinical classification of uveitis. Ocular immunology and inflammation. 2008 Jan-Feb [PubMed PMID: 18379933]
Trusko B,Thorne J,Jabs D,Belfort R,Dick A,Gangaputra S,Nussenblatt R,Okada A,Rosenbaum J,Standardization of Uveitis Nomenclature (SUN) Project., The Standardization of Uveitis Nomenclature (SUN) Project. Development of a clinical evidence base utilizing informatics tools and techniques. Methods of information in medicine. 2013; [PubMed PMID: 23392263]
Jabs DA,Busingye J, Approach to the diagnosis of the uveitides. American journal of ophthalmology. 2013 Aug [PubMed PMID: 23668682]
Micieli JA,Margolin E, A 30-year-old woman with vision loss and painful eye movements. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2015 Jun 16; [PubMed PMID: 25869872]
Oshika T,Nishi M,Mochizuki M,Nakamura M,Kawashima H,Iwase K,Sawa M, Quantitative assessment of aqueous flare and cells in uveitis. Japanese journal of ophthalmology. 1989 [PubMed PMID: 2796009]
Zaidi AA, Ying GS, Daniel E, Gangaputra S, Rosenbaum JT, Suhler EB, Thorne JE, Foster CS, Jabs DA, Levy-Clarke GA, Nussenblatt RB, Kempen JH, Systemic Immunosuppressive Therapy for Eye Diseases Cohort Study. Hypopyon in patients with uveitis. Ophthalmology. 2010 Feb:117(2):366-72. doi: 10.1016/j.ophtha.2009.07.025. Epub 2009 Dec 14 [PubMed PMID: 20006905]
Level 2 (mid-level) evidencePujari A,Temkar S,Singh R,Urkude J, Child with hypopyon. BMJ case reports. 2017 Oct 20; [PubMed PMID: 29054898]
Level 3 (low-level) evidencePillai CT,Dua HS,Azuara-Blanco A,Sarhan AR, Evaluation of corneal endothelium and keratic precipitates by specular microscopy in anterior uveitis. The British journal of ophthalmology. 2000 Dec [PubMed PMID: 11090474]
Van der Lelij A,Ooijman FM,Kijlstra A,Rothova A, Anterior uveitis with sectoral iris atrophy in the absence of keratitis: a distinct clinical entity among herpetic eye diseases. Ophthalmology. 2000 Jun; [PubMed PMID: 10857838]
Level 2 (mid-level) evidenceMyers TD,Smith JR,Lauer AK,Rosenbaum JT, Iris nodules associated with infectious uveitis. The British journal of ophthalmology. 2002 Sep [PubMed PMID: 12185117]
Level 3 (low-level) evidenceMessina M,Elalfy M,Fares U,Ghoz N,Mavi B,Dua H, Creeping posterior synechiae following hyperopic iris-fixated phakic implants. International ophthalmology. 2016 Dec [PubMed PMID: 26909500]
Stelzer O, [Iris heterochromia: variations in form, age changes, sex dimorphism]. Anthropologischer Anzeiger; Bericht uber die biologisch-anthropologische Literatur. 1979 Jun; [PubMed PMID: 485098]
Cernák M,Markovic O,Cernák A, [The treatment of the rubeosis of the iris and the neovascular glaucoma in proliferative diabetic retinopathy by means of anti-VEGF]. Ceska a slovenska oftalmologie : casopis Ceske oftalmologicke spolecnosti a Slovenske oftalmologicke spolecnosti. 2008 Nov [PubMed PMID: 19110964]
Alkhayyal MA,Stone DU, Practice patterns for herpes simplex keratitis: A survey of ophthalmologists in Gulf Coast countries. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2017 Apr-Jun; [PubMed PMID: 28559714]
Level 3 (low-level) evidenceLee MI,Lee AW,Sumsion SM,Gorchynski JA, Don't Forget What You Can't See: A Case of Ocular Syphilis. The western journal of emergency medicine. 2016 Jul; [PubMed PMID: 27429702]
Level 3 (low-level) evidenceKujundzić M, [The role of biologic therapy in the treatment of extraintestinal manifestations and complications of inflammatory bowel disease]. Acta medica Croatica : casopis Hravatske akademije medicinskih znanosti. 2013 Apr; [PubMed PMID: 24471303]
