Introduction
Idiopathic generalized epilepsy is a group of epilepsies accounting for about 20 to 40% of all epilepsies. This group of epilepsies is clinically characterized by the presence of absence seizures, generalized tonic-clonic seizures, and myoclonic seizures with an electroencephalographic pattern of generalized epileptiform spike and wave or polyspike and wave discharge, at times with a shifting predominance on a normal background.[1]
Based on the latest International League Against Epilepsy (ILAE) classification, idiopathic generalized epilepsies include childhood absence epilepsy, juvenile absence epilepsy, juvenile myoclonic epilepsy, and generalized tonic-clonic seizures alone.[2]
Juvenile absence epilepsy is an idiopathic generalized epilepsy syndrome that is recognized by the ILAE (International League Against Epilepsy) that typically starts in adolescence around puberty and is characterized by absence seizures and generalized tonic-clonic seizures. In some patients, there may be additional myoclonic jerks as well.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Though specific genetic etiology is not definitely proven, some genetic associations have been found. Allelic variants of GRIK1 were implicated as conferring genetic susceptibility by Sander et al. Parental consanguinity was reported in 40.3%, and a family history of epilepsy was reported in 41.8%.[4]
Epidemiology
Juvenile absence epilepsy prevalence was estimated to be 0.1 per 1000 persons by one study.[5] It is reported to account for 1 to 2% of childhood epilepsies and about 15%-20% of cases of idiopathic generalized epilepsy with nearly equal distribution between males and females.[4][6][7][8] The age at onset was 12.3+/- 2.8 years.[4]
Pathophysiology
The relationship between genetic variation in the T-type calcium channel gene CACNA1H and childhood absence epilepsy is well established. Novel variants in the CACNA1H alter channel properties contributing to an individual's susceptibility to juvenile absence epilepsy but not sufficient to cause epilepsy on their own.[9]
History and Physical
Almost all patients with juvenile absence epilepsy have absence seizures, while generalized tonic-clonic seizures are seen in about 79 to 95% of patients, and myoclonic jerks are seen in 21 to 39% of patients.[4][10] In about 6% of patients in one study, convulsive status epilepticus was reported.[4] The number of absence seizures is typically much lesser (in the order of less than one a day) compared to Childhood Absence epilepsy, which may be characterized by the occurrence of numerous, up to hundreds of absence seizures per day.[10]
Absence seizures are characterized by sudden impairment of consciousness and may be combined with mild clonic, atonic, tonic components, or automatisms. In JAE, these are typically described as non-pyknoleptic absences where they occur infrequently (less than every day). Patients with myoclonic jerks may overlap with juvenile myoclonic epilepsy.
Evaluation
Childhood absence epilepsy and Juvenile Absence Epilepsy are closely related to idiopathic generalized epilepsies in terms of clinical presentation, EEG findings, and long term prognosis.[10] EEG typically shows a 3 to 6 Hz generalized spike and wave pattern with or without polyspikes (Fig 1).[4][10] Neuroimaging is typically negative though non-specific changes were seen in some.[4][10] A normal EEG in a patient with typical history for JAE should not deter from appropriate diagnosis.
Treatment / Management
The first line of treatment is with valproic acid or lamotrigine. Though ethosuximide may be helpful for absence seizures, it is not effective for generalized tonic-clonic seizures and, therefore, not the first line of treatment for a patient with both absence seizures and generalized tonic-clonic seizures.[8][11][12]
In view of the side-effects of valproic acid, such as teratogenicity and weight gain, it has to be used with caution in young female patients. Therefore lamotrigine may be the preferred agent in this group of patients.
