Introduction
Lichen sclerosus (LS) is a chronic inflammatory disease. It was first described by Hallopeau in 1881. Since then, multiple names have been used to describe this condition such as leukoplakia, kraurosis vulvae, balanitis xerotica obliterans, and lichen sclerosis et atrophicus. In 1976, the International Society for the Study of Vulvovaginal Disease adopted the term of lichen sclerosus.
LS is a mucocutaneous autoimmune disorder characterized by hypopigmentation and skin atrophy. It involves most commonly the genital skin, less often the extragenital sites. LS is more common in women than in men. It may cause phimosis or scarring of the vaginal introitus. The diagnosis is based on the clinical features, but it is often confirmed by biopsy. The lesions can evolve towards the destruction of anatomic structures, functional impairment and a potential risk for malignant evolution. Thus, treatment and long term follow-up are mandatory.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
LS is considered to be an autoimmune condition; however, its etiology remains unclear. Given its association with other autoimmune diseases such as alopecia areata, vitiligo, autoimmune thyroiditis, and pernicious anemia, its etiology is probably multifactorial. Further etiologic factors have been implicated such as genetic susceptibility, infectious agents such as spirochetes, sex hormone, and the Koebner phenomenon. Furthermore, recent data demonstrated a high prevalence of lichen sclerosis associated with morphea. [1]
Epidemiology
LS is relatively rare. Although reports indicate that it affects between 1 in 1000 and 1 in 300 individuals in the general population, the exact prevalence is unknown. [2] It still seems unknown and underestimated because many patients are asymptomatic, and it is frequently misdiagnosed. Both sexes are affected, but it is more common in women than men with a female to male ratio varies from 1:1 to 10:1. There is no racial predilection. It occurs at all ages. Moreover, its incidence in women has two peaks, the first one occurs between eight and thirteen-year-old girls and the second one is during the fifth and the sixth decades. The mean age at diagnosis ranges between 52 and 60 years. LS occurs in the genital skin in 85 to 98 %, and on the extragenital skin in only 15 to 20 %. [2] Extragenital lichen sclerosus is uncommon during childhood. LS can involve the oral mucosa, known as oral lichen sclerosus, and has been rarely reported.
Pathophysiology
- The underlying pathogenesis of LS includes an infiltrate of activated T cells releasing interleukin 4 (IL 4) and transforming growth factor β (TGF β). So, these cytokines activate fibroblasts producing significantly altered collagen leading to fibrosis. Besides, the pathogenesis includes vascular damage by the decrease in the number of capillaries.
- Interleukin 1 (IL 1) and interleukin one receptor antagonist (IL 1ra) may also be included in the pathogenesis of lichen sclerosus as well as increased number of monoclonal T lymphocyte CD4 +, lymphocyte T dendritic CD1a + cells, macrophages, mast cells, and decreased number of T lymphocyte CD3 +. [3]
- Another hypothesis has been suggested such as an increased number of circulating IgG autoantibodies targeting extracellular matrix 1 (ECM 1) protein leading to widespread deposition of hyaline material in the dermis. [4]
