Introduction
Mallory bodies (MBs), also known as Mallory-Denk bodies (MDBs), are cytoplasmic hyaline inclusions of hepatocytes, once thought to be specific for alcohol-related steatohepatitis (ASH). MDBs are also seen in other liver diseases, including metabolic dysfunction-associated steatohepatitis (MASH)—formerly known as nonalcoholic steatohepatitis (NASH),[1] cholestatic liver diseases, primary biliary cirrhosis (PBC), and hepatocellular carcinoma (HCC).[2] In 1911, Frank Burr Mallory discovered these histological findings while examining the hepatocytes of patients with alcoholic hepatitis. In 1975, Helmut Denk found the first animal model of MDBs by feeding mice griseofulvin, resulting in the renaming of these formations.[3] See Image. Mallory Bodies. As a result of transitioning from mouse models to applicability in humans, MDBs were found to primarily comprise keratins, chaperones, co-transporters, and other proteins. Broadly, they are categorized as classic, non-keratinous, rounded, and variants for clinicians grading patient biopsies. Histologically, these subtypes are specified when staging the disease process.
MDBs are formed by stress mechanisms leading to cell cycle dysregulation, which impairs the generation of normal hepatocytes and non-hepatic cells in the body. Since cell cycle dysregulation is a hallmark of the gastrointestinal (GI) diseases mentioned above, MDBs are clinically correlated. To an extent, the formation of MDBs is protective in inflamed tissue to limit further inflammation, leading to fibrosis, but several stressors may eventually accelerate the pathology. The learning activity below discusses the molecular basis of MDBs, the mechanisms by which they are formed, and evidence-based literature on clinical correlations. Typically, the interprofessional team may consist of primary care, gastroenterology, and pathology, leading to continued staging of disease progression. Students within these fields are equipped to identify the histological features of MDBs as they progress in training.
Causes
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Causes
Hepatocytes
In general, MDB formation is known to present in liver diseases. Pertinent liver diseases include hepatitis B and C, alcoholic liver disease, metabolic function-associated steatotic liver disease (MASLD)—formerly known as nonalcoholic fatty liver disease (NAFLD),[1] hepatocellular carcinoma (HCC), focal nodular hyperplasia, Wilson disease, and copper toxicosis.[4] Pertinent gallbladder diseases include primary biliary cholangitis (PBC), chronic cholestasis, and cholangiocarcinoma. However, MDBs may also present following glucocorticoid therapy, intestinal bypass surgery for obesity, Weber-Christian disease, von Gierke disease, radiation pneumonitis, asbestosis, amiodarone, beta lipoproteinemia, porphyria cutanea tarda, antitrypsin deficiency, Indian childhood cirrhosis, perhexiline maleate hepatitis, cirrhosis, 2′3′-dideoxyinosine diethylaminoetheoxyhex-estriol–induced hepatitis, hepatic adenoma, sclerosing hyaline necrosis in Bloom syndrome, and congenital fibrosis.[5]
Non-Hepatic Cells
MDBs are rarely present in non-hepatic cells, but examples exist in asbestosis, renal cell carcinoma, and type 2 pneumocytes.[3] Clinical correlations discuss recent findings in lesser-known diseases detailed below.
Anatomical Pathology
P62 (a sequestosome), ubiquitin, and intermediate filament proteins keratins 8 and 18 (K8/18) are the significant elements that make up a Mallory body. In normal conditions, K8 and 18 are present in 1 to 1 ratio.[6] Protein misfolding, proteasome overload, a ratio of K8 greater than K18, and transamidation of K8 contribute to MDB formation.[7] K8 is insoluble and not easily amenable to degradation, resulting in MDBs. Overexpression of K18 inhibits MDB formation.[3] K8 is likelier to change the helical shape to cross-β sheets, resulting in MDB formation. Formations without K8 do not make MDB, thus linking cross-β sheets as necessary for MDB development.[8][9][10] A similar cross-linking is also seen in protein aggregation disorders such as prion disease and Alzheimer disease.
The results of recent studies continue to extrapolate the correlation of MDBs to other cell cycle markers, including stress-activated markers such as p16 and p21, suggesting a role in cellular senescence rather than just liver pathology.[11] Macrophages involved in the inflammatory process are transcriptionally heterogeneous.[12] Accordingly, aggregates such as MDBs are also implicated in activating nuclear factor-κB, though the downstream effects on inflammation are unknown.[13] The exact mechanism by which inflammation is upregulated is also unknown, though occurring at several stages of the cell regeneration process.