Juvenile absence epilepsy is typically a pharmaco-responsive epilepsy syndrome but some medications may exacerbate seizures such as phenytoin, carbamazepine, oxcarbazepine, gabapentin, pregabalin, and vigabatrin.[13]
Differential Diagnosis
- Benign epilepsy of childhood with centrotemporal spikes
- Benign familial neonatal convulsions
- Benign idiopathy neonatal convulsions
- Benign partial epilepsy of childhood with occipital paroxysms
- Benign epilepsy with affective symptoms
- Childhood absence epilepsy
Prognosis
In a study with long follow up by Trinka et al., 62 % of patients with JAE were in remission [10]. Approximately 18% of patients with JAE progress into juvenile myoclonic epilepsy.[10] Based on the results of the meta-analysis by Bouma et al. on the outcome of absence epilepsies, one-half of patients developed generalized tonic-clonic seizures. The proportion of patients with seizure freedom was 0.78 for absence seizures only and 0.35 for patients who developed additional tonic-clonic seizures.[14] A range of remission rates from 21 to 89% for JAE has been reported. In one study, all patients with JAE relapsed after AED withdrawal, and 25% of patients with JAE continuing on AEDs relapsed.[15] A couple of other studies also showed relapse after AED withdrawal, whereas one prospective study showed that only 3 of 9 seizure-free patients with juvenile absence epilepsy relapsed after medication withdrawal.[16] Though most patients respond well with good seizure control, often life-long anti-epileptic medications are required.[13][10][17]
Complications
SUDEP (Sudden Unexpected Death in Epilepsy) is a much-feared complication of epilepsy. Though several studies have shown that a higher burden of generalized tonic-clonic seizures is a risk factor for SUDEP, it has been reported in a full spectrum of epilepsies, including patients with relatively benign epilepsies.[18]
Childhood absence epilepsy is often thought to have a better prognosis than Juvenile absence epilepsy though this is not entirely supported by data.[19][20] The presence of generalized tonic-clonic seizures is a predictor for a poorer outcome.[21]
Though traditionally, patients with absence epilepsy were considered to have normal cognitive functioning, several recent studies showed weaknesses in various domains such as behavior, emotion, executive functioning, intelligence, attention, and language.[22][23][24] Cognitive development was also not associated with seizure freedom. Mild-to-severe academic underachievement was present in 65% and comorbidities that might affect learning by 38%.[22]
Deterrence and Patient Education
Patients should be counseled about the need for avoidance of provocative factors such as sleep deprivation and alcohol consumption. Hyperventilation may also precipitate absence seizures.
Pearls and Other Issues
There is a significant overlap in the clinical presentation of childhood absence epilepsy and juvenile absence epilepsy. The absences of childhood absence epilepsy are very frequent, up to hundreds each day and shorter in duration whereas the absences in juvenile myoclonic epilepsy are less frequent, with less severe impairment of consciousness and longer in duration than those in childhood absence epilepsy. Some studies refer to absences of CAE as pyknoleptic and those if JAE as non-pyknoleptic.
Enhancing Healthcare Team Outcomes
In view of the possibility of cognitive weaknesses that may affect academic performance even in seemingly normal individuals with Juvenile Absence Epilepsy, having a low threshold for early referral to Neuropsychology for cognitive testing would be beneficial.