Histopathology
LS has a specific histologic pattern characterized by a band-like lymphocytic infiltrate below a zone of dermal edema and orthokeratotic hyperkeratosis. Histopathology findings vary depending on disease duration. In earlier stages, it shows vacuolar degeneration of the basal layer, hyalinization of subepithelial collagen, decreased elastic fibers in the upper dermis and dilated blood vessels under the basement membrane. In older lesions, histology shows a reduced number of mononuclear cells and dispersed patchy islands of mononuclear cells within the hyalinized dermis. [3][4]
History and Physical
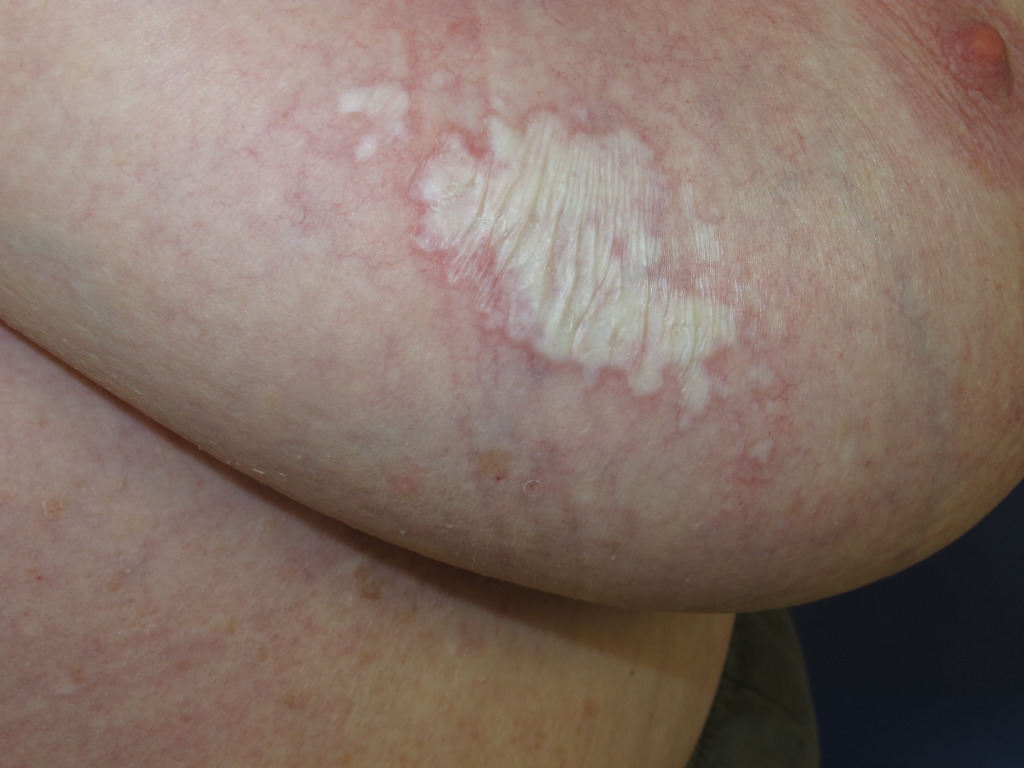
LS affects most commonly the genital site and less often the extragenital area. Typical lesions begin as a sharply demarcated erythema that becomes thin, hypopigmented, ivory-white, porcelain-like, and sclerotic plaques. Plaques may become later thickened due to repeated excoriations. Itch is the main symptom and is often worse at night. Other lesions may include telangiectasias, purpura, fissures, ulcerations, and edema. Typical complaints commonly include significant pruritus, local burning sensation, pain, painful defecation. Constipation is frequent in children but rarely seen in adults. However, lesions can be asymptomatic. Genital lesions begin around the periclitoral hood. The affected area varies from a small and single area to large area involving the entire region of the vulva, perineum, and perianus assuming a typical aspect of ‘keyhole sign.’
However, LS usually spares the vagina and cervix. In girls, LS presents commonly with irritation and soreness although it can mimic sexual abuse. However, LS and sexual abuse can coexist. Visual lichen sclerosus exhibits the Koebner phenomenon at sites of trauma; sexual abuse can aggravate lesions of LS. [5] Male genital LS (boys and men) occurs in the foreskin, glans penis, and the coronal sulcus penis. Extragenital lesions occur on any part of the skin and usually asymptomatic. The most commonly involved areas are inframammary areas, neck, wrists, thighs, upper back, and shoulders. The involvement of the oral mucosa appears clinically as bluish-white papules on the buccal mucosa or under the tongue.
Evaluation
The diagnosis is based on taking a careful history including the autoimmune diseases in the patient and family, examination of the mucosas, extragenital skin and completed by a gynecological exam. Thus, the diagnosis of LS is usually clinical. But in some cases, a biopsy can be performed. However, atypical histology does not rule out the diagnosis.
Biopsies should be performed in case of:
- Atypical clinical presentation
- Suspected malignancy
- Nonresponse, after an appropriate duration, to recommended first-line treatment
The workup of the condition should include investigation of thyroid function, and according to symptoms investigation of the other autoimmune diseases.
Treatment / Management
The aims of the treatment are relief of the symptoms, stopping the atrophy, prevention scar formation, and anatomical distortion, as well as malignant transformation. The therapy includes general care, topical treatments, systemic treatments, and surgical procedures. It is fundamental to inform the patient to avoid the use of irritating products such as soap and to prefer emollients to break the itch-stretch cycle.