Clinical Pathology
Mallory-Denk bodies are ubiquitously found in alcohol-realted steatohepatitis (ASH), MASH, PBC, and HCC, among other GI disorders. Hepatotoxicity due to medications also causes MDBs; most recently, the use of amiodarone was directly linked.[14] The presence or absence of MDBs can determine a final diagnosis if the consultation of a pathologist is involved. Recently, MDBs were found in patients with COVID-19, suggesting a correlation to the pathological transformation of pneumocytes.[15] Formations appearing similar to MDBs were also seen in ovarian fibromas that underwent torsion.[16] The clinical correlations to conditions outside of gastroenterology are not yet diagnostic. Though MDBs indicate pathology, they do not typically inform the prognosis or influence the mortality rate.
Cytoplasmic inclusion bodies, intracytoplasmic hyaline bodies (IHB), and MDBs can be visualized in HCC.[17] MDB was linked to the steatohepatitis variant of HCC, whereas intracytoplasmic hyaline bodies (IHBs) were not. However, the presence of IHBs correlates with shorter survival than MDBs.[18] MDBs are distinguishable from other cytoplasmic inclusions, such as IHBs. For example, MDBs consist of ubiquitin, p62, and keratin, whereas IHBs only consist of ubiquitin and p62. IHBs have intracytoplasmic hyaline bodies and are a morphological precursor to MDBs.[3][19]
Morphology
Mallory-Denk bodies are predominantly filamentous cytoplasmic inclusions, ranging from 3 to 24 nm versus 10 nm of intermediate filaments.
The bodies are classified as:
- Type I: Parallels filaments
- Type II: Randomly oriented filaments occurring in the periphery
- Type III: Granular, amorphous, and occur around the center
MDBs occur in ballooned hepatocytes, but not all ballooned hepatocytes lead to MDBs; both features indicate active tissue inflammation. The formation occurs in stages:
- Misfolded proteins (typically degraded by the proteasome pathway)
- Young MDB in ballooned hepatocytes
- Mature MDB
They are visible via hematoxylin-eosin stain; however, immunohistochemical staining of cytokeratin or ubiquitin is more sensitive and diagnostic. Pericellular fibrosis and neutrophils tend to surround the hepatocytes with MDB, causing satellitosis.[20] The distribution of MDB in the cells suggests different stages of their formation. For example, small cytoplasmic globular structures are early, large para-nuclear inclusions are mature, and those located in the periphery are considered old.[3] MDB are found in different liver zones and vary in location depending on the disease process. In PBC and Wilson disease, MDBs are seen in zone 1, whereas in ASH and MASLD, they are present in zone 3.[4]
Mechanisms
Before MDBs are formed, hepatocytes balloon, a response to oxidative stress, such as abnormal proteins (heat shock proteins) or fat, resulting in water accumulation in the hepatic cytoplasm.[4] Heat shock protein formation indicates cellular dysfunction.
Three mechanisms describe the formation:
- The first mechanism is that epigenetics (acetylation, methylation, and ubiquitination of histones) contribute to genetic regulation during MDB formation. Hepatocytes have shown stored memory of previous inciting toxicity, leading to gene silencing.
- The second pathway is the shift from the 26S proteasome to the immunoproteasome, though the exact mechanism of gene regulation is unknown. The 26S proteasome degrades intracellular (cytosolic, nuclear, and membrane) proteins.
- The 3,5-diethoxycarbonyl-1,4-dihydrocollidine (DDC) agent induces MDB by changing 26s proteasome to immunoproteasome, accumulating protein.
- When chaperones (ie, heat shock protein 70) and proteins that refold misfolded proteins are uncontrolled, inclusion bodies such as MDB may form.
- Toxins such as alcohol or DDC cause chaperones to become defective.
- Misfolded proteins are targeted by ubiquitination, which signals the molecule via p62 for proteasomal and autophagic degradation.
- The third is the chronic activation of the toll-like signaling receptors (TLR) that stimulate proinflammatory and cell growth pathways.
- Interferon (IFR)-γ and tumor necrosis factor (TNF)-α stimulate TLR, which causes up-regulation of growth factors, resulting in the proliferation of MDB-forming cells.
- Drugs can also create a shift to the formation of the immunoproteasome rather than the 26s proteasome.