Patients and families must be educated regarding SUDEP (Sudden unexpected death in epilepsy) and patient safety strategies must be discussed.
Due to teratogenic side-effects of anti-epileptic medications as well as their interaction with hormonal contraceptives, these should be specifically discussed in female patients, and referral to gynecology and obstetrics should be considered when appropriate.[25]
Media
(Click Image to Enlarge)
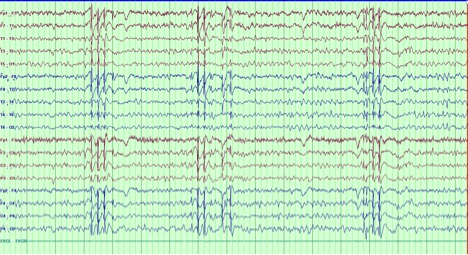
Fig 1 EEG showing 3-3.5 Hz Generalized Spike and wave and polyspike and wave discharges Contributed by the author Sisira Yadala,MD
References
Koutroumanidis M, Arzimanoglou A, Caraballo R, Goyal S, Kaminska A, Laoprasert P, Oguni H, Rubboli G, Tatum W, Thomas P, Trinka E, Vignatelli L, Moshé SL. The role of EEG in the diagnosis and classification of the epilepsy syndromes: a tool for clinical practice by the ILAE Neurophysiology Task Force (Part 1). Epileptic disorders : international epilepsy journal with videotape. 2017 Sep 1:19(3):233-298. doi: 10.1684/epd.2017.0935. Epub [PubMed PMID: 28984246]
Scheffer IE, Berkovic S, Capovilla G, Connolly MB, French J, Guilhoto L, Hirsch E, Jain S, Mathern GW, Moshé SL, Nordli DR, Perucca E, Tomson T, Wiebe S, Zhang YH, Zuberi SM. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017 Apr:58(4):512-521. doi: 10.1111/epi.13709. Epub 2017 Mar 8 [PubMed PMID: 28276062]
Engel J Jr. Report of the ILAE classification core group. Epilepsia. 2006 Sep:47(9):1558-68 [PubMed PMID: 16981873]
Asadi-Pooya AA, Emami M, Sperling MR. A clinical study of syndromes of idiopathic (genetic) generalized epilepsy. Journal of the neurological sciences. 2013 Jan 15:324(1-2):113-7. doi: 10.1016/j.jns.2012.10.014. Epub 2012 Nov 10 [PubMed PMID: 23149265]
Level 2 (mid-level) evidenceSidenvall R, Forsgren L, Blomquist HK, Heijbel J. A community-based prospective incidence study of epileptic seizures in children. Acta paediatrica (Oslo, Norway : 1992). 1993 Jan:82(1):60-5 [PubMed PMID: 8453224]
Jallon P, Latour P. Epidemiology of idiopathic generalized epilepsies. Epilepsia. 2005:46 Suppl 9():10-4 [PubMed PMID: 16302871]
Level 2 (mid-level) evidenceOlafsson E, Hauser WA, Ludvigsson P, Gudmundsson G. Incidence of epilepsy in rural Iceland: a population-based study. Epilepsia. 1996 Oct:37(10):951-5 [PubMed PMID: 8822693]
Wirrell E. Infantile, Childhood, and Adolescent Epilepsies. Continuum (Minneapolis, Minn.). 2016 Feb:22(1 Epilepsy):60-93. doi: 10.1212/CON.0000000000000269. Epub [PubMed PMID: 26844731]
Heron SE, Khosravani H, Varela D, Bladen C, Williams TC, Newman MR, Scheffer IE, Berkovic SF, Mulley JC, Zamponi GW. Extended spectrum of idiopathic generalized epilepsies associated with CACNA1H functional variants. Annals of neurology. 2007 Dec:62(6):560-8 [PubMed PMID: 17696120]
Trinka E, Baumgartner S, Unterberger I, Unterrainer J, Luef G, Haberlandt E, Bauer G. Long-term prognosis for childhood and juvenile absence epilepsy. Journal of neurology. 2004 Oct:251(10):1235-41 [PubMed PMID: 15503104]
Level 2 (mid-level) evidenceGlauser T, Ben-Menachem E, Bourgeois B, Cnaan A, Guerreiro C, Kälviäinen R, Mattson R, French JA, Perucca E, Tomson T, ILAE Subcommission on AED Guidelines. Updated ILAE evidence review of antiepileptic drug efficacy and effectiveness as initial monotherapy for epileptic seizures and syndromes. Epilepsia. 2013 Mar:54(3):551-63. doi: 10.1111/epi.12074. Epub 2013 Jan 25 [PubMed PMID: 23350722]
Moosa ANV. Antiepileptic Drug Treatment of Epilepsy in Children. Continuum (Minneapolis, Minn.). 2019 Apr:25(2):381-407. doi: 10.1212/CON.0000000000000712. Epub [PubMed PMID: 30921015]