Adio AO,Alikor A,Awoyesuku E, Survey of pediatric ophthalmic diagnoses in a teaching hospital in Nigeria. Nigerian journal of medicine : journal of the National Association of Resident Doctors of Nigeria. 2011 Jan-Mar; [PubMed PMID: 21970270]
Level 3 (low-level) evidenceMajumder PD,Sudharshan S,Biswas J, Laboratory support in the diagnosis of uveitis. Indian journal of ophthalmology. 2013 Jun; [PubMed PMID: 23803478]
Lardenoye CW, van Kooij B, Rothova A. Impact of macular edema on visual acuity in uveitis. Ophthalmology. 2006 Aug:113(8):1446-9 [PubMed PMID: 16877081]
Level 2 (mid-level) evidenceBaneke AJ, Lim KS, Stanford M. The Pathogenesis of Raised Intraocular Pressure in Uveitis. Current eye research. 2016:41(2):137-49. doi: 10.3109/02713683.2015.1017650. Epub 2015 May 14 [PubMed PMID: 25974243]
Rathinam SR, Babu M. Algorithmic approach in the diagnosis of uveitis. Indian journal of ophthalmology. 2013 Jun:61(6):255-62. doi: 10.4103/0301-4738.114092. Epub [PubMed PMID: 23803476]
Yemm RW,Pecen PE,Fliney GD,Palestine AG, Chest X-ray and Uveitis Evaluation in a Population with Low Incidence of Sarcoidosis. Ophthalmology and therapy. 2020 Sep [PubMed PMID: 32613593]
Dessì G, Lahuerta EF, Puce FG, Mendoza LH, Stefanini T, Rosenberg I, Del Prato A, Perinetti M, Villa A. Role of B-scan ocular ultrasound as an adjuvant for the clinical assessment of eyeball diseases: a pictorial essay. Journal of ultrasound. 2015 Sep:18(3):265-77. doi: 10.1007/s40477-014-0153-y. Epub 2014 Dec 30 [PubMed PMID: 26261467]
Regatieri CV,Alwassia A,Zhang JY,Vora R,Duker JS, Use of optical coherence tomography in the diagnosis and management of uveitis. International ophthalmology clinics. 2012 Fall [PubMed PMID: 22954927]
Herbort CP, Fluorescein and indocyanine green angiography for uveitis. Middle East African journal of ophthalmology. 2009 Oct [PubMed PMID: 20404985]
Agrawal RV, Biswas J, Gunasekaran D. Indocyanine green angiography in posterior uveitis. Indian journal of ophthalmology. 2013 Apr:61(4):148-59. doi: 10.4103/0301-4738.112159. Epub [PubMed PMID: 23685486]
Marchese A,Agarwal A,Moretti AG,Handa S,Modorati G,Querques G,Bandello F,Gupta V,Miserocchi E, Advances in imaging of uveitis. Therapeutic advances in ophthalmology. 2020 Jan-Dec [PubMed PMID: 32524072]
Level 3 (low-level) evidenceVojvodić S,Ademović-Sazdanić D,Busarčević 1st, Human leukocyte antigen-b27 and disease susceptibility in vojvodina, serbia. Balkan journal of medical genetics : BJMG. 2012 Dec; [PubMed PMID: 24052732]
Shah D,Marfatia YS, Serological tests for syphilis. Indian journal of sexually transmitted diseases and AIDS. 2019 Jul-Dec [PubMed PMID: 31922115]
Weinreb RN,O'Donnell JJ,Sandman R,Char DH,Kimura SJ, Angiotensin-converting enzyme in sarcoid uveitis. Investigative ophthalmology & visual science. 1979 Dec [PubMed PMID: 229083]
Harrison M. Erythrocyte sedimentation rate and C-reactive protein. Australian prescriber. 2015 Jun:38(3):93-4 [PubMed PMID: 26648629]
Schriefer ME, Lyme Disease Diagnosis: Serology. Clinics in laboratory medicine. 2015 Dec [PubMed PMID: 26593258]
Kasapçopur O,Yologlu N,Ozyazgan Y,Ercan G,Caliskan S,Sever L,Ozdogan H,Arisoy N, Uveitis and anti nuclear antibody positivity in children with juvenile idiopathic arthritis. Indian pediatrics. 2004 Oct; [PubMed PMID: 15523130]
Hagen EC,van de Vijver-Reenalda H,de Keizer RJ,Kijlstra A,van Es LA,Daha MR,van der Woude FJ, Uveitis and anti-neutrophil cytoplasmic antibodies. Clinical and experimental immunology. 1994 Jan [PubMed PMID: 8287609]