- DDC also stimulates TNF-α and IFN-γ expression, activating the TLR. Proinflammatory cytokines TNF-α and IFN-γ via TLR signaling cause up-regulation of the immunoproteasome and down-regulation of the 26s proteasome, resulting in undigested proteins and MDB formation.[3][7][21][22][23]
All 3 mechanisms describe different stress-induced points in the cell cycle, either at deoxyribonucleic acid replication, transcription, or translation. Depending on the inciting event, these mechanisms can occur simultaneously, sequentially, or separately.
Clinicopathologic Correlations
Liver Diseases
Mallory-Denk bodies as a marker for MASLD depend on the histological scoring system. Matteoni et al emphasized the formation of MDBs, while Kleiner et al, which is a more accepted scoring system, did not.[3] Kleiner's system emphasizes fibrosis, steatosis, inflammatory inflammation, and ballooning hepatocytes. Some recommend that the KRT8/K18 ratio is a biomarker for HCC.[6] In patients who use alcohol, a sensitive and specific test to detect MDB is Ub/immunostaining. Inclusions occur in the liver, muscle, and neural tissues, suggesting a common intracellular network of protein synthesis and degradation and responsiveness to stressors. MDBs can be considered a protective mechanism against cell injury or, rather, a step in the pathogenesis of liver damage.[4] The MDBs seem to reoccur within 2 to 3 days in animal models when alcohol use ceases after previous use of alcohol.[20]
Metabolic Dysfunction-Associated Steatohepatitis
Clinical findings of MASH (jaundice, leukocytosis, fever) may demonstrate classical histological findings of steatosis; however, few or no MDBs could be seen. MDBs are less developed in MASH, which tends to be less severe as a hepatic pathology. MASH in children often does not exhibit the formation of MDBs, suggesting that aging may play a role.
Clinical Significance
Areas for Further Research
Abnormal protein folding is known to cause other diseases, including Alzheimer disease. A recent literature review demonstrated common ground between the mechanisms involved in Alzheimer disease and MDB formation. Due to the similarities, future studies should test betaine or S-adenosyl-L-methionine's (SAMe) effect on Alzheimer disease, as they have been shown to prevent MDB formation.[5] Beta sheets that are present in amyloid deposits are also present in MDB.[3]
In patients with alcoholic liver disease, about 70% to 75% have MDB. However, in patients with MASLD, MDB ranges from 7% to 90%.[4] The wide range of MDBs in MASLD is likely the result of not having the specific amount, which qualifies as excessive alcohol use, categorizing the patient as alcoholic rather than non-alcoholic. In severe alcoholic hepatitis, non-responders to corticosteroids had high histopathological findings of ballooning degeneration and MDB, suggesting that histopathological findings can identify those who may respond to corticosteroids.[24] Study results have shown that autophagy contributes to MDB degradation along with other intracellular compartments.[25][26] Fenofibrate, a fibric acid derivative that lowers cholesterol, prevents MDB formation by preventing disruption of the intermediate filament.[27]
Methyl donors like betaine and SAMe prevent MDB formation. SAMe prevents the demethylation of histones, which occurs with DDC. In contrast, betaine prevents MDB formation by preventing the changes in methionine metabolism, and betaine-homocysteine methyltransferase (BHMT) methionine increases from homocysteine.[7][21][28] TLR and p62 pathways are also prevented by betaine and SAMe.
These identified markers for MDBs are potential areas for novel therapeutic intervention at the primary, secondary, tertiary, and quaternary protein formation levels and in patients undergoing treatment for related conditions.[29][30] Though the results in animal studies do not fully apply to clinical medicine, specifically when the MDBs revert or recur, the implications may benefit clinicians treating patients with GI conditions.
Interprofessional Collaboration
Given the established process for identifying, differentiating, and diagnosing conditions based on the presence or absence of MDBs, further inclusion or exclusion criteria could refine the diagnostic process. Though the molecular basis is elucidated, several downstream effects of epigenetics, proteasome regulation, TLR signaling, and immunomodulation are unknown, though the aggregations resemble several protein-aggregating diseases. The role of MDBs in lesser-known reproductive or pulmonary diseases could be explored.