For genital LS, the gold standard treatment is three months application of high potency topical steroids (clobetasol propionate). Second-line therapies include topical calcineurin inhibitors and imiquimod. In men, early circumcision may be recommended. Surgery is indicated only for the treatment of complications associated with lichen sclerosus. For extragenital LS, therapeutic modalities are limited and include phototherapy, ultrapotent topical steroids, tacrolimus ointment 0, 1%, and systemic steroids or methotrexate. Follow-up examinations must be kept indefinitely. [6]
Differential Diagnosis
- Lichen planus
- Lichen simplex chronicus
- Vitiligo
- Morphea
- Eczema
- Contact dermatitis
- Psoriasis
- Child sexual abuse
Prognosis
The prognosis of genital LS in children is good. Often the disease may resolve itself spontaneously. LS responds mostly well to local corticosteroid treatment. The forecast is not as positive for extragenital LS and chronic atrophic genital disease.
When untreated, LS leads to disease complications making early diagnosis and treatment crucial. Timely diagnosis and treatment may prevent disease complications.
Although LS is not a precancerous condition, patients with genital LS have an increased risk of squamous cell carcinoma.
Complications
LS is a chronically relapsing disease and if untreated leads to a potential scarring process that may evolve to a complete loss of standard vulvar architecture in women including introital stenosis, fusion, and resorption of the labia minora, and urethral strictures in males. Tissue adhesion and sclerosis lead to tearing and then the loss of sexual function, in addition to dysuria, constipation, itching, and soreness. Furthermore, vulvar lichen sclerosis may evolve to vulvar squamous cell carcinoma in the affected area with an estimated risk up to 5 %; however, its association with penile SCC is not clear. Extragenital lesions are not associated with this risk of transformation. Melanoma and basal cell carcinoma have been reported. [7]
Deterrence and Patient Education
LS may lead to scarring and loss of standard genital architecture. Hence, education of the patient relating to sexual dysfunction may be required.
Given its potential for malignant transformation to squamous cell carcinoma, the patients with anogenital LS should receive long-term follow-up.
Enhancing Healthcare Team Outcomes
It is essential that dermatologists, gynecologists, urologists, surgeons, and pediatricians, respectively, do not hesitate to cooperate. LS may have a negative impact on sexual health. Care coordination by different specialists is necessary to improve outcomes.
Media
(Click Image to Enlarge)
(Click Image to Enlarge)

Kraurosis Vulvae, Lichen Sclerosus, Pathology. Lichen sclerosus is a chronic inflammatory dermatosis that presents as small white raised patches on the genital area.
Contributed by NJ Fiumara, MD, Centers for Disease Control and Prevention
(Click Image to Enlarge)

Lichen sclerosus Image courtesy S Bhimji MD
(Click Image to Enlarge)

Lichen Sclerosus vulva Contributed by Dr. Shyam Verma, MBBS, DVD, FRCP, FAAD, Vadodara, India
References
Bercaw-Pratt JL, Boardman LA, Simms-Cendan JS, North American Society for Pediatric and Adolescent Gynecology. Clinical recommendation: pediatric lichen sclerosus. Journal of pediatric and adolescent gynecology. 2014 Apr:27(2):111-6. doi: 10.1016/j.jpag.2013.11.004. Epub [PubMed PMID: 24602304]
Kreuter A, Kryvosheyeva Y, Terras S, Moritz R, Möllenhoff K, Altmeyer P, Scola N, Gambichler T. Association of autoimmune diseases with lichen sclerosus in 532 male and female patients. Acta dermato-venereologica. 2013 Mar 27:93(2):238-41. doi: 10.2340/00015555-1512. Epub [PubMed PMID: 23224274]
Level 2 (mid-level) evidencePérez-López FR, Vieira-Baptista P. Lichen sclerosus in women: a review. Climacteric : the journal of the International Menopause Society. 2017 Aug:20(4):339-347. doi: 10.1080/13697137.2017.1343295. Epub 2017 Jun 29 [PubMed PMID: 28661705]
Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. American journal of clinical dermatology. 2013 Feb:14(1):27-47. doi: 10.1007/s40257-012-0006-4. Epub [PubMed PMID: 23329078]
Powell JJ, Wojnarowska F. Lichen sclerosus. Lancet (London, England). 1999 May 22:353(9166):1777-83 [PubMed PMID: 10348006]
Kirtschig G. Lichen Sclerosus-Presentation, Diagnosis and Management. Deutsches Arzteblatt international. 2016 May 13:113(19):337-43. doi: 10.3238/arztebl.2016.0337. Epub [PubMed PMID: 27232363]
Halonen P, Jakobsson M, Heikinheimo O, Riska A, Gissler M, Pukkala E. Lichen sclerosus and risk of cancer. International journal of cancer. 2017 May 1:140(9):1998-2002. doi: 10.1002/ijc.30621. Epub 2017 Feb 10 [PubMed PMID: 28124469]