Ang M,Wong W,Ngan CC,Chee SP, Interferon-gamma release assay as a diagnostic test for tuberculosis-associated uveitis. Eye (London, England). 2012 May [PubMed PMID: 22302066]
Level 2 (mid-level) evidenceZhu J,Jiang Y,Shi Y,Zheng B,Xu Z,Jia W, Clinical manifestations and treatment outcomes of syphilitic uveitis in HIV-negative patients in China: A retrospective case study. Medicine. 2017 Oct; [PubMed PMID: 29069031]
Level 2 (mid-level) evidenceAllegri P,Rissotto R,Herbort CP,Murialdo U, CNS diseases and uveitis. Journal of ophthalmic & vision research. 2011 Oct [PubMed PMID: 22454751]
Patnaik G,Annamalai R,Biswas J, Intraocular biopsy in uveitis. Indian journal of ophthalmology. 2020 Sep; [PubMed PMID: 32823400]
Damato EM,Angi M,Romano MR,Semeraro F,Costagliola C, Vitreous analysis in the management of uveitis. Mediators of inflammation. 2012 [PubMed PMID: 23150722]
Biswas J,Annamalai R,Krishnaraj V, Biopsy pathology in uveitis. Middle East African journal of ophthalmology. 2011 Oct [PubMed PMID: 22224013]
Doycheva D,Deuter C,Grajewski R, [Topical Corticosteroids and Non-steroidal Anti-inflammatory Drugs in the Therapy of Non-infectious Uveitis]. Klinische Monatsblatter fur Augenheilkunde. 2018 May; [PubMed PMID: 29739028]
Rahman W,Pavesio C, A simple technique to administer mydricaine in needle-phobic patients. The British journal of ophthalmology. 2009 Mar [PubMed PMID: 19244033]
Level 3 (low-level) evidenceLerner LE,Patil AJ,Kenney MC,Minckler D, Use of intraocular human recombinant tissue plasminogen activator as an adjunct treatment of posterior synechiae in patients with uveitis. Retinal cases [PubMed PMID: 25389735]
Level 3 (low-level) evidenceBabu K, Mahendradas P. Medical management of uveitis - current trends. Indian journal of ophthalmology. 2013 Jun:61(6):277-83. doi: 10.4103/0301-4738.114099. Epub [PubMed PMID: 23803479]
Lafranco Dafflon M,Tran VT,Guex-Crosier Y,Herbort CP, Posterior sub-Tenon's steroid injections for the treatment of posterior ocular inflammation: indications, efficacy and side effects. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 1999 Apr [PubMed PMID: 10208261]
Level 2 (mid-level) evidenceDegenring RF,Jonas JB, Intravitreal injection of triamcinolone acetonide as treatment for chronic uveitis. The British journal of ophthalmology. 2003 Mar; [PubMed PMID: 12598455]
Level 3 (low-level) evidenceJabs DA, Antimetabolite Therapy for Uveitis: Methotrexate or Mycophenolate? JAMA ophthalmology. 2019 Dec 1 [PubMed PMID: 31503274]
Lee S,Park YJ,Lee JY, The Effect of Tumor Necrosis Factor-Alpha Inhibitors on Uveitis in Patients with Ankylosing Spondylitis. Journal of Korean medical science. 2019 Nov 4 [PubMed PMID: 31674159]
van Laar JAM,Rothova A,Missotten T,Kuijpers RWAM,van Hagen PM,van Velthoven MEJ, Diagnosis and treatment of uveitis; not restricted to the ophthalmologist. Journal of clinical and translational research. 2015 Sep 30 [PubMed PMID: 30873449]
Maini R,O'Sullivan J,Reddy A,Watson S,Edelsten C, The risk of complications of uveitis in a district hospital cohort. The British journal of ophthalmology. 2004 Apr; [PubMed PMID: 15031168]
Level 2 (mid-level) evidenceMurthy SI,Pappuru RR,Latha KM,Kamat S,Sangwan VS, Surgical management in patient with uveitis. Indian journal of ophthalmology. 2013 Jun; [PubMed PMID: 23803480]
McCluskey PJ,Towler HM,Lightman S, Management of chronic uveitis. BMJ (Clinical research ed.). 2000 Feb 26 [PubMed PMID: 10688564]
Engelhard SB,Patrie J,Prenshaw J,Bajwa A,Monahan R,Reddy AK, Traumatic uveitis in the mid-Atlantic United States. Clinical ophthalmology (Auckland, N.Z.). 2015; [PubMed PMID: 26491249]