Media
(Click Image to Enlarge)
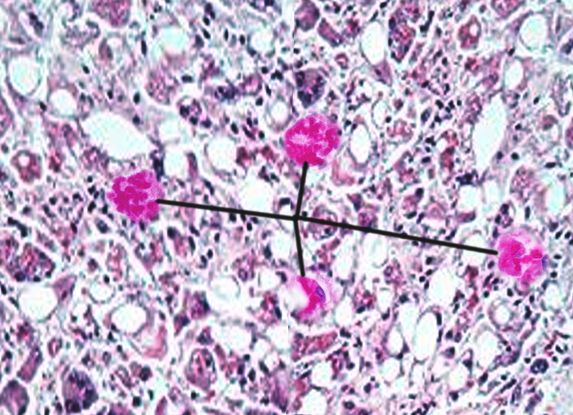
Mallory Bodies. Mallory bodies, also known as Mallory-Denk bodies, are cytoplasmic hyaline inclusions of hepatocytes, once thought to be specific for alcoholic hepatitis.
Contributed by O Chaigasame, MD
References
Rinella ME. Examining the Nomenclature Change From NAFLD and NASH to MASLD and MASH. Gastroenterology & hepatology. 2023 Nov:19(11):697-699 [PubMed PMID: 38405223]
Aishima S, Fujita N, Mano Y, Iguchi T, Taketomi A, Maehara Y, Oda Y, Tsuneyoshi M. p62+ Hyaline inclusions in intrahepatic cholangiocarcinoma associated with viral hepatitis or alcoholic liver disease. American journal of clinical pathology. 2010 Sep:134(3):457-65. doi: 10.1309/AJCP53YVVJCNDZIR. Epub [PubMed PMID: 20716803]
Level 2 (mid-level) evidenceZatloukal K, French SW, Stumptner C, Strnad P, Harada M, Toivola DM, Cadrin M, Omary MB. From Mallory to Mallory-Denk bodies: what, how and why? Experimental cell research. 2007 Jun 10:313(10):2033-49 [PubMed PMID: 17531973]
Level 3 (low-level) evidenceBasaranoglu M, Turhan N, Sonsuz A, Basaranoglu G. Mallory-Denk Bodies in chronic hepatitis. World journal of gastroenterology. 2011 May 7:17(17):2172-7. doi: 10.3748/wjg.v17.i17.2172. Epub [PubMed PMID: 21633525]
French SW, Mendoza AS, Peng Y. The mechanisms of Mallory-Denk body formation are similar to the formation of aggresomes in Alzheimer's disease and other neurodegenerative disorders. Experimental and molecular pathology. 2016 Jun:100(3):426-33. doi: 10.1016/j.yexmp.2016.03.010. Epub 2016 Apr 9 [PubMed PMID: 27068270]
Golob-Schwarzl N, Bettermann K, Mehta AK, Kessler SM, Unterluggauer J, Krassnig S, Kojima K, Chen X, Hoshida Y, Bardeesy NM, Müller H, Svendova V, Schimek MG, Diwoky C, Lipfert A, Mahajan V, Stumptner C, Thüringer A, Fröhlich LF, Stojakovic T, Nilsson KPR, Kolbe T, Rülicke T, Magin TM, Strnad P, Kiemer AK, Moriggl R, Haybaeck J. High Keratin 8/18 Ratio Predicts Aggressive Hepatocellular Cancer Phenotype. Translational oncology. 2019 Feb:12(2):256-268. doi: 10.1016/j.tranon.2018.10.010. Epub 2018 Nov 12 [PubMed PMID: 30439626]
French SW, Bardag-Gorce F, Li J, French BA, Oliva J. Mallory-Denk body pathogenesis revisited. World journal of hepatology. 2010 Aug 27:2(8):295-301. doi: 10.4254/wjh.v2.i8.295. Epub [PubMed PMID: 21161012]
Mahajan V, Klingstedt T, Simon R, Nilsson KP, Thueringer A, Kashofer K, Haybaeck J, Denk H, Abuja PM, Zatloukal K. Cross β-sheet conformation of keratin 8 is a specific feature of Mallory-Denk bodies compared with other hepatocyte inclusions. Gastroenterology. 2011 Sep:141(3):1080-1090.e1-7. doi: 10.1053/j.gastro.2011.05.039. Epub 2011 May 27 [PubMed PMID: 21699779]
Level 3 (low-level) evidenceMurray KA, Hughes MP, Hu CJ, Sawaya MR, Salwinski L, Pan H, French SW, Seidler PM, Eisenberg DS. Identifying amyloid-related diseases by mapping mutations in low-complexity protein domains to pathologies. Nature structural & molecular biology. 2022 Jun:29(6):529-536. doi: 10.1038/s41594-022-00774-y. Epub 2022 May 30 [PubMed PMID: 35637421]
Somlapura M, Gottschalk B, Lahiri P, Kufferath I, Pabst D, Rülicke T, Graier WF, Denk H, Zatloukal K. Different Roles of p62 (SQSTM1) Isoforms in Keratin-Related Protein Aggregation. International journal of molecular sciences. 2021 Jun 9:22(12):. doi: 10.3390/ijms22126227. Epub 2021 Jun 9 [PubMed PMID: 34207662]