Pearl PL. Epilepsy Syndromes in Childhood. Continuum (Minneapolis, Minn.). 2018 Feb:24(1, Child Neurology):186-209. doi: 10.1212/CON.0000000000000568. Epub [PubMed PMID: 29432243]
Bouma PA, Westendorp RG, van Dijk JG, Peters AC, Brouwer OF. The outcome of absence epilepsy: a meta-analysis. Neurology. 1996 Sep:47(3):802-8 [PubMed PMID: 8797483]
Level 1 (high-level) evidenceHealy L, Moran M, Singhal S, O'Donoghue MF, Alzoubidi R, Whitehouse WP. Relapse after treatment withdrawal of antiepileptic drugs for Juvenile Absence Epilepsy and Juvenile Myoclonic Epilepsy. Seizure. 2018 Jul:59():116-122. doi: 10.1016/j.seizure.2018.05.015. Epub 2018 May 20 [PubMed PMID: 29807291]
Shinnar S, Berg AT, Moshé SL, Kang H, O'Dell C, Alemany M, Goldensohn ES, Hauser WA. Discontinuing antiepileptic drugs in children with epilepsy: a prospective study. Annals of neurology. 1994 May:35(5):534-45 [PubMed PMID: 8179299]
Level 2 (mid-level) evidenceAiguabella Macau M, Falip Centellas M, Veciana de Las Heras M, Climent Perín MA, Miró Lladó J, Moreno Gómez I, Elices Palomar E. Long term prognosis of juvenile absence epilepsy. Neurologia (Barcelona, Spain). 2011 May:26(4):193-9. doi: 10.1016/j.nrl.2010.09.005. Epub 2010 Nov 13 [PubMed PMID: 21163225]
Level 2 (mid-level) evidenceVerducci C, Hussain F, Donner E, Moseley BD, Buchhalter J, Hesdorffer D, Friedman D, Devinsky O. SUDEP in the North American SUDEP Registry: The full spectrum of epilepsies. Neurology. 2019 Jul 16:93(3):e227-e236. doi: 10.1212/WNL.0000000000007778. Epub 2019 Jun 19 [PubMed PMID: 31217259]
Holtkamp M, Janz D, Kirschbaum A, Kowski AB, Vorderwülbecke BJ. Absence epilepsy beyond adolescence: an outcome analysis after 45 years of follow-up. Journal of neurology, neurosurgery, and psychiatry. 2018 Jun:89(6):603-610. doi: 10.1136/jnnp-2017-317052. Epub 2018 Jan 18 [PubMed PMID: 29348303]
Beghi M, Beghi E, Cornaggia CM, Gobbi G. Idiopathic generalized epilepsies of adolescence. Epilepsia. 2006:47 Suppl 2():107-10 [PubMed PMID: 17105478]
Tovia E, Goldberg-Stern H, Shahar E, Kramer U. Outcome of children with juvenile absence epilepsy. Journal of child neurology. 2006 Sep:21(9):766-8 [PubMed PMID: 16970883]
Level 2 (mid-level) evidenceFonseca Wald ELA, Klinkenberg S, Voncken TPC, Ebus SCM, Aldenkamp AP, Vles JSH, Vermeulen RJ, Hendriksen JGM, Debeij-Van Hall MHJA. Cognitive development in absence epilepsy during long-term follow-up. Child neuropsychology : a journal on normal and abnormal development in childhood and adolescence. 2019 Nov:25(8):1003-1021. doi: 10.1080/09297049.2019.1614156. Epub 2019 May 30 [PubMed PMID: 31145023]
Caplan R, Siddarth P, Stahl L, Lanphier E, Vona P, Gurbani S, Koh S, Sankar R, Shields WD. Childhood absence epilepsy: behavioral, cognitive, and linguistic comorbidities. Epilepsia. 2008 Nov:49(11):1838-46. doi: 10.1111/j.1528-1167.2008.01680.x. Epub 2008 Jun 13 [PubMed PMID: 18557780]
Cheng D, Yan X, Gao Z, Xu K, Zhou X, Chen Q. Common and Distinctive Patterns of Cognitive Dysfunction in Children With Benign Epilepsy Syndromes. Pediatric neurology. 2017 Jul:72():36-41.e1. doi: 10.1016/j.pediatrneurol.2016.12.005. Epub 2017 Jan 4 [PubMed PMID: 28533141]
Montouris G, Aboumatar S, Burdette D, Kothare S, Kuzniecky R, Rosenfeld W, Chung S. Expert opinion: Proposed diagnostic and treatment algorithms for Lennox-Gastaut syndrome in adult patients. Epilepsy & behavior : E&B. 2020 Sep:110():107146. doi: 10.1016/j.yebeh.2020.107146. Epub 2020 Jun 18 [PubMed PMID: 32563898]
Level 3 (low-level) evidence