Denk H, Abuja PM, Zatloukal K. Mallory-Denk bodies and hepatocellular senescence: a causal relationship? Virchows Archiv : an international journal of pathology. 2024 Apr:484(4):637-644. doi: 10.1007/s00428-024-03748-1. Epub 2024 Jan 30 [PubMed PMID: 38289501]
Zhang R, Zhong B, He J, Yang X, He M, Zeng W, Pan J, Fang Z, Jia J, Liu H. Single-cell transcriptomes identifies characteristic features of mouse macrophages in liver Mallory-Denk bodies formation. Experimental and molecular pathology. 2022 Aug:127():104811. doi: 10.1016/j.yexmp.2022.104811. Epub 2022 Jul 16 [PubMed PMID: 35850229]
Liu Y, Trnka MJ, Guan S, Kwon D, Kim DH, Chen JJ, Greer PA, Burlingame AL, Correia MA. A Novel Mechanism for NF-κB-activation via IκB-aggregation: Implications for Hepatic Mallory-Denk-Body Induced Inflammation. Molecular & cellular proteomics : MCP. 2020 Dec:19(12):1968-1986. doi: 10.1074/mcp.RA120.002316. Epub 2020 Sep 10 [PubMed PMID: 32912968]
Pop A, Halegoua-DeMarzio D, Barnhart H, Kleiner D, Avigan M, Gu J, Chalasani N, Ahmad J, Fontana RJ, Lee W, Barritt AS, Durazo F, Hayashi PH, Navarro VJ. Amiodarone and Dronedarone Causes Liver Injury with Distinctly Different Clinical Presentations. Digestive diseases and sciences. 2024 Apr:69(4):1479-1487. doi: 10.1007/s10620-023-08251-2. Epub 2024 Feb 28 [PubMed PMID: 38416280]
Zubieta-Calleja GR, Zubieta-DeUrioste N, de Jesús Montelongo F, Sanchez MGR, Campoverdi AF, Rocco PRM, Battaglini D, Ball L, Pelosi P. Morphological and functional findings in COVID-19 lung disease as compared to Pneumonia, ARDS, and High-Altitude Pulmonary Edema. Respiratory physiology & neurobiology. 2023 Mar:309():104000. doi: 10.1016/j.resp.2022.104000. Epub 2022 Nov 29 [PubMed PMID: 36460252]
Krishnamurthy K, Stillman IE, Hecht JL, Vyas M. Defining the Nature and Clinicopathologic Significance of Mallory-Denk-like Inclusions in Ovarian Fibromas: A Potential Degenerative Phenomenon Associated With Torsion. International journal of gynecological pathology : official journal of the International Society of Gynecological Pathologists. 2024 May 1:43(3):290-295. doi: 10.1097/PGP.0000000000000974. Epub 2023 Jul 18 [PubMed PMID: 37562060]
Level 2 (mid-level) evidenceKawasaki M, Shioya A, Takata M, Tsubata Y, Okanemasa Y, Takenaka M, Terauchi T, Yamashita M, Kumagai M, Yamada S. A case of bone metastasis of hepatocellular carcinoma: Mallory hyaline bodies can lead to the correct cytological diagnosis. Diagnostic cytopathology. 2023 Feb:51(2):E70-E74. doi: 10.1002/dc.25072. Epub 2022 Nov 8 [PubMed PMID: 36345980]
Level 3 (low-level) evidenceAigelsreiter A, Neumann J, Pichler M, Halasz J, Zatloukal K, Berghold A, Douschan P, Rainer F, Stauber R, Haybaeck J, Denk H, Lackner C. Hepatocellular carcinomas with intracellular hyaline bodies have a poor prognosis. Liver international : official journal of the International Association for the Study of the Liver. 2017 Apr:37(4):600-610. doi: 10.1111/liv.13325. Epub 2017 Jan 12 [PubMed PMID: 27885796]
Byrnes K, Bailey NT, Baral K, Mercer A, Joshi S, Wahby N, Rorison T, Liu G, Yin XM, Khambu B. Impaired hepatic autophagy exacerbates hepatotoxin induced liver injury. Cell death discovery. 2023 Feb 21:9(1):71. doi: 10.1038/s41420-023-01368-3. Epub 2023 Feb 21 [PubMed PMID: 36810855]
Denk H, Stumptner C, Zatloukal K. Mallory bodies revisited. Journal of hepatology. 2000 Apr:32(4):689-702 [PubMed PMID: 10782920]
Level 3 (low-level) evidenceBardag-Gorce F, Oliva J, Villegas J, Fraley S, Amidi F, Li J, Dedes J, French B, French SW. Epigenetic mechanisms regulate Mallory Denk body formation in the livers of drug-primed mice. Experimental and molecular pathology. 2008 Apr:84(2):113-21. doi: 10.1016/j.yexmp.2007.12.004. Epub 2008 Jan 11 [PubMed PMID: 18281034]
Level 3 (low-level) evidenceLivneh I, Cohen-Kaplan V, Cohen-Rosenzweig C, Avni N, Ciechanover A. The life cycle of the 26S proteasome: from birth, through regulation and function, and onto its death. Cell research. 2016 Aug:26(8):869-85. doi: 10.1038/cr.2016.86. Epub 2016 Jul 22 [PubMed PMID: 27444871]
Qian H, Ding WX. SQSTM1/p62 and Hepatic Mallory-Denk Body Formation in Alcohol-Associated Liver Disease. The American journal of pathology. 2023 Oct:193(10):1415-1426. doi: 10.1016/j.ajpath.2023.02.015. Epub 2023 Mar 9 [PubMed PMID: 36906265]
Level 2 (mid-level) evidenceShasthry SM, Rastogi A, Bihari C, Vijayaraghavan R, Arora V, Sharma MK, Sarin SK. Histological activity score on baseline liver biopsy can predict non-response to steroids in patients with severe alcoholic hepatitis. Virchows Archiv : an international journal of pathology. 2018 Apr:472(4):667-675. doi: 10.1007/s00428-018-2330-4. Epub 2018 Mar 7 [PubMed PMID: 29516163]
Harada M. Autophagy is involved in the elimination of intracellular inclusions, Mallory-Denk bodies, in hepatocytes. Medical molecular morphology. 2010 Mar:43(1):13-8. doi: 10.1007/s00795-009-0476-5. Epub 2010 Mar 26 [PubMed PMID: 20340001]
Level 3 (low-level) evidenceKe PY. Diverse Functions of Autophagy in Liver Physiology and Liver Diseases. International journal of molecular sciences. 2019 Jan 13:20(2):. doi: 10.3390/ijms20020300. Epub 2019 Jan 13 [PubMed PMID: 30642133]
Nikam A, Patankar JV, Somlapura M, Lahiri P, Sachdev V, Kratky D, Denk H, Zatloukal K, Abuja PM. The PPARα Agonist Fenofibrate Prevents Formation of Protein Aggregates (Mallory-Denk bodies) in a Murine Model of Steatohepatitis-like Hepatotoxicity. Scientific reports. 2018 Aug 28:8(1):12964. doi: 10.1038/s41598-018-31389-3. Epub 2018 Aug 28 [PubMed PMID: 30154499]
Oliva J, Bardag-Gorce F, Li J, French BA, Nguyen SK, Lu SC, French SW. Betaine prevents Mallory-Denk body formation in drug-primed mice by epigenetic mechanisms. Experimental and molecular pathology. 2009 Apr:86(2):77-86. doi: 10.1016/j.yexmp.2008.11.002. Epub 2008 Nov 24 [PubMed PMID: 19073172]
Level 3 (low-level) evidenceNeuman MG, Mueller J, Mueller S. Non-invasive Biomarkers of Liver Inflammation and Cell Death in Response to Alcohol Detoxification. Frontiers in physiology. 2021:12():678118. doi: 10.3389/fphys.2021.678118. Epub 2021 Jul 7 [PubMed PMID: 34305638]
Zhong B, Dong J, Zhang R, He M, Zeng W, Pan J, He J, Tao A, Yang R, Fu B, French SW, Liu H. Altered regulation of LncRNA analysis of human alcoholic hepatitis with Mallory-Denk Bodies (MDBs) is revealed by RNA sequencing. Experimental and molecular pathology. 2020 Dec:117():104559. doi: 10.1016/j.yexmp.2020.104559. Epub 2020 Oct 27 [PubMed PMID: 33121977]